INTRODUCTION
Visual function is considered to be one of the most important perceptions for development. During motor development, vision provides crucial feedback to the vestibular and proprioceptive systems [1]. Vision leads to the development of integrative functions such as eye-hand coordination, visual-manual-oral coordination, object recognition and learning, and visual-spatial recognition and learning. Several studies [2,3,4] on children who were diagnosed as blind or with visual impairment by an ophthalmologist have suggested that children with visual impairment show developmental delay and demonstrated the correlation between visual impairment and development. Also, the reported studies diagnosed the children's vision disorders based on ophthalmic examination, without the use of other vision-testing tools.
There exist few tools to evaluate the visual status of young children. Visual evoked potentials (VEPs) can provide diagnostic information on the functional integrity of the visual system. VEPs are visually evoked electrophysiological signals extracted from the electroencephalographic activity in the visual cortex recorded from the overlying scalp [5]. VEP testing is a simple, non-invasive, and easily accessible tool for evaluating the visual status of young children who might be uncooperative. Among several types of VEPs, flash VEP, which is less dependent on fixation, is commonly used in young children.
One study that used VEP in preterm infants within 2 weeks of birth identified a good predictive value for the occurrence of cerebral palsy [6]. However, the diagnosis of cerebral palsy was made at the corrected ages of 12 months in the study, which is too early for definitive diagnosis of cerebral palsy. Furthermore, no other developmental disabilities were assessed except for cerebral palsy. Thus, further studies involving both preterm and full-term babies and a longer follow-up period are required to clarify the diagnosis. In addition, studies using reliable assessment tools to evaluate development status such as the Bayley Scales of Infant and Toddler Development second edition (BSID-II) would reveal detailed information.
Until now, only a few studies have correlated VEP results in children with developmental delay. To our knowledge, there was no previous study which used VEP together with the BSID-II. The BSID-II is a tool used worldwide to evaluate the development of variable cognitive functions as well as the motor performances of infants and children [7]. Furthermore, the clinical significance of the VEP in children with developmental disorders has not been demonstrated. Therefore, the aim of this study was to investigate the neurodevelopmental outcome of children assessed with the BSID-II according to the VEP results.
MATERIALS AND METHODS
Subjects
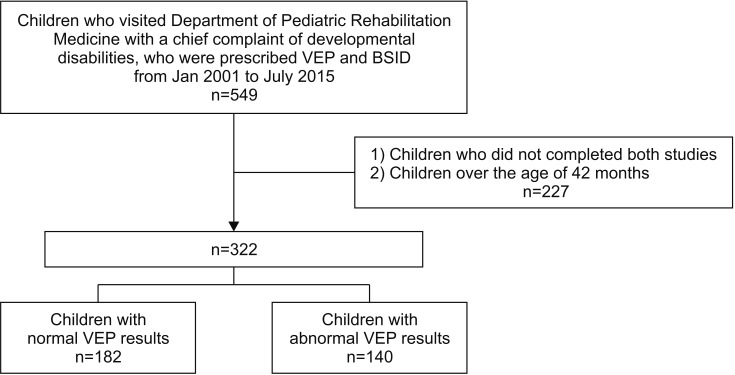
We retrospectively analyzed children who visited the Department of Pediatric Rehabilitation Medicine at Asan Medical Center, from January 2001 to July 2015 with a chief complaint of developmental disability. The medical records of 549 children who were prescribed both BSID-II and VEP studies were reviewed. And, 227 children who did not complete the studies or who were over than 42 months of age (not indicated for BSID) were excluded. Consequently, 322 children who completed both the BSID-II and VEP studies were enrolled.
Baseline characteristics
We reviewed the results of the VEP test and classified children into ŌĆśchildren with normal VEPŌĆÖ and ŌĆśchildren with abnormal VEPŌĆÖ groups. Consequently, the development of 182 children with normal VEP latency results and 140 children with delayed VEP latency results was compared (Fig. 1). Age, gender, whether preterm birth or not, and the children's underlying diseases were checked as baseline characteristics. Corrected age was used until the age of 24 months for children who were born in preterm. We divided the age into three groups to observe the correlation between the age and VEP result: (1) age younger than 12 months, (2) age of 12ŌĆō23 months, and (3) age of 24ŌĆō42 months. Underlying diseases included cerebral palsy, genetic disorders, developmental delay with unknown etiology, and others. Genetic disorders included syndromic diseases such as Down syndrome, Prader-Willi syndrome, and other gene mutations. Others included acute disseminated encephalomyelitis, meningoencephalitis, corpus callosum agenesis, seizure, metabolic disorder, and hearing impairment.
BSID
Results of BSID-II were analyzed for children's development. The BSID-II is composed of two scales: the mental developmental index (MDI) and the psychomotor developmental index (PDI). The MDI was designed to assess cognition by evaluating sensory perception, knowledge, memory, problem solving, and early language [8], whereas the PDI was designed to assess gross and fine motor skills. A higher index score indicates a better development: score of <70 represents significantly delayed performance, score of 70ŌĆō84 represents mildly delayed performance, score of 85ŌĆō114 indicates development within normal limits, and the score of >115 represents accelerated performance.
