INTRODUCTION
The pronator quadratus (PQ) muscle arises from the oblique ridge on the anterior surface of the distal fourth of the ulna and inserts on the lateral border and anterior surface of the distal fourth of the radius. This muscle is a deep-seated, short, flat quadrilateral muscle with parallel running fibers [1]. The PQ muscle receives the final branch of the anterior interosseous nerve (AIN) and is the key muscle used in the electrophysiologic diagnosis of AIN lesions.
The function of the PQ is forearm pronation. In the management of pronator spasticity in stroke patients, the injection of neurolytic agents such as phenol or alcohol into the motor point of the PQ may be useful. Motor point block must be achieved at an accurate location to enhance the efficacy of treatment [2].
Because the PQ muscle is the deepest muscle in the forearm and can be neither palpated nor observed [3], the proper approach to this muscle is challenging. Previously suggested points for needle insertion vary depending on the study [4,5]. Therefore, accurate anatomic knowledge is also important for clinicians who inject neurolytic agents to treat forearm spasticity or in needle electromyography to evaluate this muscle.
Few studies have investigated the location of the PQ muscle and its motor points. The purpose here was to use cadaver dissection to accurately locate the PQ muscle and the motor point of this muscle relative to anatomic landmarks.
MATERIALS AND METHODS
Subjects
For this study we dissected 20 limbs from 10 fresh cadavers (9 males and 1 female). After each cadaver was placed supine in the anatomic position, the skin and subcutaneous tissue were dissected from the mid-forearm, exposing the entire PQ muscle. After the flexor digitorum profundus and flexor pollicis longus tendons were cut, the origin and insertion sites of the PQ muscle and the AIN were visualized.
Methods
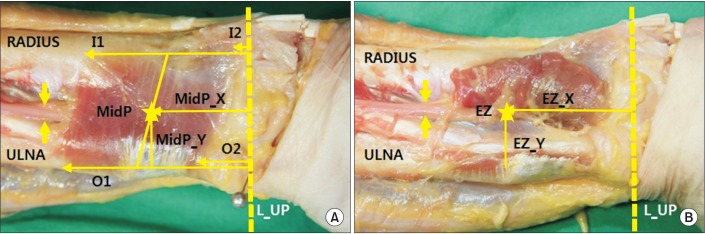
We measured the relative distances to the origin and insertion of the PQ muscle from an imaginary vertical line (L) passing the tip of ulnar styloid process (L_UP). Measurements were also made of the proximal and distal origin sites (O) of the PQ muscle on the ulna (O1 and O2, respectively) and of the proximal and distal insertion sites (I) of the PQ muscle on the radius (I1 and I2, respectively) (Fig. 1A).
The midpoint of the PQ muscle (MidP) was determined using the origin and insertion sites of this muscle. An imaginary line was drawn from the half point between O1 and O2 to the half point between I1 and I2, and the center point of the imaginary line was considered the MidP. In addition, we measured the distances from MidP to the ulnar styloid process (MidP_X) and to the medial border of the ulna (MidP_Y) (Fig. 1A).
The entry zone (EZ) was defined as the center of the site where the AIN entered the belly of the PQ muscle, and the AIN had three to five branches around the EZ. We measured the distance from the L_UP to the EZ of the AIN and the distance from the medial border of the ulna to the EZ of the AIN (EZ_X and EZ_Y, respectively) (Fig. 1B).
Each of the X-values and Y-values of the EZ and MidP (EZ/FL and MidP/FL, respectively) were also calculated as a percentage of the forearm length (FL) and the wrist width (WW). FL was defined as the length from the tip of the ulnar styloid process to the medial epicondyle. WW was measured as the length of muscle margin from ulna to radius.
