INTRODUCTION
Stroke is the second leading cause of death worldwide and can lead to severe, long-term disability. Over 75% of stroke survivors are left with a disability that makes it difficult to find employment, and over 80% of patients experience motor dysfunction requiring rehabilitation therapy [1,2]. In addition to neurological deficits, various medical complications can occur following a stroke [3]. Moreover, complications from stroke interfere with early rehabilitation therapy and prevent recovery [4].
In patients with acute stroke, a considerable number of medical complications that occur during hospitalization can be prevented or treated if they are detected early [5]. The availability of data on the types and incidence of medical complications facilitates both treatment and prognosis. Several studies have assessed poststroke medical complications and discussed their effects on prognosis and socioeconomic status [6,7]. Since the pattern of complications differs in accordance with the medical environment and characteristics of different countries and regions, a nationwide cohort study of complications occurring during the first admission period of stroke is warranted.
The present investigation is part of the Korean Stroke Cohort for Functioning and Rehabilitation (KOSCO) study, which was designed and instituted to investigate the following: (1) the prevalence of and risk factors for post-stroke medical complications and (2) the association of such complications with functional outcomes in a cohort of Korean patients. This study specifically aimed to assess the KOSCO cohort to garner information that will aid in decreasing the prevalence of post-stroke complications and facilitate successful recovery.
MATERIALS AND METHODS
Study design and data sources
The present study is part of the KOSCO study [8]. KOSCO is a nationwide, multicenter, prospective study of consecutive Korean patients suffering first stroke episodes. KOSCO was designed with a 10-year follow-up period to investigate residual disabilities, activity limitations, and quality of life and their influencing factors.
Patients with first stroke episodes admitted to nine university hospitals in Korea from August 2012 to June 2015 were recruited. All study sites received Institutional Review Board ethical approval for human research and complied with the tenets of the Declaration of Helsinki (IRB No. 2012-06-016 of Samsung Medical Center). Patients provided written informed consent to participate in the study.
The medical complications from stroke onset until discharge evaluated in this study included the following: thromboembolic disease, pneumonia, ventricular insufficiency, urinary tract infection, bladder dysfunction, bowel dysfunction, pressure sores, shoulder dysfunction, complex regional pain syndrome (CRPS), seizure, joint contracture, central post-stroke pain syndrome, falls and injuries, fracture, and insomnia.
Clinical assessment
Patient age, sex, and the clinical characteristics of stroke were obtained through an examination of the patients' clinical records. Assessments were made according to the following metrics: comorbidities using the Charlson Comorbidity Index (CCI); clinical function (including stroke severity) via the Korean version of the National Institutes of Health Stroke Scale (K-NIHSS); cognitive function by the Korean version of the Mini-Mental State Examination (K-MMSE); swallowing function using ASHA-NOMS (American Speech-Language-Hearing Association National Outcome Measurement System swallowing scale); activities of daily living via the Functional Independence Measure (FIM); and lastly, motor function at 7 days, 3 months, 6 months, and 12 months post-stroke via the Fugl–Meyer Assessment (FMA).
The CCI is often used to measure health status and it has been used in many clinical studies as it provides an overall score for comorbidity based on a weighted score from 1 to 6 assigned to 19 selected conditions [9]. CCI assigns 1 point to all forms of coronary artery disease as well as to congestive heart failure, peripheral vascular and cerebrovascular diseases, dementia, chronic pulmonary disease, connective tissue disease, peptic ulcer, mild liver disease, and diabetes. The score for hemiplegia and organ damage in addition to diabetes, any tumor, leukemia, or lymphoma is 2. Moderate or severe liver disease is assigned a score of 3 and AIDS or metastatic solid tumor a score of 6 [10].
The NIHSS comprises 11 items including the level of consciousness, visual field, facial paralysis, limb ataxia, sensation, speech, and inattention. A higher score indicates a higher severity [11]. The MMSE is the most widely used test for detecting dementia [12]. In the present study, we used the K-MMSE, which has been standardized for elderly Korean individuals [13].
