INTRODUCTION
Lumbar muscles functionally support and maintain the stability of the spine. The weakness of back muscles is the main cause of recurring low back pain [1].
The psoas muscle is the largest muscle at the cross section of the lower levels of lumbar spine [2]. It stabilize the spine through its potential to generate large compressive forces, thereby increasing the spinal stiffness [3]. Unilateral disc herniation affects the psoas muscle at two locations (the lumbar spine and the hip joint) leading to more pronounced atrophy of the muscle compared with atrophy in other muscles [4]. The multifidus muscle is the most medial part of the lumbar paraspinal muscles [5], unisegmentally innervated by the dorsal ramus medial branch of the segmental nerve [2]. Multifidus muscle atrophy has specifically been studied in relation to disc lesion. Hyun et al. reported a significant decrease in the cross-sectional area (CSA) of the ipsilateral multifidus muscle in patients with unilateral lumbosacral radiculopathy [6]. The erector spinae muscle acts as a global muscle that affects the movement and muscular strength [1]. Since it has a longer lever arm than the multifidus muscle, most of the extensor momentum of the trunk is generated from this muscle rather than the multifidus muscle [7]. Few studies have evaluated the size of the erector spinae muscle in patients with lumbar radicular pain.
Previous studies have shown a significant correlation between the size of a muscle, measured as its CSA, and its ability to generate maximum voluntary isometric force. Since muscular strength is proportional to the CSA of the muscle, the measurement of the CSA of muscle is indirectly used to estimate the strength of the lumbar muscle [1].
To date, there have been several studies of lumbar muscle changes in patients with low back pain or radiculopathy. However, few reports have evaluated the association between the chronicity of unilateral lumbar radiculopathy and the CSA of lumbar muscles, and the studies reporting the association are contradictory. Kim et al. [2] reported that the CSA of multifidus muscle was reduced by disc herniation when symptom duration was three months or more. Conversely, Farshad et al. [8] reported that the asymmetry of multifidus muscle correlated with neither severity nor duration of nerve root compression in lumbar spine. In addition, very few studies have evaluated the changes of both multifidus and erector spinae muscles in patients with unilateral lumbar radiculopathy.
The current study therefore assessed the CSA of paraspinal and psoas muscles using magnetic resonance imaging (MRI), and investigated whether there was an asymmetrical occurrence of the paraspinal (multifidus and erector spinae) and psoas muscles, and whether this feature was related to the chronicity of unilateral lumbar radiculopathy.
MATERIALS AND METHODS
Subjects
This was a retrospective study of patients who visited the outpatient clinic of the Department of Rehabilitation Medicine of Kyung Hee University Hospital from January 2012 to December 2014 for symptoms of unilateral lumbar radiculopathy.
Inclusion criteria included: (1) clinical symptoms of unilateral radiculopathy, (2) unilateral L5 radiculopathy seen on electrodiagnostic study of the both lower extremities, and (3) lumbar disc herniation at the L4-5 level on lumbar MRI. The electrodiagnostic criteria for unilateral lumbar radiculopathy included: (1) abnormal spontaneous activity in the unilateral involved paraspinal muscles and/or (2) abnormal spontaneous activity, or abnormal motor unit morphology consistent with nerve injury (polyphasic, large amplitude, increased duration), or reduced recruitment patterns in involved limb muscles innervated by the same myotome but by different nerves.
Exclusion criteria were bilateral symptoms of lower extremities, peripheral polyneuropathy, previous spinal surgery, spinal fracture, spinal cord injury, tumor or infection, and comorbidities influencing physical activities (e.g., severe heart disease, cerebrovascular accident).