Statistical analysis
Median and range values were determined, as appropriate. The Kolmogorov-Smirnov test verified the normality of the distribution of variables. The Wilcoxon signed-rank test was used to determine the differences in X-values and Y-values of EZ and MidP. The intraclass correlation coefficient was calculated for the agreement of X-values and Y-values and considered to be strong if the correlation coefficient was >0.8. All statistics were two-tailed, and differences with p-values of <0.05 were considered significant. All statistical analyses were performed using SPSS software ver. 14.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
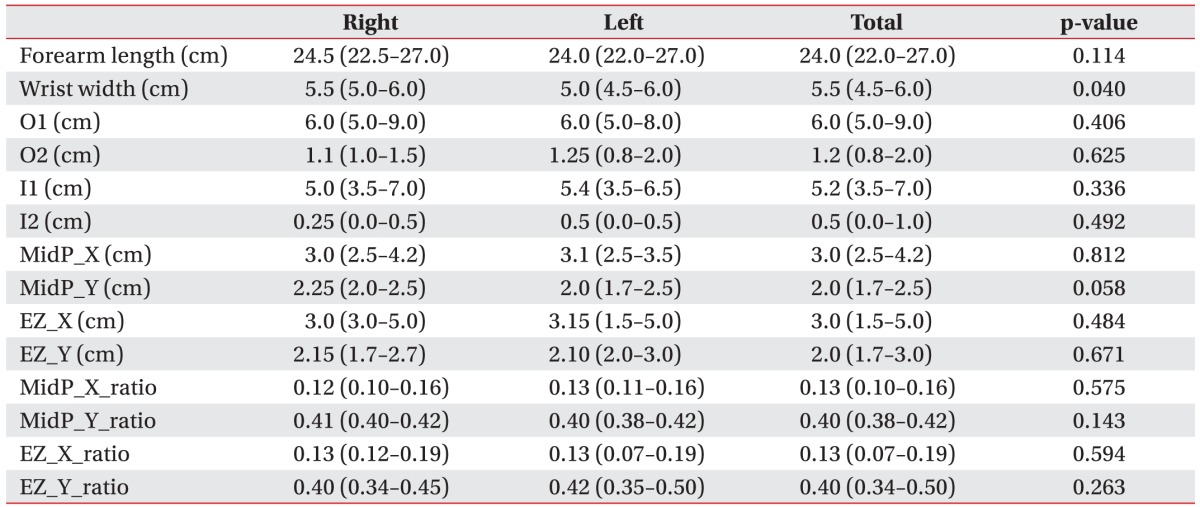
Table 1 shows the medians and ranges of the measurements. There was no side-to-side difference for each of the values in this study.
The PQ muscle was located in the distal forearm just above the wrist joint: distances of the median proximal origin and insertion sites from L_UP were 6.0 cm and 5.2 cm, respectively, and distances of the median distal origin and insertion sites from L_UP were 1.2 cm and 0.5 cm, respectively.
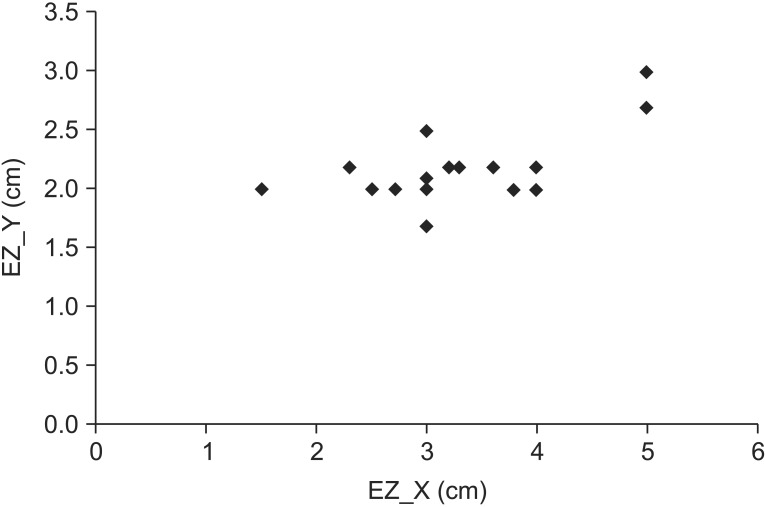
The MidP was measured as 3.0 cm (range, 2.5–4.2 cm) proximal to the L_UP (MidP_X) and 2.0 cm (range, 1.7–2.5 cm) lateral to the medial border of the ulna (MidP_Y). The EZ of the AIN to the PQ muscle was located 3.0 cm (range, 1.5–5.0 cm) proximal to the L_UP (EZ_X) and 2.0 cm (range, 1.7–3.0 cm) lateral to the medial border of the ulna (EZ_Y). Plot of the locations of entry zone (EZ) in the pronator quadratus muscle muscle is shown in Fig. 2.
The median MidP/FL ratio was 0.13 (range, 0.10–0.16), and the median EZ/FL ratio was also 0.13 (range, 0.07–0.19). The median MidP/WW ratio was 0.40 (range, 0.38–0.42), and the median EZ/WW ratio was also 0.40 (range, 0.34–0.50), indicating that the relative location of the muscle and the motor point was distal 13% of the FL and was distal 40% of the ulnar side of the WW. There was no significant difference between the location of the EZ and MidP in the PQ muscle.
DISCUSSION
Accurate knowledge of the PQ muscle is important, especially when performing electrodiagnostic studies to detect an AIN lesion. The diagnosis of AIN lesions is established by means of nerve conduction studies and needle electromyography of the PQ muscle [6]. The motor point is considered to be an optimal site for the active recording electrode in AIN conduction studies or for the injection of neurolytic agents such as botulinum toxin, alcohol, or phenol to reduce pronator spasticity. However, inserting a needle in the PQ muscle is not easy because of its deep location. Therefore, cadaver dissection to identify the actual location of the PQ muscle and its motor point is very important.
Many authors have described the anatomic location of the PQ muscle and have recommended needle insertion sites for electrodiagnosis. Moore et al. [3] described its position as the muscle attached to the distal fourth of the radius and ulna. Jenkins [7] also referred to it as the muscle that is attached from the distal fourth of the ulna to the distal part of the radius. However, these descriptions are too broad for electromyographers or physicians to identify the needle insertion points precisely.