The FMA is an index for evaluating motor function and comprises five domains: joint movement and pain, sensation, balance, and upper and lower limb motor function [14]. These five domains are further divided into subcategories, each of which is graded on a three-point scale as follows: 0, complete inability to perform the task; 1, partial ability to perform the task; and 2, perfect ability to complete the task. The FIM comprises five domains: personal hygiene, sphincter control, mobility, communication, and social cognition. The results are represented by a score, the highest being 126 [15].
Statistical analysis
We analyzed the incidence of and risk factors for post-stroke medical complications. Functional outcomes were determined at discharge and then at 3, 6, and 12 months after stroke onset using online registry forms. In univariate analysis of patients with and without complications, continuous variables were reported as mean±standard deviation (SD) when the distribution was normal and medians with interquartile ranges when the distribution was not normal. Continuous variables with normal and non-normal distributions were compared using t-tests and Wilcoxon rank-sum tests, respectively. Categorical variables were analyzed using χ2 or Fisher exact tests when appropriate. For the analysis of risk factors for post-stroke complications, only those variables that showed a p-value of <0.05 in univariate analysis were included in multivariate logistic regression analysis. For the analysis of functional outcomes as defined by the number of complications, repeated-measures analysis of variance (RM ANOVA) was performed. The Bonferroni correction was used for post-hoc analysis. All tests were two-tailed and a p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Demographic data
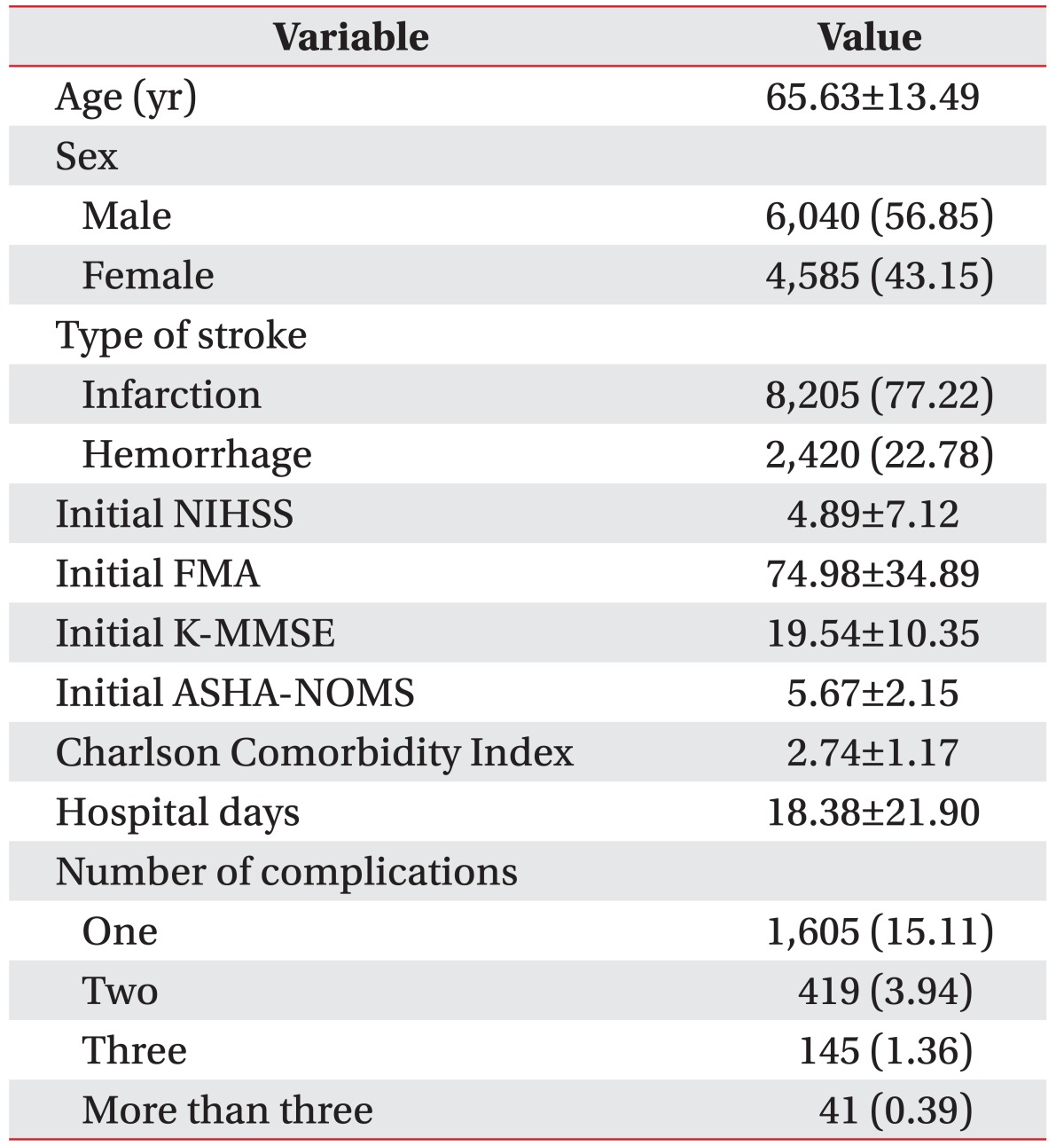
Between August 2012 and May 2015, a total of 8,205 patients with ischemic stroke and 2,420 with hemorrhagic stroke were enrolled in the KOSCO study. The average age of patients was 65.63 (±13.49) years, and 4,585 (43.2%) were female. Mean hospitalization was 18.4 (±21.9) days. The length of hospitalization was significantly longer in the complication group than in the without-complication group (p<0.01). A total of 2,210 patients (20.8%) exhibited at least one medical complication in the acute or the subacute stage (Table 1).
Incidences of post-stroke medical complications
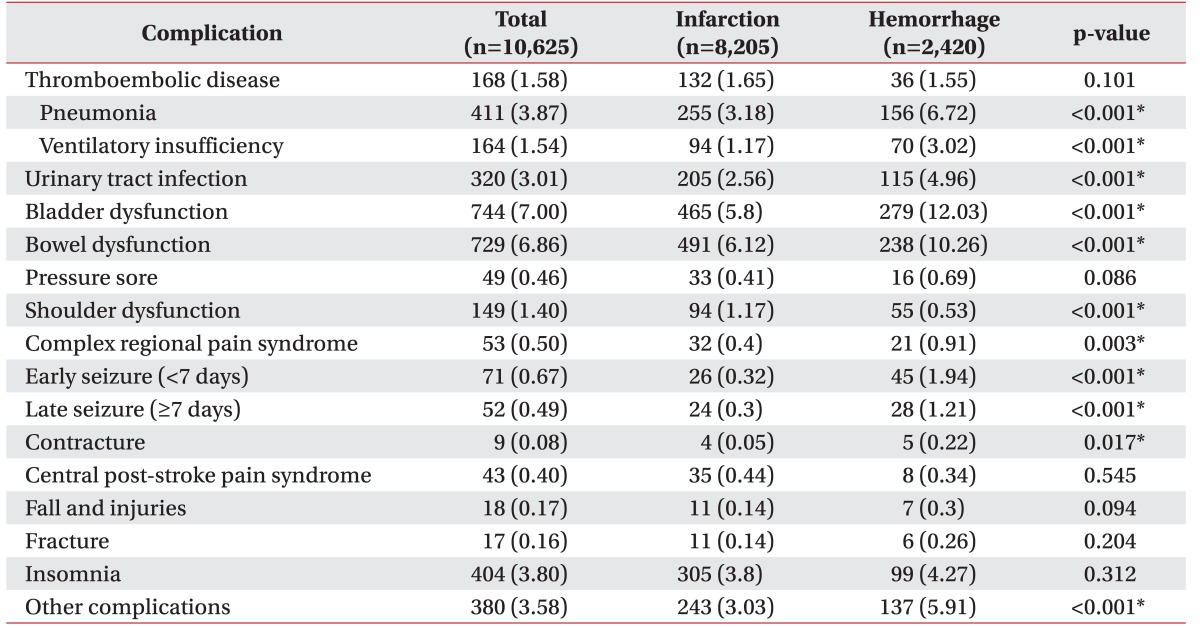
The frequencies of post-stroke medical complications are shown in Table 2. Bladder dysfunction was the most common complication (8.0%), followed by bowel dysfunction (6.9%) and sleep disturbances (3.8%). With regard to infectious diseases, pneumonia and urinary tract infection (UTI) occurred in 3.8% and 3.0% of patients, respectively. As for painful conditions, shoulder dysfunction, CRPS, and central post-stroke pain syndrome occurred in 1.4%, 0.5%, and 0.4% patients, respectively.
