INTRODUCTION
Spinal cord injury (SCI) involves damage to the spinal cord that causes temporary or permanent changes in its function. SCIs significantly alter every aspect of a personŌĆÖs life, usually irreversibly [1ŌĆō3]. Pediatric SCI (PedSCI) is further complicated by issues related to ongoing physical and emotional growth. After PedSCI, there is approximately a 50%ŌĆō83% reduction in life expectancy [4]. In addition, given the early occurrence, individuals with PedSCI require substantially long-term care than adults with SCIs [5]. PedSCI have a large proportional composition of cervical SCI than an adult due to different vertebral configuration, incomplete ossification, relatively larger head size, and more ligamentous laxity [6]. Moreover, the socioeconomic burden of PedSCIs is greater when considering disability-adjusted life years as an endpoint [7].
PedSCI is rare compared to adults and the incidence rate of PedSCI has been studied at 0.9ŌĆō27 per million per year in Europe and 14.8ŌĆō20 cases per million per year in the United States [5]. A low incidence and prevalence may result in varied experiences in treatment and a low priority for the development of related research and care programs. In the United States, annual data on SCIs are systematically published by the National Spinal Injury Statistical Center (NSCISC) [8]. However, there are few national spinal injury statistics on PedSCIs in South Korea. There are few previous studies that focused on the PedSCI [9]. Therefore, this study aimed to investigate the characteristics of PedSCI in South Korea, along with its etiology and related demographic characteristics of affected individuals, and to identify prevention strategies to reduce the incidence of PedSCI.
MATERIALS AND METHODS
The Ethics Committee of the Institutional Review Board of the National Rehabilitation Center (NRC) in South Korea approved this study (No. NRC-2019-04-025). The requirement for informed consent was waived owing to the studyŌĆÖs retrospective design.
Pediatric individuals with SCIs aged <20 years admitted to the NRC from 1990 to 2019 were enrolled. A total of 4,951 who were hospitalized with SCI were identified. Of these, 267 pediatric individuals were enrolled in this study after excluding the following: those aged Ōēź20 years at the time of onset (n=4,076), those who were re-admitted (n=318), those with onset dates before 1990 (n=149), and those with unknown onset date or incomplete data (n=141).
Individual data on sex, admission data, age of onset, cause of injury (injury etiology), American Spinal Injury Association impairment scale (AIS) score [10], and neurological information on the degree of impairment were collected. The neurological level of injury and the degree of impairment after the injury were assessed by a physician. In most cases, examinations had been performed during the first week after admission. The etiologies of traumatic SCI (TSCI) and non-traumatic SCI (NTSCI) were classified according to international SCI datasets [11,12]. TSCIs were classified as those caused by land transport accidents, falls, violence, sports, and others, including iatrogenic causes and in those cases where objects fell on the spine. NTSCIs were classified as those caused by neoplasm, inflammation, infection, degeneration, vascular issues, and others including syringomyelia and meningomyelocele. To identify age-related differences, the individuals were classified into the following age groups according to the International Spinal Cord Injury Data Set [11]: Ōēż5 years, 6ŌĆō12 years, 13ŌĆō14 years, 15ŌĆō17 years, and 18ŌĆō19 years.
All statistical analyses were performed using IBM SPSS Statistics for Windows, version 26 (IBM Corp., Armonk, NY, USA). Pearson chi-square test was used to compare categorical data, and statistical significance was set at p<0.05.
RESULTS
General characteristics
According to the cause of injury, 216 individuals had TSCIs and 51 had NTSCIs. The mean┬▒standard deviation onset age of SCI in all study individuals was 15.7┬▒4.5 years. Most individuals were 15ŌĆō19 years old (79.8%). The most common age at injury of TSCI and NTSCI was 19 years (n=64) and 14 years (n=9), respectively. There was a significantly higher male-to-female ratio in the TSCI group (Žć2=10.603; p<0.05) (Table 1).
Traumatic spinal cord injuries
Among the patients with traumatic spinal cord injury patients admitted to the NRC during the 1990ŌĆō2019 period, 6.3% were aged <20 years. The mean age of the individuals with TSCI was 16.4┬▒3.8 years. Of the 216 individuals with TSCI, 192 (88.9%) were Ōēź15 years old (male, 78.6%; n=151) (Tables 1, 2). And of 216 patients with TSCI, 10 patients (4.6%) were accompanied by hemorrhagic stroke.
