INTRODUCTION
Stroke is the most prevalent cause of disability that impairs ambulation and the ability to perform the activities of in daily living (ADL) [1,2]. The common deficits following stroke are lower limb impairment and postural imbalance, and these can significantly impact physical ability and health [3,4]. Balance control is defined as the ability to maintain the body's movement and to perform an activity or action within the base of support without falling. It combines sensory and motor skills, and requires integration of sensory input and planning and execution of movement patterns that are necessary to control the center of body mass [5,6,7]. These functions are impaired in stroke patients, resulting in frequent falls, impaired gait and impaired ability to perform the ADL after a stroke. Previous studies have reported reduced loading on the paretic lower limb and increased postural sway during static standing in stroke patients [8,9].
The ability to evaluate balance and predict recovery of balance after a stroke may help in planning rehabilitation. Several clinical and demographic factors, including the severity of initial neurological deficit, lesion size, lesion location and age, have been suggested as predictors of recovery after stroke [10,11]. Evoked potentials (EPs) provide an objective and direct method by which to assess the integrity of sensory and motor pathways of the central nervous system [12]. Evoked potential can also predict recovery after stroke [12]. Motor evoked potentials (MEPs) [3,13,14,15,16,17,18,19,20] and somatosensory evoked potentials (SSEPs) [7,21,22,23,24,25,26] are reliable indicators of post-stroke prognosis. However, most of the studies that have quantified the prognostic value of MEPs and SSEPs have focused on motor and functional recovery of the upper limb. Although a few studies have investigated lower limb function [3,21,23], these studies have not evaluated balance well. In addition, only a few reports have evaluated MEPs and SSEPs simultaneously [27,28,29,30].
Therefore, the aim of this study was to investigate the association between baseline MEP and SSEP responses in the lower extremity and balance recovery and whether baseline MEP and SSEP responses are beneficial in predicting balance recovery after rehabilitation in subacute hemiparetic stroke patients.
MATERIALS AND METHODS
Subjects
Twenty patients (seven males and 13 females) with subacute cortical stroke (i.e., within three months of stroke onset) were recruited from the patients admitted to our hospital. Stroke was confirmed clinically through computed tomography scans or magnetic resonance imaging. Inclusion criteria were the ability to stand for at least one minute without assistance and the ability to understand simple oral instructions given by a physical therapist. Exclusion criteria were previous symptomatic strokes, severe cognitive impairment or aphasia (determined by clinical evaluation with a physiatrist), presence of neglect, psychological disorder, uncontrolled medical diseases, significant orthopedic or pain conditions that limited participation in balance testing, peripheral polyneuropathy identified by nerve conduction, and contraindications for transcranial magnetic stimulation, such as a history of epileptic seizure, a history of major head trauma, the presence of metal in the skull, or a pacemaker. All participants received four weeks of conventional rehabilitation consisting of physical and occupational therapies focused on mobility and ADL functions. The protocol was reviewed and approved by the Institutional Review Board, and all subjects provided written informed consent before the selection procedure.