Compared to patients with ischemic stroke, those with hemorrhagic stroke showed a higher overall incidence of complications. In particular, the incidence of early and late seizures was approximately four times higher in the latter.
Risk factors for post-stroke medical complications
Multivariate regression analysis (Table 3) showed that medical complications after stroke occurred more often in elderly patients (95% confidence interval [CI], 1.002–1.012), patients with pre-existing comorbidities (95% CI, 1.218–1.336), hemorrhagic stroke (95% CI, 1.475–1.979), poor swallowing function as assessed using ASHA-NOMS (95% CI, 0.855–0.921), and low FMA scores at admission (95% CI, 0.989–0.991).
Effects of post-stroke medical complications on functional outcome
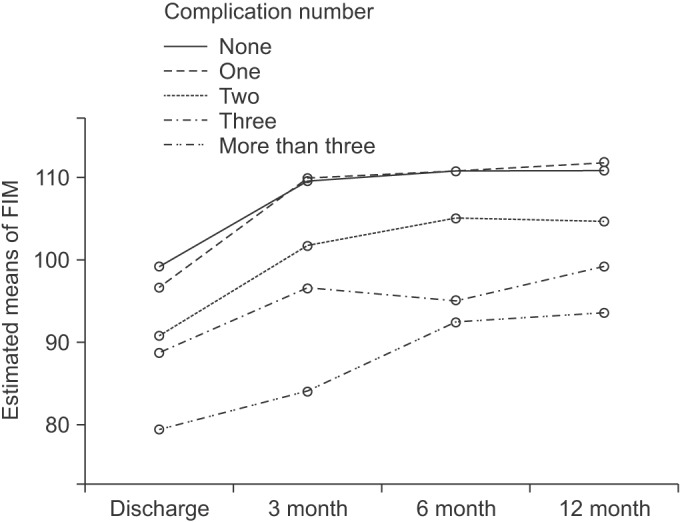
In order to investigate the effects of post-stroke medical complications on functional outcome, FIM scores were compared for 2,490 patients who underwent a 12-month functional assessment follow-up. The FIM scores changed significantly over the post-stroke study time course (F=9.22, p<0.05), and the degree in FIM score changes varied significantly according to the number of medical complications (F=2.39, p<0.05). Specifically, the patients with relatively more complications showed poorer functional outcomes from the time of discharge to 12 months after stroke onset, except at the 3 to 6 months interval, even after adjustment for age and FMA scores at 7 days after stroke onset (F=6.66, p<0.01) (Fig. 1).
DISCUSSION
In the present study, we investigated the prevalence of and risk factors for post-stroke medical complications in hospitalized Korean patients with first stroke episodes and determined the impact of complications on functional outcome after stroke. In our cohort, 20.8% experienced at least one post-stroke medical complication; this rate of incidence is lower than in previous studies, which reported complication rates of 56%–96% during inpatient stroke rehabilitation [4,16,17,18,19]. One multicenter study reported that internal medical complications occurred in 85% of patients with acute stroke, with pain being the most common complication (34%), followed by falls (25%), UTI (24%), pneumonia (22%), and bedsores (21%) [5].
In addition, in a previous study investigating 984 Korean patients [20], the incidences of pneumonia and pressure sores were 5.8% and 2.7%, respectively, which is considerably higher in both cases than in the present study. The lower rates observed in our cohort can be attributed to thorough post-stroke care including early mobilization, lung care, and early work-up for dysphagia.