Among TSCIs, motor vehicle-related complete SCI was observed in 60.2% of individuals, and motor vehicle-related incomplete SCI was observed in 39.8%. In the case of TSCI, the proportion of patients with complete injury was high. The most common level and severity of injury were complete paraplegia (n=78; 36.1%), followed by complete tetraplegia (n=52; 24.1%) (Table 2).
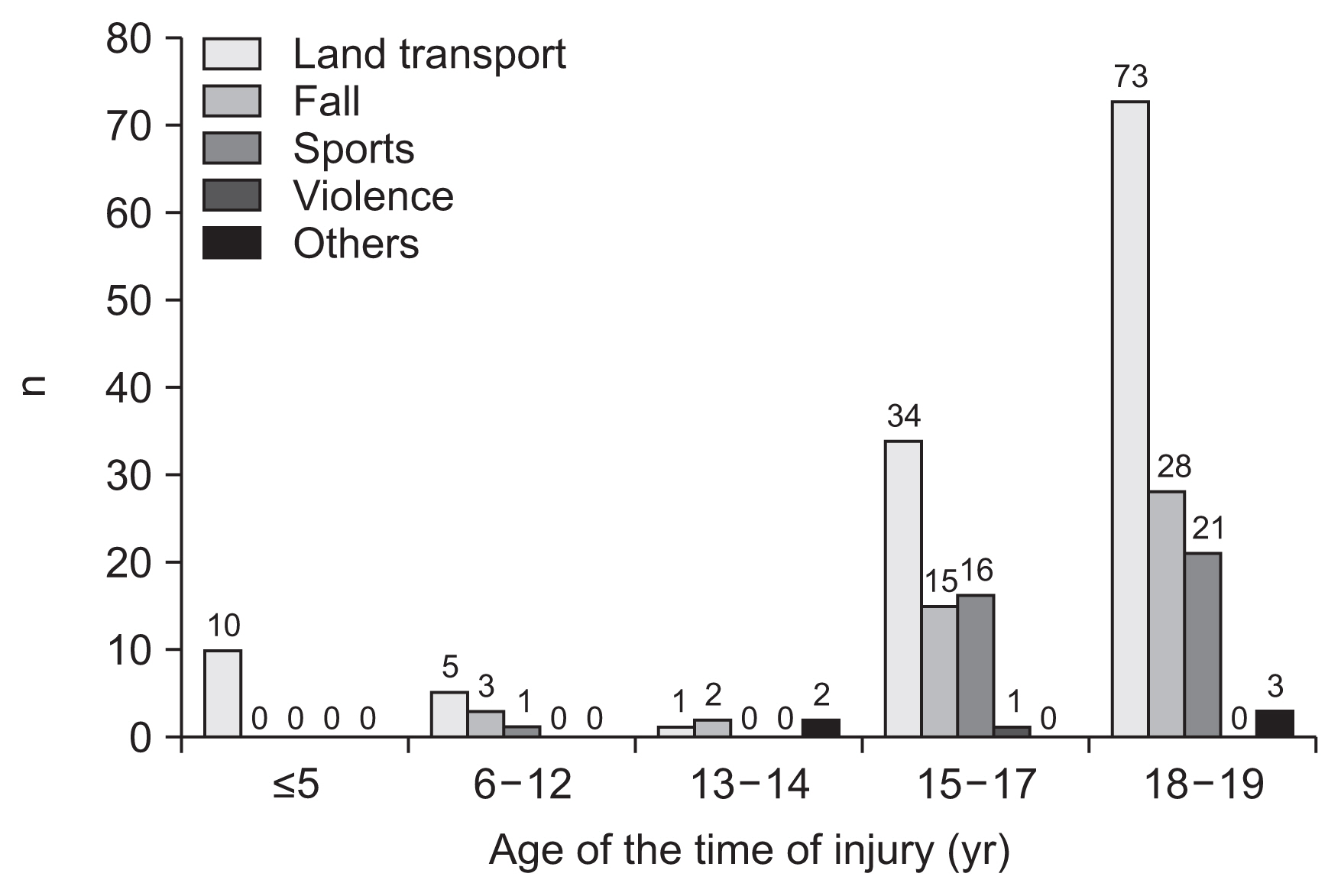
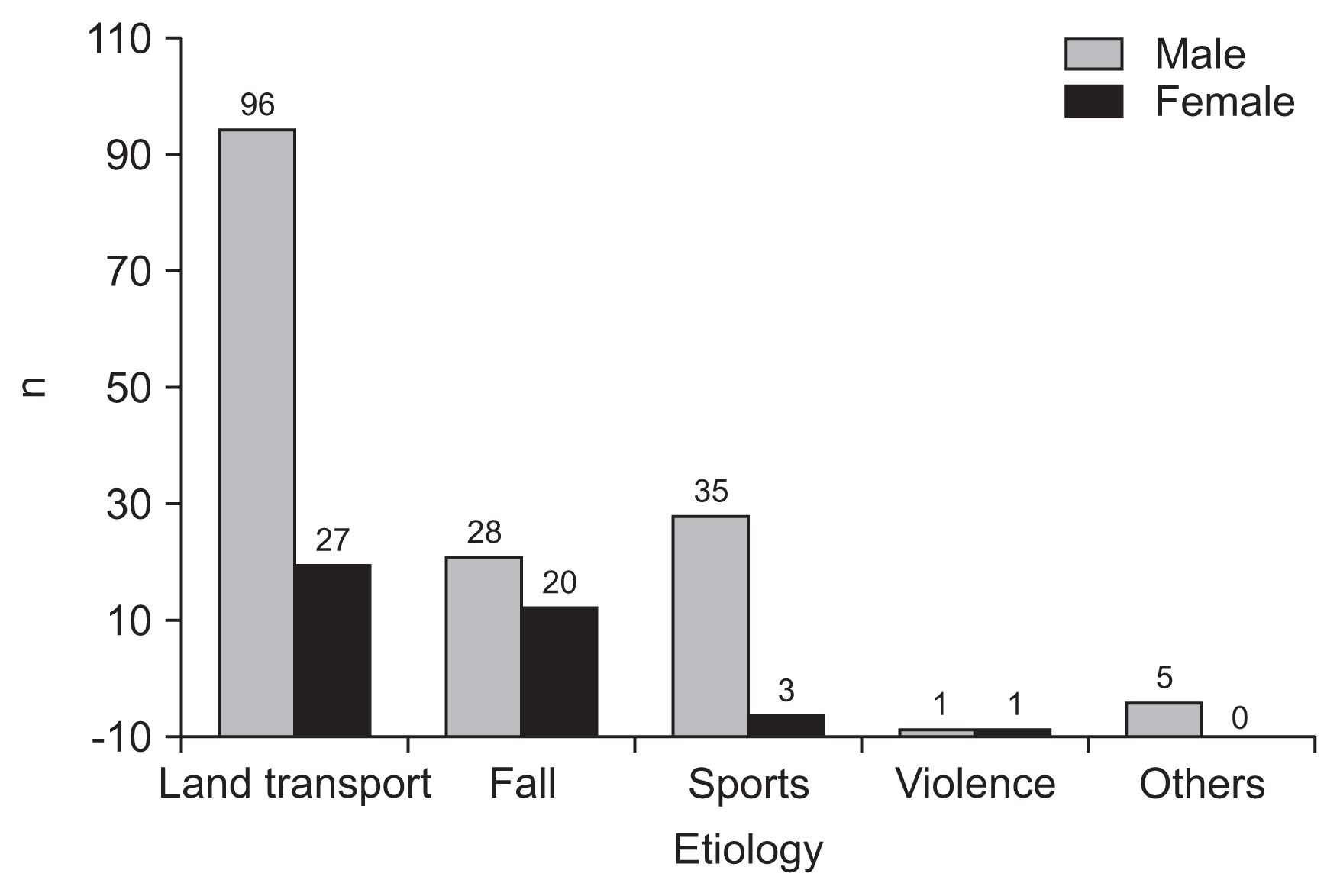
The most common cause of TSCIs was land transport accidents (n=123; 56.9%), followed by falls (n=48; 22.2%) and sports-related injuries (n=38; 17.6%) (Figs. 1, 2 and Table 2). Land transport accidents were the most common cause in both male and female participants. The second most common cause in male participants was sports, whereas in female participants it was falls (Fig. 2). There was no statistical significance between etiology and severity of injury. (p>0.05)
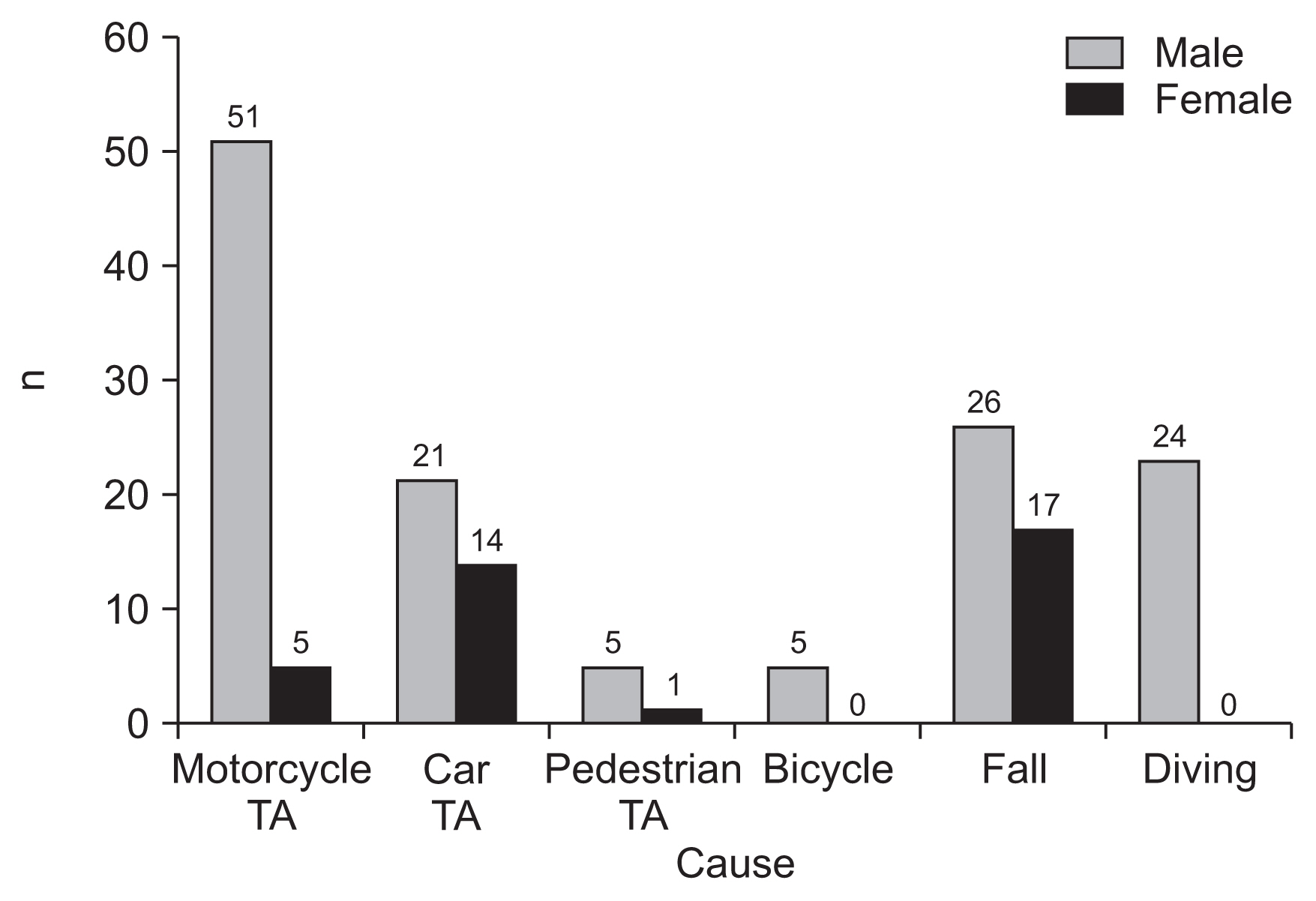
The causes of TSCI in the aged Ōēź15 years, were analyzed in detail (Fig. 3). The male-to-female ratio was 3.6:1. Land transport accidents (n=106; 55.2%) were the most common cause of TSCIs, followed by falls (n=43; 22.4%) and sports-related injuries (n=37; 19.3%). Of the land transport accident cases, 56 were due to motorcycle accidents, 35 were due to in-car traffic accidents, and six were due to pedestrian traffic accidents. Diving (n=24) was the most common cause of sports-related injuries (Fig. 3). According to sex, the most common cause of TSCIs in male participants was motorcycle accidents (n=51), followed by falls (n=26) and diving (n=24). In female participants, the most common cause of TSCIs was falls (n=17), followed by car traffic accidents (n=14) and motorcycle accidents (n=5) (Fig. 3).