Neurophysiologic assessment
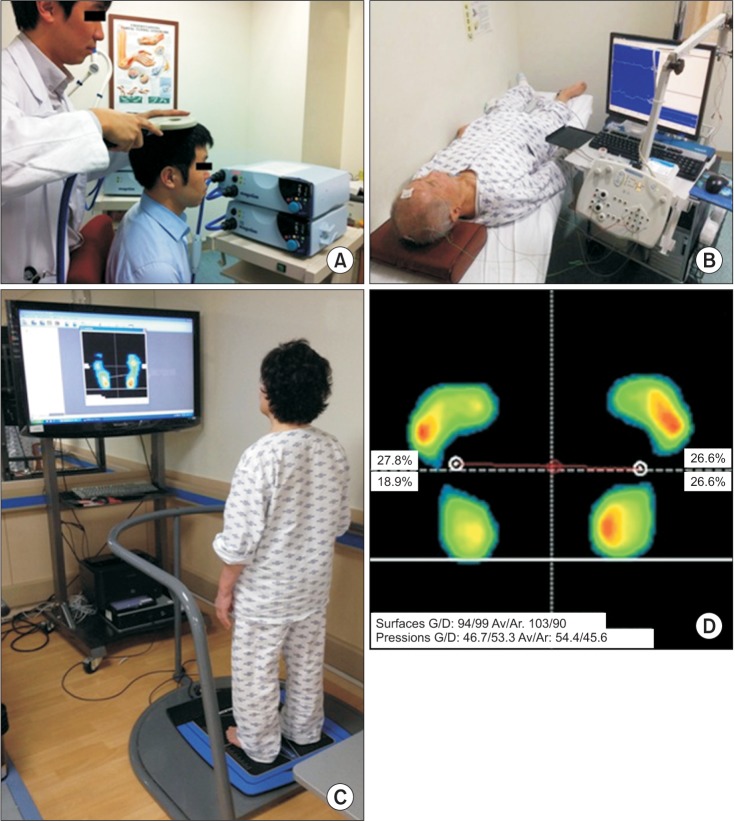
MEPs and SSEPs were measured before rehabilitation (baseline) using Magstim 200 (Magstim, Dyfed, UK) and an electromyogram (Medelec Synergy, Oxford, UK). MEPs were evoked by transcranial magnetic stimulation delivered through a 70-mm radius-round coil (Fig. 1A). The active electrode was placed on the skin over the tibialis anterior muscle of the paretic lower limb and the reference electrode was placed on the skin over the tibialis anterior muscle tendon. The center of the coil was placed on the scalp over the parietal region of the brain contralateral to the paretic lower limb. The coil was moved in 1-cm intervals and, at each location, the stimulus intensity was increased in 2%-steps from 50% of maximum stimulator output to 100% of maximum stimulator output. The minimum stimulus intensity that evoked a response in the tibialis anterior muscle was Ōēź50 mV on more than five out of 10 occasions and this minimum intensity was defined as the resting threshold [30,31]. If a resting threshold was identified, the patient was classified as MEP-positive, MEP (+). If no resting threshold was identified at any location, the patient was classified as MEP-negative, MEP (-).
SSEPs were evoked by electrical stimulation of the posterior tibial nerve at the ankle of the lower limbs (Fig. 1B). The stimulus strength was adjusted to produce minimal twitches in the muscles. The stimulus rate was 4 Hz and the stimulus duration was 0.2 ms. At least two traces of 250 averaged responses were recorded. Responses were recorded by an active electrode placed on the midline of the scalp 2 cm behind Cz, with a reference electrode placed at the midfrontal point (Fpz) according to the international 10-20 system [30,32]. If there was a response to stimulation of the posterior tibial nerve on the paretic side, the patient was categorized as SSEPs-positive, SSEPs (+). If there was no response to stimulation of the posterior tibial nerve on the paretic side, the patient was categorized as SSEPs-negative, SSEPs (-).
Outcome measures
Balance, motor and ADL functions were assessed before and after four weeks of rehabilitation.
Balance
Patients were evaluated for balance ability using the BioRescue (RM Ingenierie, Rodez, France) static posturography and Berg Balance Scale (BBS). BioRescue static posturography was evaluated using force plates that measured the vertical pressure fluctuations of the toes and heels of both feet. The subject stood on the force plates with bare feet without holding the support bar, and the vertical pressure fluctuations were measured, amplified and filtered before being recorded for analysis (Fig. 1C, D). Balance was quantified using weight distribution indices, namely weight distribution index-surface area (WDI-Sa) and weight distribution index-pressure (WDI-Pr), and stability indices, namely stability index-surface area (SI-Sa) and stability index-length (SI-L). Weight distribution indices (WDIs) checked with the ratio of the paretic side to the intact side. Ideal posture occurs when the subject's weight is distributed equally across the two feet, and the WDI is 1.00. However, stroke patients often have reduced loading on the paretic lower limb [8,9], indicated by WDIs less than 1.00. As WDIs approach 1.00, balance is more stable. The stability indices indicate the horizontal and vertical postural sway of center of pressure over a 30-s period. The higher the stability index becomes, the more unstable the posture. All static posturography parameters were evaluated during eyes open (EO) and eyes closed (EC) conditions.