Our findings appear to confirm previous studies [21] that showed more complications and more severe strokes occur in the elderly. Previous studies reported a higher incidence of post-stroke medical complications in patients with a higher stroke severity [21,22,23]. We have also confirmed that the extent of the initial motor impairment influenced the incidence of post-stroke medical complications. Hemorrhagic stroke was a significant risk factor for post-stroke complications. Greater stroke severity in the initial stage of hemorrhagic stroke might affect the likelihood and severity of post-stroke medical complications.
In our study, the incidence of medical complications increased with increasing comorbidity scores. Patients with a higher number of medical complications showed poor functional outcomes not only at the time of discharge, but also 12 months after stroke onset. Moreover, the duration of hospitalization was longer in the patients with additional medical complications than in those without. Previous work has generally been in accordance with these findings, though with some distinctions. Kiely et al. [24] reported that functional outcomes at the time of discharge were poor in patients with stroke accompanied by a systemic disease, although there was no significant correlation with the number of diseases. However, in another study, the functional outcomes at the time of discharge were found to deteriorate with an increase in the number of systemic diseases accompanying stroke [25]. Roth et al. [26] reported that 19% of rehabilitating stroke patients experiencing complications were transferred to an acute care unit, resulting in prolonged hospitalization. Kim et al. [7] reported that patients with pneumonia, UTI, myocardial infarction, depression, dementia, or delirium as post-stroke complications showed poor functional measure scores at discharge. Moreover, the number of complications has been associated with increased duration of hospitalization [4,6]
Altogether, it would be expected that accompanying systemic disease, and possibly a greater number of comorbidities, would directly correlate to the prevalence of post-stroke medical complications and poor functional outcomes, as our results indicate. In order to prevent general deconditioning, our findings and previous studies suggest that rapid countermeasures would be taken to decrease the incidence of medical complications after stroke. The present study has the following limitations. First, post-stroke medical complications other than those assessed in this study can occur. In particular, among patients with other complications, a considerable number showed symptoms of depression. There is much variation in the reported frequency of depression [27], probably owing to differences in methods of diagnosing its symptoms. Identification of patients with stroke who have depression can be difficult when there are language and cognitive impairments [28]. Those with post-stroke depression might be less likely to participate in rehabilitation therapies, be less compliant with medications, feel more fatigue, have less appetite, and generally have poorer post-stroke outcomes [29,30]. Post-stroke depression can also contribute to post-stroke mortality [31]. Thus, future studies should assess whether patients meet precise diagnostic criteria for post-stroke depression. In addition, stroke can provoke disturbances in autonomic control and predispose patients to cardiac complications such as myocardial infarction, angina, and congestive heart failure [32,33,34]. In a previous study, 1.5% of subjects developed gastrointestinal bleeding during hospitalization [35]. Gastrointestinal bleeding has a significant effect on stroke morbidity and mortality [35,36]. Further studies are therefore necessary to assess patients with post-stroke cardiac complication and/or gastrointestinal bleeding.
Second, since the institutions participating in this cohort study assessed the presence or absence of post-stroke medical complications by reviewing medical records, it is possible that unrecorded minor complications were overlooked. Third, since there were no data regarding the timing of post-stroke medical complications, it was difficult to determine whether the complications occurred immediately after stroke or during hospitalization for rehabilitation. We expect fewer post-stroke complications in patients who received active rehabilitative therapy, although this will require a more detailed analysis in future studies. Finally, post-stroke medical complications after discharge were not investigated; therefore, the long-term incidence of complications remains unclear. Further studies should determine the complications that interfere with recovery in the acute and chronic stages and seek measures to decrease the incidence of such complications.
Nevertheless, the present study is significant in that it offers a comprehensive evaluation of the incidence of post-stroke medical complications in Korean patients with first stroke episodes and the factors affecting these complications. This report thereby provides considerable analysis and key information on the association between prognosis and factors affecting post-stroke functional recovery.
In conclusions, our results suggest that post-stroke medical complications affect functional recovery. However, the majority of complications are preventable and treatable; therefore, the long-term quality of life of individuals who experience stroke can be improved by providing timely, appropriate care, either through stroke prevention projects or post-stroke care projects. Furthermore, special care should be provided to patients with risk factors for post-stroke medical complications including old age, hemorrhagic stroke, poor initial motor function, poor swallowing function, and pre-existing morbidities.