We primarily compared the MDI and PDI of the normal and delayed VEP latency groups. Children failing to achieve the minimum MDI or PDI score of 50 were assigned a score of 49 [9]. Many children had an MDI or PDI score under 50. For more detailed analysis, we additionally calculated the developmental quotient (DQ) using the mental and psychomotor age assessed with BSID and the chronological age [10]:
VEP
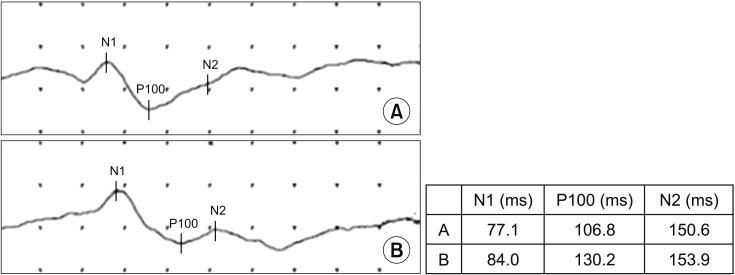
Flash VEP testing of both the eyes was used to evaluate visual impairments. The VEP was assessed in the electrophysiological laboratory at Asan Medical Center with Nicolet (Natus Medical Inc., Pleasanton, CA, USA). The study was performed by the rehabilitation medicine physicians and skilled examiners. The latency of the first positive waveform (P100) was mainly checked and was defined as delayed if it was over 115 ms [11] (Fig. 2). Among 322 children, 140 children showed delayed VEP latency results with delayed P100 latency and there was no child with absent VEP result. About 74% of children underwent VEP studies prior to the age of 24 months and the others underwent the studies between the age of 24 months and 42 months. The mean time difference between the VEP study and the BSID test was about 4 months, and the VEP study was usually done prior to the BSID test.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) software version 18.0 (SPSS Inc., Chicago, IL, USA). Based on the Kolmogorov-Smirnov and Shapiro-Wilk test, it was observed that the two groups did not follow the normal distribution. A Mann-Whitney U-test was used to analyze differences in MDI, PDI, and DQ between the two groups. Statistical significance was defined as p<0.05.
RESULTS
Baseline characteristics
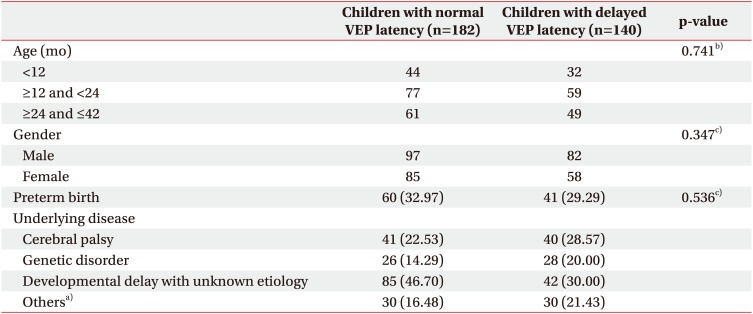
In total, 182 children with normal VEP latency results (56.5%) and 140 children with delayed VEP latency results (43.5%) were compared. There were no significant differences in the baseline characteristics between the two groups (Table 1). Mean ages were 19.26┬▒10.22 months in the normal VEP latency group and 19.98┬▒9.75 months in the delayed VEP latency group. There were 60 preterm birth children in the normal VEP latency group and 41 in the delayed VEP latency group. We subdivided children into three groups according to their age at BSID-II; similar distributions were seen in the groups. There were more male children than female in all the groups.
The etiology of the development delay and diagnoses was diverse, and many children were classified as having a developmental delay with unknown etiology. Within this category, 38 of 85 children in the normal VEP latency group and 25 of 42 children in the delayed VEP latency group were premature. There were 41 children with cerebral palsy in the normal VEP latency group and 40 in the delayed VEP latency group. There were 26 children with a genetic disorder in the normal VEP latency group and 28 in the delayed VEP latency group.
Comparison of development between the normal and delayed VEP latency groups
The children in the delayed VEP latency group showed a significant delay in both MDI and PDI scores and DQs of BSID-II compared with the children in the normal VEP latency group (Table 2). As per the Mann-Whitney U-test, the p-values of all the parameters were less than 0.05.
DQs were also compared between the two groups according to age (Table 3). The DQs of the mental and psychomotor domains were significantly lower in children with delayed VEP latency than in children with normal VEP latency, who were younger than 12 months and between 12 and 23 months of age. In children from 24 to 42 months, the delayed VEP latency group tended to show more delay than the normal latency group, but the difference was not statistically significant.
Subanalysis of the BSID-II index scores between the two groups based on their birth as full-term or preterm was done (Table 4). In a full-term group, children with delayed VEP latency showed a significant delay in both MDI and PDI scores compared with the children with normal VEP latency. In preterm group, though both the index scores of the children with delayed VEP latency showed more delay than those with normal VEP latency, only PDI was observed to be significantly different.