According to the time of injury, TSCI occurred the most in June (n=26), July (n=27), and August (n=28) and the number of patients was below the average (n=18) in all the other months. There was no statistical significance between the month of the accident and the causes of TSCI (Žć2=54.269; p>0.05). During the study period, the month with the most pediatric TSCIs was August (n=28), and the least was April (n=9).
Non-traumatic spinal cord injuries
The mean age of participants with NTSCI was 12.5┬▒5.4 years. Of the 51 with NTSCIs, 12 (23.5%) had tetraplegia, 39 (76.5%) with paraplegia, 15 (29.4%) with complete injury, and 36 (70.6%) had incomplete injury. The most common injury level and severity were incomplete paraplegia (n=25; 49.0%), followed by complete paraplegia (n=14; 27.4%), incomplete tetraplegia (n=11; 21.6%), and complete tetraplegia (n=1; 2.0%) (Table 3).
Regarding etiology, inflammatory causes (n=17; 33.3%) were the most common, followed by neoplasm (n=13; 25.5%), vascular (n=8; 15.7%), infection (n=5; 9.8%), and other causes (n=5; 9.8%). There was no difference in etiology according to age.
Epidemiologic differences according to year of onset
In total, 97 individuals were hospitalized from 1990ŌĆō1999, 112 from 2000ŌĆō2009, and 58 from 2010ŌĆō2019. The proportion of individuals with TSCI according to the year of onset was 87.6% (n=85) in 1990ŌĆō1999, 77.7% (n=87) in 2000ŌĆō2009, and 75.9% (n=44) in 2010ŌĆō2019, with no difference between those with TSCI and NTSCI in terms of the year of onset. In addition, the severity of injury and site of injury did not differ in terms of the year of onset.
DISCUSSION
This study was conducted to describe the characteristics of PedSCI in Korea. Although PedSCI is a catastrophic event, it is difficult to study because it is relatively rare [5], and there are few prior research data on PedSCI in Korea. According to the results of our study the incidence of TSCIs in the PedSCI population in South Korea is high, particularly in males aged Ōēź15 years. The most frequent causes of TSCIs, in aged Ōēź15 years, were motorcycle accidents, followed by falls, car accidents, and diving. The causes of inflammatory and neoplasm accounted for more than half of patients of NTSCI. In addition, there were more patients with paraplegia and incomplete injury than those with tetraplegia and complete injury, respectively.
Vogel et al. [13] reported that 3%ŌĆō5% of TSCIs occur in individuals aged <15 years and 15%ŌĆō20% in <20 years old; however, these rates vary depending on the country and institution investigated [14,15]. In this study, 6.3% of TSCI patients admitted to the NRC during the 1990ŌĆō2019 period was aged <20 years.
Pediatric patients with TSCI had a mean age of 16.4┬▒3.8 years, and 88.9% with trauma were aged 15ŌĆō19 years. This is similar to that in the 2021 United States NSCISC annual report, where individuals with TSCI aged 15ŌĆō19 years accounted for 90.4% of all those <20 years old [16]. Compared with those aged <15 years, the number of cases due to land transport accidents, falls, and sports-related injuries increased rapidly in participants aged Ōēź15 years. In those Ōēź15 years old, land transport accidents were the most common cause of PedSCI, with motorcycle injuries accounting for the majority. Thus, reducing motorcycle accidents in Ōēź15-year-old boys would appear to be an essential injury prevention strategy.