BBS is a widely used clinical test of a static and dynamic balance [33]. It assesses the performance of 14 functional tasks and assigns a score ranging from zero to four points for each task. The total scores ranges from zero to 56 points, with higher scores indicating greater balance and functional independence. The Korean version of the BBS has been validated and was used in this study [34].
Motor function
The Fugl-Meyer Assessment (FMA) is a stroke-specific, performance-based impairment index that assesses motor function, balance, sensation, joint function and pain in patients with post-stroke hemiplegia. It consists of 155 items and each item is rated on a three-point ordinal scale (0, cannot perform; 1, perform partially; and 2, perform fully). The motor domain includes 50 items that assess movement, coordination and reflexes, and has a maximum score of 66 points for the upper extremities and 34 points for the lower extremities. The FMA score for the lower extremities was used to evaluate motor function in this study.
ADL function
The Modified Barthel Index (MBI) is a reliable and valid instrument for measuring the functional status of stroke patients, and indicates the degree of independence of a patient in terms of the patient's need for any assistance. It assesses the patient's performance in 10 daily activities, such as personal hygiene, bathing, feeding, toileting, climbing stairs, dressing, bowel control, bladder control, ambulation and transfer. It assigns a score ranging from zero to 15 points for every variable, and the maximum score is 100. The Korean version of the MBI (K-MBI) has been validated [35] and was used to evaluate ADL function in this study.
Statistical analysis