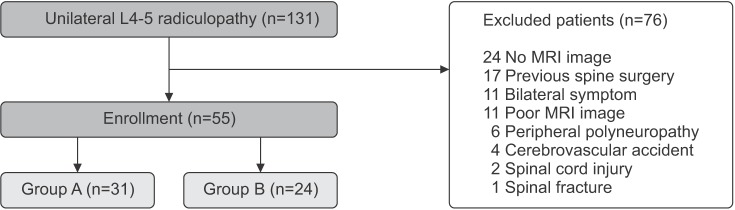
Of the total patients screened, 139 were eligible on the basis of their clinical symptoms and electrodiagnostic findings, of which 78 patients were excluded from the study. Finally, 61 subjects (31 males and 30 females) were enrolled in this study. The subjects were divided into two groups based on their symptom duration of unilateral radiculopathy: patients with a symptom duration less than 3 months (group A, 30 cases), and patients with a symptom duration of 3 months or more (group B, 31 cases) (Fig. 1).
Measures and procedures
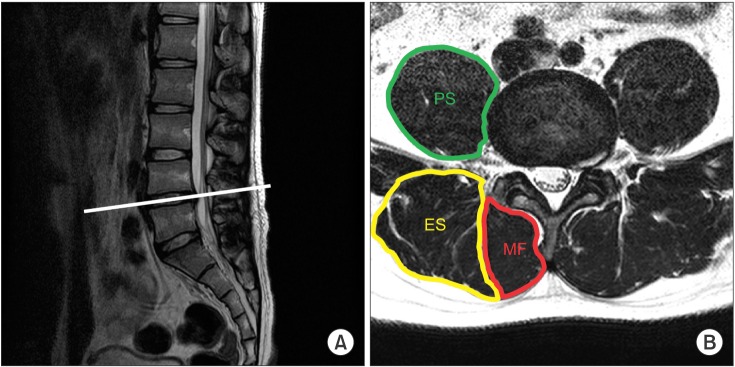
All patients underwent lumbosacral spine MRI within four weeks before or after the diagnosis of unilateral L5 radiculopathy by electrodiagnostic study. We captured axial T2-weighted images of MRI at the level of the L4–5 and L5–S1 intervertebral disc, which was obtained at the middle between the lower margin of the upper vertebra and upper margin of the lower vertebra. The CSA of both sides of muscles (multifidus, erector spinae, psoas) and lower margin of L4 vertebra were measured by drawing their outlines with the region of interest (ROI) using a PiView program (Infinitt, Seoul, Korea) (Fig. 2). Previous studies had used the relative CSA (rCSA) to compensate for the influence of individual body shape, body weight, and height on the CSA of the muscles [1]. We therefore calculated the rCSA of the muscles, which is defined as the ratio of the CSA of muscles to that of the lower margin of L4 vertebra.
All CSA measurements were performed independently twice by the same person to minimize the potential for error in constructing the polygons around the margins of muscles. The average value of the two measurements was used for statistical analysis. Clinical and electrodiagnostic findings of all cases were blinded.
Statistical analysis
Statistical analysis was performed using the SPSS ver. 13.0 for Windows (SPSS Inc., Chicago, IL, USA). Demographic differences between the two groups were analyzed using chi-square test and independent t-test. Paired t-test was compared the CSA and rCSA between the affected and normal sides in each group. Statistical significance was considered when the p-value was less than 0.05. All values are presented as mean±standard deviation.