Falls mainly involved accidents and suicide attempts [17]. Particularly in Ōēź15-year-old females, falls were the most common cause of SCIs, including suicide attempts. In a systematic review, Kennedy and Garmon-Jones [18] reported that approximately 6.8% of SCIs are due to suicide. According to the 2020 Korean Youth Risk Behavior Survey of the Korean Ministry of Health and Welfare, approximately 2% of middle- and high-school students in South Korea attempted suicide within the previous 12 months, with females having made more attempts than males [19]. However, this retrospective study relied on medical records; thus, whether the cause of the fall was an accident or a suicide attempt was not clearly noted, making it difficult to determine the exact number of falls attributable to suicide attempts.
All diving accidents involved males and mainly occurred in small outdoor pools and ravines in tourist locations. Diving accidents can lead to quadriplegia due to cervical SCI, and in this study, 24 individuals with diving-related TSCI admitted to the hospital were tetraplegic, of which 75% were motor-complete SCIs. The 58.3% in diving injuries occurred in July (n=6) and August (n=8). In the United States, violence-related SCIs have been reported to comprise the third most common SCIs among those aged <15 years, and the second-highest among those aged 15ŌĆō30 years [16]. However, in countries with restrictions on firearm use, such as Ireland, SCI cases due to violence are rare [20]. In this study, SCI due to violence was noted in 2 cases (0.9%). Thus, to prevent the occurrence of TSCIs in South Korea, it is necessary to discourage dangerous behaviors in middle- and high-school students aged Ōēź15 years, particularly among male students. The prevention of motorcycle and diving accidents should also be emphasized.
Regarding NTSCIs, inflammation (n=7) was the most common cause in those aged 0ŌĆō9 years, with six cases of these being due to transverse myelitis. In those aged 10ŌĆō19 years, neoplasm (n=13) was the most common cause. In pediatric NTSCI studies conducted in the United Kingdom Ireland, and Australia, transverse myelitis and neoplasm were the major causes of pediatric NTSCIs [20ŌĆō22]. Meningomyelocele was a common congenital cause. As the importance of folic acid supplementation in pregnant women has become widely known since the 1990s, the incidence of spina bifida has decreased [23], as reflected in our results. There were three individuals with NTSCI in the 1990s due to meningomyelocele and only one was similarly affected since 2000. Despite being a developed country, tuberculosis is still common in South Korea. In this study, there were three NTSCI cases in the 2000s caused by tuberculosis spondylitis.
The male-to-female ratio was 3.2:1 in pediatric individuals with TSCI and 0.7:1 in pediatric individuals with NTSCI. Traumatic causes suggest that males tend to be more active and engage in riskier activities than females, resulting in a lower incidence of TSCIs [5]. This study also showed that motorcycle and diving accidents with a high risk of trauma mostly occurred in males (93.7%) aged 15ŌĆō19 years.
This study had some limitations. First, it was a single-centered study; thus, our results cannot represent all individuals with PedSCI in South Korea. Second, data from individuals who required intensive care, such as those needed ventilator support and those who expired in the acute phase immediately after SCI, were not included because there is no intensive care unit ward in the NRC. Therefore, multicenter, large population-based studies should be conducted to acquire a more accurate picture of PedSCI epidemiology. Finally, it was impossible to determine whether TSCIs were caused by a fall accident owing to carelessness or a suicide attempt. Hence, the proportion of falls caused by suicide attempts remains unknown.
Nevertheless, this is the largest and most comprehensive study on PedSCIs in South Korea, involving data from the past 30 years. This study also analyzed the most frequent causes of TSCIs in detail. Therefore, this study is important because this can be used as reference in understanding the characteristics of PedSCI in South Korea.
In conclusion, this study describes the characteristics of PedSCI in South Korea. The proportion of men in TSCI was high, and the number of TSCI patients increased rapidly, after the age of 15 years. NTSCI mostly caused paraplegia and incomplete injury, and inflammatory and neoplasm induced SCIs were the most common.
In this study, we identified the current status and causes of PedSCIs in South Korea. Our results can be used as reference for appropriate evaluation, therapeutic approach and prevention strategy by age and causes.