Lee and DeLisa [4] defined the needle insertion point of the PQ muscle in more detail—that is, close to the anterior surface of the ulna, 2 to 3 cm proximal to the ulnar styloid on the forearm in the supinated position, or cleft between the layers of extensor tendons over the dorsal aspect of the distal forearm (distal fourth between the lateral epicondyle and the ulnar styloid) on the forearm in the pronated position. Perotto et al. [5] described the needle insertion point as three fingerbreadths proximal to the midpoint of a line connecting the radial and ulnar styloids; however, use of this method of measurement might be inaccurate because of individual variations in fingerbreadth according to such factors as race, sex, height, and body mass index. Therefore, we used centimeters to measure each point more accurately.
As mentioned above, authors have described the needle insertion point of the PQ in many different ways. In our results, the accurate location of the PQ muscle for proper needle insertion was 3 cm proximal to the ulnar styloid process or the distal 13% of the FL. This result reveals a more distal point than a fourth of the forearm, as described in the studies just referred to.
The motor point of a muscle has been defined as the entry point of the motor nerve branch into the epimysium of the muscle belly [8]. The number, location, and distribution of motor points are variable. According to Safwat and Abdel-Meguid [9], the PQ muscle is supplied by the motor branches along its whole length. However, Svizenska et al. [10] observed three types of AIN branching patterns: gradual branching, terminal branching, and terminal branches that continue to the wrist joint. Sakamoto et al. [11] also noted that the AIN divided into three or four branches and entered the posterior surface of the PQ muscle and became distributed in various patterns. In our study, EZ was defined as the center of the site where the AIN entered the belly of the PQ muscle and split into several branches.
In nerve conduction studies, surface recordings provide the most important information because an amplitude is obtained. The optimal compound motor action potential could be recorded with the least intense stimulation when the recording electrode is located at the motor point. Oh [12] described an AIN motor conduction study using a needle recording electrode at the PQ muscle, although the specific location was not explained. Shafshak and El-Hinawy [13] used the surface recording technique and found it to be more clinically useful than needle recording from this muscle. Foley et al. [14] also used the surface recording technique: the active electrode was placed on the midpoint between the radius and the ulna on the dorsal forearm, 3 cm proximal to the ulnar styloid process, while the reference electrode was placed over the radial styloid [15]. Our finding that the EZ of the AIN to the PQ muscle was located 3 cm proximal to the ulnar styloid process could support the nerve conduction study technique mentioned above.
Compared with our study, previous reports have demonstrated more proximal points for the motor point of the PQ muscle. Lin et al. [16] reported that the median distance of the motor branches of AIN from the wrist to the PQ was 4.54 cm. Svizenska et al. [10] reported that the median distance of the origins of muscular branches from the AIN trunk to the wrist joint was 4 cm (range, 2–8 cm). According to Alves et al. [17], the mean point of penetration of AIN branches to the PQ muscle was 3.6 to 3.9 cm above the wrist articular line. But our study revealed that the EZ of the motor branch is located 3.0 cm (range, 1.5–5.0 cm) proximal to the L_UP or distal 13% of the FL. Because the height and FL differ among different races, the motor point could also be different. There is no previous study concerning the motor point of the PQ muscle in Asia, suggesting that the actual EZ of the PQ in Asian is located more distal than prior studies have reported.
Earlier studies about the needle insertion site or the motor point of the PQ muscle demonstrated the length from the ulnar styloid process to each point. We also analyzed the relativity between the points and the WW and suggest that the accurate site for the needle insertion or motor point is similarly located at the distal 13% of the FL and at the ulnar 40% of the WW.
When physicians insert the needle at the site we mentioned or at a more proximal site, nerve injury is possible. To avoid AIN injury during needle electrodiagnostic studies, we suggest a PQ needle site that is 3 cm proximal to the ulnar styloid process or slightly distal to the point. If physicians insert a needle more proximally than the motor point, the risk of injury to the AIN might increase.
This study has a few limitations. First, the number of dissected forearms (20) from 10 fresh cadavers was small and too limited to assess the relation to individual characteristics. More cadaveric studies could suggest that this anatomic point is more accurately related to individual characteristics. Second, the EZ of the AIN does not exactly reflect all the motor points to the PQ muscle. Further cadaveric studies, including the numbers and bounds of motor branches from the EZ, could supplement these findings. Also, additional studies involving ultrasonographic examination could be useful for more accurately localization of the PQ muscle and the EZ of the AIN.
The present study demonstrated the exact anatomic location of the PQ muscle and the EZ of the AIN relative to the PQ muscle. The results are expected to facilitate precise localization of the muscle and the EZ and offer a more accurate approach for needle electromyography and motor point blocks of this muscle. The optimal site for needle electromyography and motor point blocks of the PQ muscle is 3 cm proximal to the ulnar styloid process or the distal 13% of the FL and 2 cm lateral to the medial border of the ulna or the ulnar 40% side of the WW.