DISCUSSION
Our current study findings indicate that children with delayed VEP latency results exhibited impediment in both mental and psychomotor development compared with children with normal VEP latency. These findings are consistent with the common concept that vision plays an important role in development and learning and that visual impairment would lead to disturbance in development.
Both mental and psychomotor developments are visually driven. Rolling over, raising up on upper limbs, sitting, crawling, and walking are all believed to be driven initially by visual stimulation triggered by some factor in the environment, coupled with the drive to obtain objects, explore, and manipulate them and thus learn about them. Therefore, a great extent of developmental delay observed in both mental and psychomotor development in the delayed VEP latency group compared to the normal group seems to be reasonable.
Significant differences were observed in the index scores of BSID between the normal and delayed VEP latency groups including all ages. However, a comparison of the index scores of the subdivided age groups revealed only a significant difference in children aged between 12 and 23 months and not in children younger than12 months and from 24 months to 42 months, possibly because many children had index scores under 50 (assigned a score of 49) in both the groups. Comparisons of the DQs of BSID in the subdivided age groups revealed no significant differences in children younger than 12 months and those aged between 12 and 24 months.
Subgroup analysis based on the birth of children as full-term or preterm revealed no significant difference in MDI between the children born at preterm in both the groups. However, both MDI and PDI showed a significant delay in the delayed VEP latency group in children born at full-term. These results suggest the reliability of VEP in children born at full-term. The previous study on VEP between premature and full-term children demonstrated the vulnerability of VEP abnormality in premature infants than full-term infants [12].
The results of our present study are consistent with those of the previous reports that stated a correlation between visual impairment and developmental delay. Levtzion-Korach et al. [2] compared the motor development in blind children with a sighted control group based on Bayley and Denver's motor milestones, and reported a highly significant developmental delay in all the motor skills in the blind children. However, the study only examined the motor development, and children with a mild visual impairment who could see the objects were excluded. A study by Vaizey et al. [3] reported a correlation between the severity of visual impairment and the incidence of neurodevelopmental delay in a series of 30 patients with congenital retinal dystrophies. However, the case series did not present any developmental assembly and some patients were found to be mentally subnormal. In addition, the participants were limited to Leber congenital amaurosis patients, diagnosed with electroretinography.
Cass et al. [4] revealed that developmental setback is a significant clinical problem among children with severe visual impairment and is most prevalent in those with the greatest degree of visual impairment. This finding is different from our present analyses as it focused on the developmental setback in children who are initially thought to be undergoing normal development by 16 months of age. Additionally, the participants in the study of Cass et al. [4] were all diagnosed with visual impairment by an ophthalmologist and the study only focused on cognitive progress and used Reynell-Zinkin scales of mental development, which were designed for young visually handicapped children.
Several studies have investigated the prognostic value of VEP in high-risk newborns. Kato and Watanabe [13] reviewed the relevant reports and concluded that VEP demonstrates a good correlation with neurodevelopmental outcome in full-term infants with birth asphyxia. However, based on the five articles they reviewed, the prognostic value of VEP in preterm infants was controversial [6,14,15,16]. The five reviewed studies mainly focused on the prevalence of cerebral palsy as a neurodevelopmental outcome. The VEP examinations were performed in the preterm infants within 3 weeks of birth. And the follow-up time of assessing neurodevelopmental status ranged from 12 to 24 months, which is too early to diagnose cerebral palsy. Except for a study that included 123 preterm infants, the others included less than 100 participants.
Our current study reviewed a fairly large number of children and included both full-term and preterm infants. Furthermore, this is the first study to use the BSID-II, a widely accepted reliable developmental assessment tool for evaluating development status, along with VEP. We not only examined the prevalence of the neurodevelopmental disorder but investigated both mental and psychomotor development.
There are several limitations in our study. First, in this retrospective analysis, we could only obtain limited information recorded in the medical chart. Secondly, although most of the children we analyzed underwent the VEP study at around 1 year of age, the time of the VEP study varied from several months to 3 years. In addition, though the P100 latency of VEP changes rapidly in form and complexity in the first 6 months and reaches the typical adult value by 1 year of age [11,17], the latency in preterm infants can be a little more delayed by 5 months [18]. Although the VEP study is typically done after 6 months of age in our hospital, we should be cautious with the interpretation of this value.
Though in the present study, as per the result of VEP normal and delayed latency groups were designed, the value of the latency was not checked. Therefore we could not concretely suggest the degree of the latency delay and further analyze the correlation with delayed development. These aspects need to be considered in the future study. Furthermore, the mean time difference between the VEP study and the BSID test was about 4 months, which is not a short-term for young children. Also, we could not control the extent of rehabilitation undertaken by the participants. It is hypothesized that differences in rehabilitation program intensity would probably affect children's development. Lastly, ophthalmologic interventions, such as prescription of corrective lenses or surgery, were not considered.
In conclusion, children with VEP-proven visual impairment showed a more developmental delay in both mental and psychomotor domains. Although VEP provides limited information, it does have any clinical usefulness. When a physician has concerns about visual impairment, VEP studies could be easily applied to children with suspected developmental delay. In addition, VEP study results could provide an insight into children's development and serve as early indicators for consultation with an ophthalmologist for the existing problem.