RESULTS
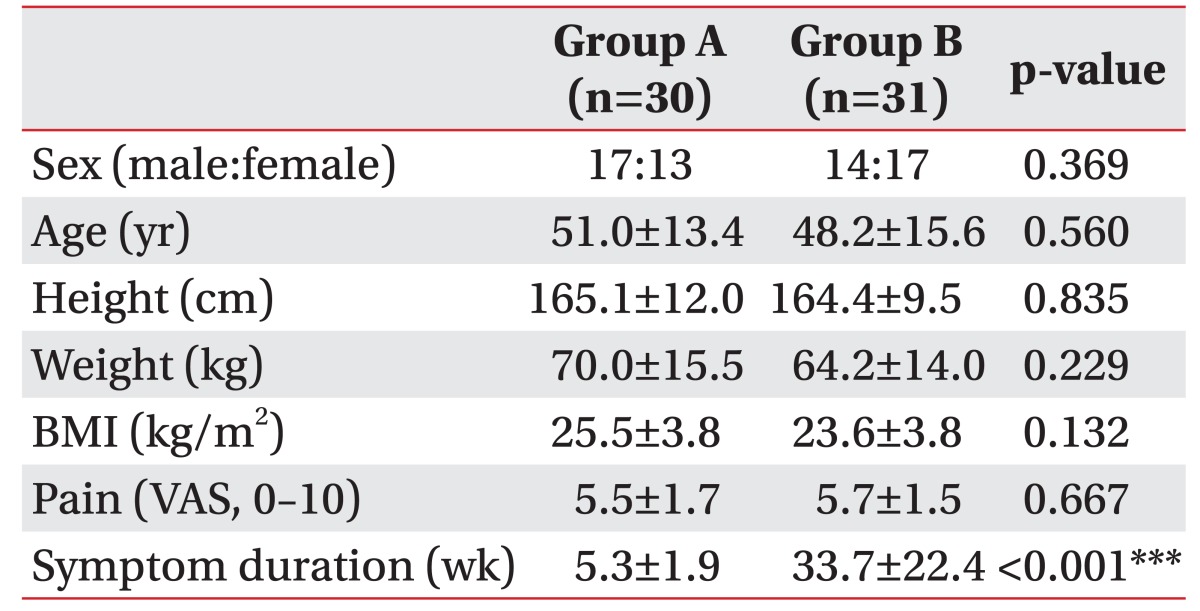
Group A comprised 17 men and 13 women, with mean age 51.0±13.4 years (range, 25–76 years). Group B comprised 14 men and 17 women, with a mean age 48.2±15.6 years (range, 19–71 years). There were no significant differences in demographic characteristics of both groups, except symptom duration (Table 1).
In group A patients with a symptom duration less than 3 months, the differences were statistical not significant in in any of the muscles, with regards to the rCSA of the involved and the uninvolved sides, at both the L4–5 and L5–S1 levels (Table 2).
In group B patients with a symptom duration of 3 months or more, the rCSA of erector spinae was significantly smaller only at the L4–5 level on the involved side (0.816±0.185) as compared with the uninvolved side (0.855±0.210) (p<0.05), but this difference was not observed at the L5–S1 level.
The rCSA of multifidus muscle at the L4–5 level was significantly smaller on the involved side (0.463±0.165) as compared with the uninvolved side (0.500±0.195); a similar significant difference was also observed at the L5–S1 level (0.522±0.106, 0.540±0.101) (p<0.05).
The rCSA of psoas muscle measured at the L4-5 level was rather small on the involved side (0.857±0.252) than the uninvolved side (0.868±0.215), but there were no statistically significant differences in the rCSA of the involved and uninvolved sides at all levels (Table 3).
DISCUSSION
To date, there have been several studies for multifidus muscle changes in patients with lumbar radiculopathy. However, few reports have evaluated the relationship between the chronicity of unilateral lumbar radiculopathy and the CSA of lumbar muscles, and the results have been contradictory. Farshad et al. [8] reported that the asymmetry of multifidus correlated with neither severity nor duration of nerve root compression in lumbar spine. However, Kim et al. [2] demonstrated that the CSA of the multifidus muscle was reduced by lumbar disc herniation with symptom duration 3 months or more.
In this study, the rCSA of multifidus muscle was influenced by the lumbar unilateral radiculopathy, which was seen only in patients with symptom duration of 3 months or more.