All statistical analyses were performed using IBM SPSS for Windows ver. 20.0K (IBM Co., Armonk, NY, USA). To test whether the subjects' results fell on a normal distribution, the Shapiro-Wilk normality test was introduced. Since the normality assumption was not satisfied and the sample size was small, we used the non-parametric test to perform the analysis. Baseline demographic and clinical characteristics were compared across MEP (+) and MEP (-) groups and across SSEP (+) and SSEP (-) groups using a Mann-Whitney test for continuous data and chisquare tests for categorical data. A Wilcoxon signed-rank test was used to compare the change in a variable within each group at the start and after four weeks of rehabilitation. The difference between the change in this variable between the two groups was compared using the Mann-Whitney test. All p-values <0.05 were considered statistically significant.
RESULTS
Demographic and clinical characteristics
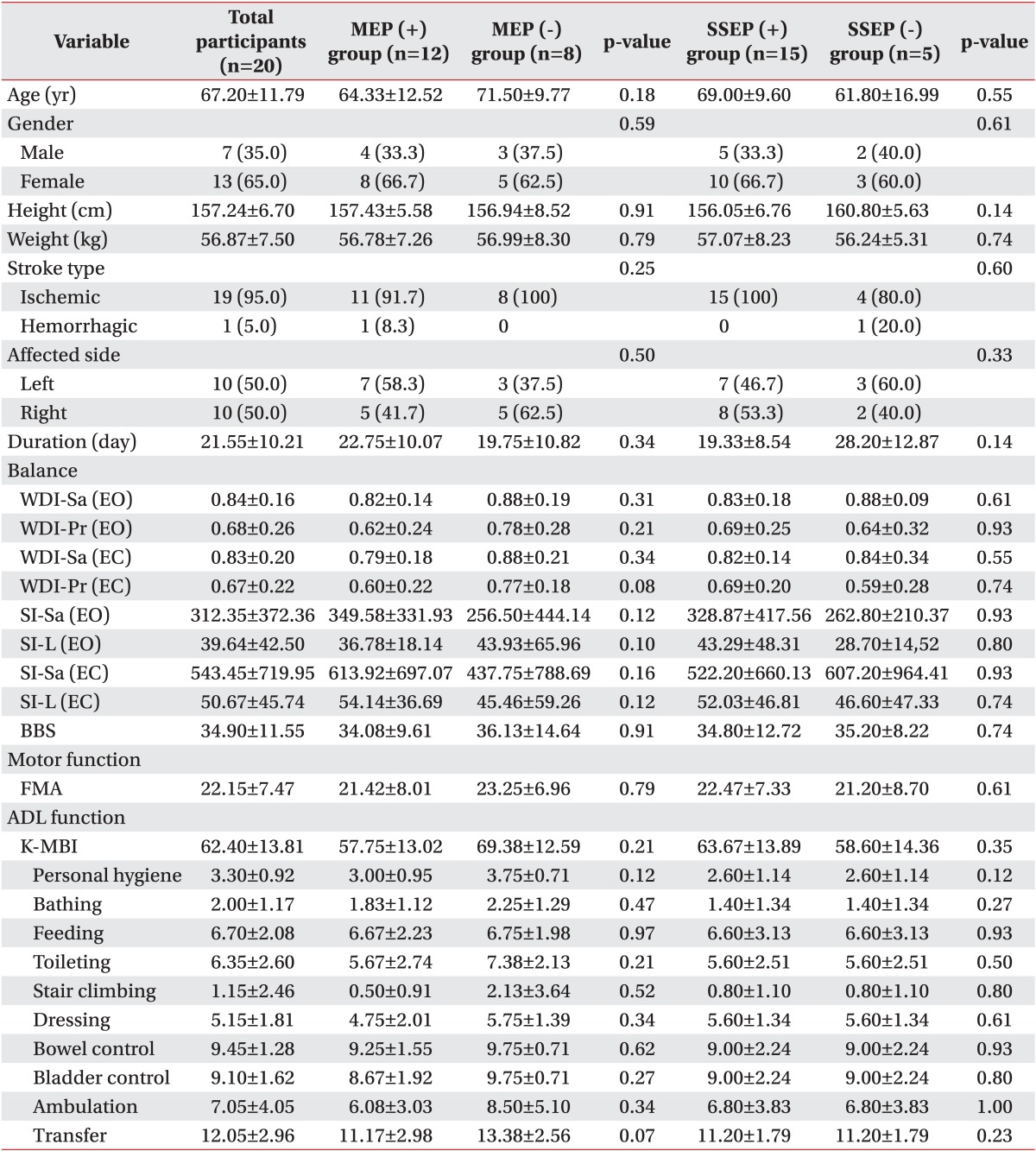
Baseline demographics and clinical characteristics are shown in Table 1. A total of twenty subjects (seven males and 13 females) participated in this study. The average age of the patients was 67.20┬▒11.79 years, and the average post-stroke duration was 21.55┬▒10.21 days. Demographic characteristics, including gender, age, height, weight, stroke type (ischemic and hemorrhagic), affected side (right and left), and the duration of time between the stroke and the first evaluation were not significantly different in terms of the EP responses. In addition, in the comparison of evaluation items including balance, motor function and ADL function in terms of EP responses that were tested before rehabilitation, there were no significant differences between the two groups. No participants in either group experienced a serious adverse event during the study period.
In the comparison of balance, motor and ADL functions in terms of EP response at the start and after four weeks of rehabilitation within the group
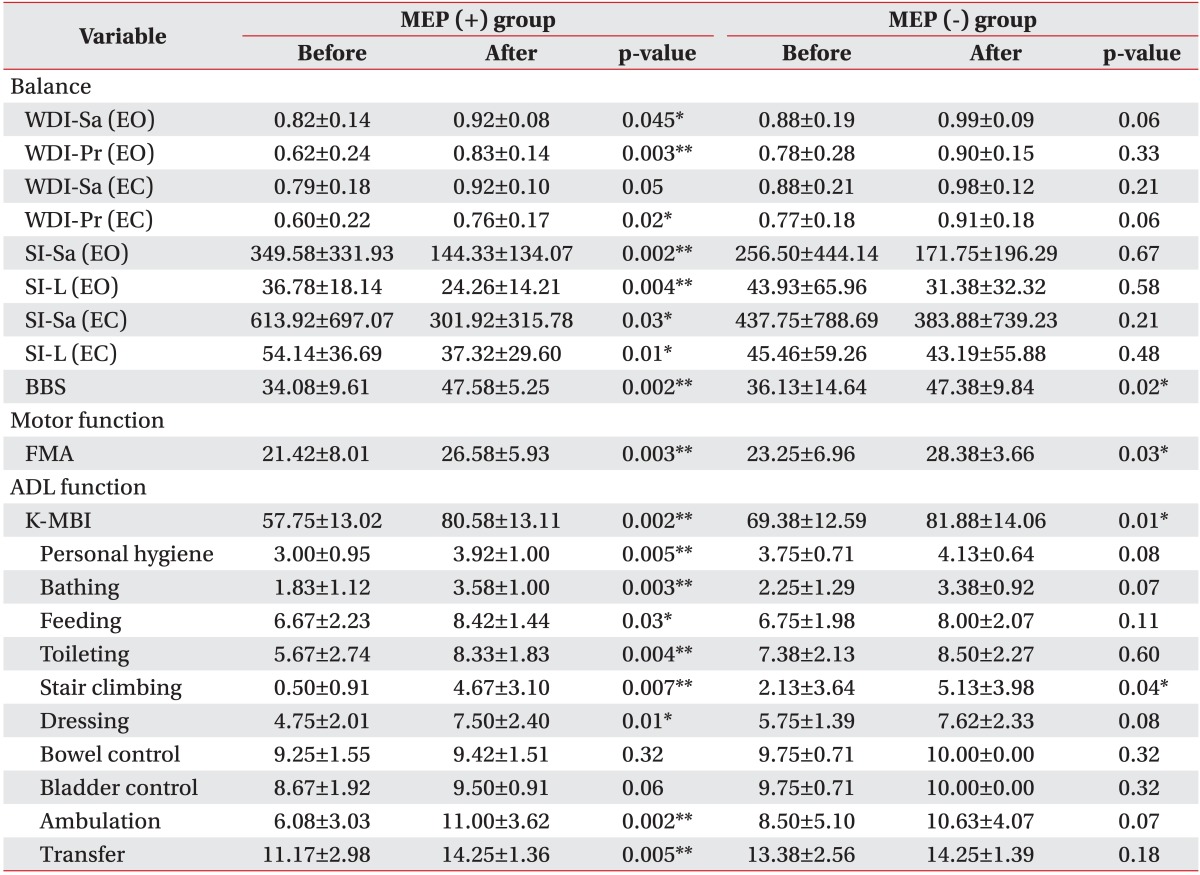
The MEP (+) group showed significant improvements in the posturography parameters, BBS, FMA, total K-MBI and K-MBI subscales except WDI-Sa (EC), bowel and bladder control, while the MEP (-) group showed only significant improvements in the BBS, FMA, total K-MBI and stair climbing in the K-MBI subscales after rehabilitation when compared to the results before treatment (Table 2).