The multifidus muscle is divided into 5 myotomes, each innervated by a single spinal segment. Muscle fibers attaching to the spinous process of a particular vertebra are segmentally innervated by medial branch of the dorsal ramus that originates inferior to the respective vertebra [9]. There have been some studies regarding the extent of multifidus atrophy in patients with lumbosacral radiculopathy. Battie et al. [10] reported that asymmetry of multifidus is most apparent from the muscle measurement at the disc level below the affected disc, and to a lesser degree at the level of herniation because of the unisegmental innervation of multifidus. Similarly, Kang et al. [11] suggested that the most severe atrophy of the multifidus muscle may occur at the mid spinous process level of the vertebra, which is one level below the segmental number of involved nerve root in patients with single level unilateral lumbar radiculopathy.
In this study, multifidus atrophy was shown at the level of L4–5 and L5–S1 intervertebral disc level in unilateral L5 radiculopathy patients with symptom duration of 3 months or more. In our opinion, there are two mechanisms that cause the atrophy of the multifidus muscles: denervation and disuse.
Previous studies revealed that the atrophy of the multifidus muscle was seen at the intervertebral disc level which is one level below the segmental number of involved nerve root, because of the unisegmental innervation of multifidus [10,11]. The L5 medial branch of the dorsal ramus innervates the fascicles of multifidus arising from spinous process of L5 vertebra. Therefore, in this study, we suppose that the denervation of the dorsal ramus by L5 radiculopathy mostly affects the multifidus muscle at the L5–S1 intervertebral disc level.
Furthermore, our study observations revealed that atrophy of the multifidus and erector spinae muscles were at the level of the L4-5 intervertebral disc only, in patients with symptom duration of 3 months or more. At this level, the atrophy of back muscles could mainly be due to disuse. Parkkola et al. [12] suggested that disuse arising with back pain causes disuse atrophy. Other studies have established that multifidus atrophy in unilateral back pain is localized rather than generalized, and lumbar dorsal ramus syndrome causes multifidus atrophy in patients with back pain, thus triggering a vicious cycle that promotes atrophy [5]. The maximum CSA of the back muscles are usually observed at the L4–5 intervertebral disc space, and asymmetry of back muscles caused by disuse atrophy are frequently found at this level.
Previous studies reporting the effect of lumbar pathology on psoas size have been contradictory. Dangaria and Naesh [4] reported significant reduction in the CSA of psoas muscle in the affected side only, prominently at the level of disc herniation. Conversely, Danneels et al. [13] reported no change in psoas size in patients with low back pain. In our study, the CSA of the psoas muscle was not influenced by unilateral lumbar radiculopathy. In our opinion, since psoas muscle is not innervated directly by the dorsal ramus of the medial branch, the denervation atrophy may not occur in the psoas muscle. In addition, the psoas muscle acts as a hip flexor which is different from the other two muscles, namely the multifidus and erector spinae. We did not see any atrophy of the psoas muscle, indicating that the muscle atrophy of multifidus and erector spinae was not merely due to general disuse atrophy resulting from global inactivity. The cause of these differences will be examined in the future studies.
A strength of our study was in the diagnosis of lumbosacral radiculopathy. In most previous studies, the patient group with disc herniation and radiculopathy was divided based solely on the clinical symptoms and MRI findings, without electrodiagnostic findings. Only Kang et al. [11] used electrodiagnostic tools in addition to the clinical symptoms and MRI findings. Electrodiagnostic study is an essential method to confirm lumbosacral radiculopathy, and is considered to be a more objective method to reveal the association between muscle atrophy and denervation [6,14,15].
There were several limitations in this study. First, the study sample size was small. Second, because this study was performed retrospectively, standardized assessment of the severity of pain and daily activity were not available. Medical treatment leading to pain relief may also affect the structure of lumbar muscles. This will be examined in the future prospective studies. Finally, only gross measurement techniques were used, and this did not allow for any computation of muscle degeneration due to increased amount of fatty deposit within the muscle.
In conclusion, the study findings suggest that the atrophy of the multifidus and erector spinae muscles ipsilateral to the lumbar radiculopathy are observed only in patients who suffered from unilateral radiculopathy for 3 months or more.