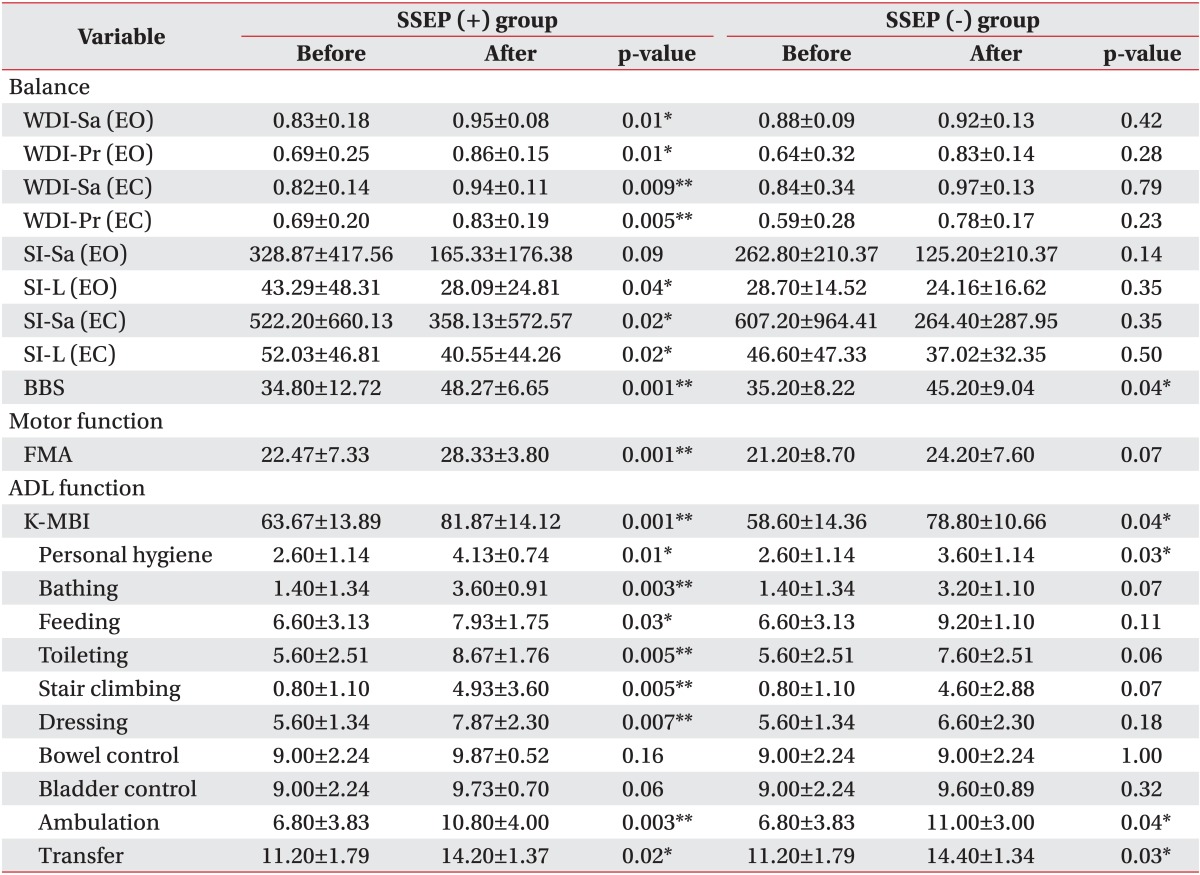
The SSEP (+) group showed significant improvements in the posturography parameters, BBS, FMA, total K-MBI, and K-MBI subscales except SI-Sa (EO), bowel, and bladder control, while the SSEP (-) group showed only significant improvements in the BBS, total K-MBI and personal hygiene, ambulation, and transfer in the K-MBI subscales after rehabilitation when compared to the results before treatment (Table 3).
In the comparison of the changes of balance, motor and ADL functions in terms of EP responses at the start and after four weeks of rehabilitation between groups
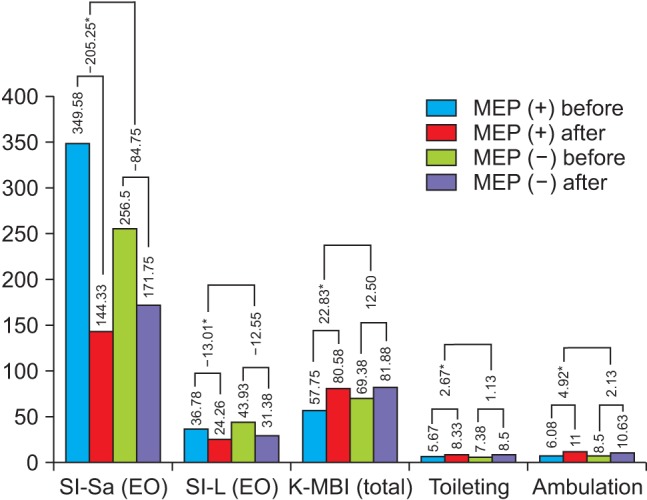
When comparing the changes of balance, motor and ADL functions before and after treatment between the MEP (+) group and MEP (-) group, the SI-Sa (EO) (-205.25┬▒287.09 vs. -84.75┬▒396.94, p=0.03), SI-L (EO) (-13.01┬▒9.13 vs. -12.55┬▒45.06, p=0.03), total K-MBI (22.83┬▒7.58 vs. 12.50┬▒6.76, p=0.01) and toileting (2.67┬▒1.72 vs. 1.13┬▒1.25, p=0.047) and ambulation (4.92┬▒2.23 vs. 2.13┬▒2.80, p=0.04) in the K-MBI subscales showed significant improvements in the MEP (+) group compared to the MEP (-) group. However, there was no significant difference in the changes of balance, motor, and ADL functions between SSEP (+) group and SSEP (-) group (Fig. 2).
DISCUSSION
The main finding of this study was that baseline MEPs and SSEPs responses were significantly associated with balance recovery after four weeks of rehabilitation in subacute hemiparetic stroke patients. In particular, patients with a baseline MEP response showed more significant improvements in terms of their static balance ability and functional status including ADL subitems correlated with balance ability after rehabilitation than patients without a baseline MEP response.
Several studies have reported the predictive value of MEPs and SSEPs for post-stroke functional recovery. Most of these studies have focused on muscular strength or functional ability of the upper extremities. Pizzi et al. [15] reported that patients with a baseline MEP response had better functional recovery (assessed using the Medical Research Council scale score and the Barthel Index) at 12 months post-stroke than patients without a baseline MEP response. Lim et al. [16] reported that the improvement in ADL function, particularly the self-care dimension of the Functional Independence Measure, after four weeks of rehabilitation was greater in patients with a baseline MEP response than in patients without a baseline MEP response. Al-Rawi et al. [7] showed that, among the SSEP parameters, the N20-P25 amplitude had a positive correlation with motor recovery of the upper limb in patients who had had strokes. Although they only evaluated the prognostic value of median SSEPs for motor and functional recovery of the upper extremity, they proved the effectiveness of EPs in predicting the overall functional recovery of patients who had had strokes.
In contrast to these studies, we analyzed the predictive value of MEPs and SSEPs for the recovery of lower limb functions, especially balance. Our results showed that patients with a baseline MEP response had better balance recovery after four weeks of rehabilitation than patients without a baseline MEP response. This may be due to the location of the generators of evoked potentials. In our patients, the majority of lesions involved the middle cerebral artery territory, and the injury of pathways to the motor cortex had led to a loss of MEPs. Only a few other studies have assessed the prognostic value of lower-extremity MEPs for motor recovery of the lower extremity and the ability to ambulate after stroke. Hendricks et al. [3] showed that MEPs in the tibialis anterior muscle provided important prognostic information on the motor recovery of muscles and the ability to perform independent transfer.
Our results also showed that patients with a baseline SSEP response had better balance recovery after four weeks of rehabilitation than patients without a baseline SSEP response. Similarly, Tzvetanov et al. [23] reported that the absolute amplitude of the P40 component of SSEPs elicited by stimulation of the posterior tibial nerve had a moderately strong correlation with the Barthel Index and Rankin Scale three months after a stroke. The authors mentioned that SSEP impairment reflects not only the involvement of the sensory system, especially proprioceptive structures, but also damage to motor areas, as sites of cortical generators of SSEPs overlap with the primary motor zone.
Importantly, we evaluated MEPs and SSEPs simultaneously, and found that a presence of MEPs and SSEPs response at the start was a good indicator of balance recovery after a stroke. Only a few studies evaluated both MEPs and SSEPs at the same time and showed mixed results [27,28,29,30]. Kim et al. [27] reported that MEPs in tibialis anterior was useful in predicting mobility and SSEPs were a predictive indicator for ADL after a stroke. Lee et al. [28] reported that only patients with baseline MEP and SSEP responses in the lower limbs had good functional recovery, and that baseline MEP responses had a higher specificity, but this was not significant in the SSEP study. Pereon et al. [29] reported that a baseline MEP response had a predictive value for functional outcomes, but a baseline SSEP response and sympathetic skin response did not. Lee et al. [30] also reported that baseline MEP and SSEP responses had a stronger correlation with the manual function test score. As mentioned in our study and previous reports, combining the predictive information from MEPs and SSEPs could be more effective and interrelated than either MEPs or SSEPs alone.
In addition, our study showed that the changes in some posturography parameters, total K-MBI and K-MBI subscales related to the ability to balance, which is evident in activities such as toileting and ambulation. These changes were significantly larger after four weeks of rehabilitation in patients with a baseline MEP response than patients without a baseline MEP response. This means that out of the ADL toileting and ambulation required better balance than other K-MBI subscales. These results have an important clinical implication for planning and execution of an acute rehabilitation program in that an EP response, especially baseline MEP response, is a meaningful predictive factor of the recovery of static balance and the ability to perform ADL correlated with the ability to maintain dynamic balance.
To the best of our knowledge, this is the first study to assess the predictive value of lower-extremity MEPs and SSEPs for balance evaluated using posturography. Although there are other clinical tools that can be used to evaluate balance, it is a highly likely that they are subjectively influenced by examiners or subjects, and it is difficult to evaluate quantitatively changes in balance using these tools [36]. By contrast, posturography is highly sensitive, quantitative, and is not affected by physical indices, such as body weight or height.
In addition, because posturography assesses static balance ability, and clinical tools such as BBS or K-MBI assess static and dynamic balance abilities, combining the assessment of balance from posturography and clinical tools could be helpful in evaluating the ability to balance in various aspects. Therefore, like in our study, the combined assessment of posturography and clinical tools, such as BBS and K-MBI, could be beneficial in detecting the recovery of balance for subacute hemiparetic stroke patients.
There are several limitations to the present study. Firstly, the sample size in each group was small because we enrolled patients who only had cortical infarction or hemorrhage. This meant that we could not analyze according to the location and size of the strokes, and these variables may have influenced the functional outcome. Secondly, the average post-stroke duration of our patients (21.55┬▒10.21 days) and the duration of the follow-up period (four weeks) were insufficient to assess recovery of functional ability. Physiological recovery of the injured tissue is generally completed about three months after the onset of a stroke; therefore, pathophysiological processes in addition to direct tissue damage, such as cortical irritation and cortical depression, may have influenced our data. Accordingly, we suggest that future studies examine the long-term relation between MEP and SSEP responses and functional ability. Thirdly, we dichotomized the baseline evoked potential responses and divided patients into two groups according to the presence or absence of an evoked potential response. This was done because the normal physiologic variability of SSEP parameters (latency, spine-to-scalp sensory central conduction time, peak-to-peak amplitude, side-to-side amplitude) is large, and our sample size was small. Fourthly, the change of several dependent variables, especially WDI, might be limited by a ceiling effect. Participants of MEP (+) groups were more than those of MEPs (-) group, and participants with higher baseline variables in MEP (-) group may already have had a relatively better ability to balance to start with, so, the change was less than in the MEP (+) group. Therefore, future studies of more participants are warranted to confirm our findings and reveal a meaningful difference between the two evoked potentials. Finally, we could not include a nonrehabilitation control group for ethical reasons; therefore, we do not know whether the improvement in function was the result of rehabilitation or natural recovery after a stroke.
In conclusion, we demonstrated that baseline MEPs and SSEPs responses were significantly associated with balance recovery after 4 weeks' rehabilitation in subacute hemiparetic stroke patients. These findings suggest that initial combined assessments of MEPs and SSEPs might be of benefit for predicting balance recovery in subacute hemiparetic stroke patients.