INTRODUCTION
Fluoroscopy-guided cervical nerve root block is conventionally used for managing cervical radiculopathy. In general, the needle approach in the posterior aspect of the foramen has been popularly used to avoid the penetration of critical blood vessels such as the vertebral artery [1]. However, always underlying such a procedure is the risk of critical complication of unintentional blood vessel injury despite following strict guidelines, such as carefully performing a fluoroscopy-guided needle approach in the posterior aspect of the foramen to minimize the inherent risks.
A survey by Ma et al. [2] of 1,036 consecutive nerve blocks (specifically, fluoroscopically-guided extraforaminal cervical nerve blocks) revealed a complication rate of 1.64%. Most of the serious reported complications were commonly associated with intravascular injections, which resulted in infarction of the spinal cord and the brainstem [3].
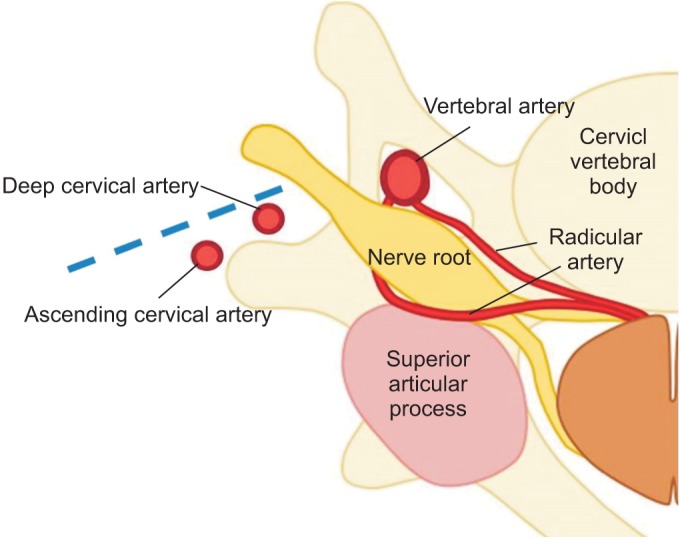
In previous studies, the authors suggested that unexpected anatomical variations of cervical arteries might be the cause of unintended intravascular injections [3]. In a cadaveric study by Huntoon [4], 7 out of 95 cases (7.3%) showed that some critical artery branches extending from the vertebral, ascending, and deep cervical arteries were located in the posterior aspects of the foramen, which are vulnerable to the conduction of routine transforaminal epidural steroid injections (Fig. 1). Also, the Hoeft et al. [5] cadaveric study showed an anatomical variation of the radicular artery entering the cervical intervertebral foramen.
In the case series study showing the feasibility of administering an ultrasound-guided cervical nerve root block for 10 patients, Narouze et al. [6] reported that 2 patients had critical arteries at the posterior aspects and 1 patient had a critical one continuing medially into the foramen.
In this study, the authors suggest that the anatomical variation of cervical arteries is much more than has previously been known [6]. Until now, there has been no definitive report regarding the prevalence of critical blood vessels around each cervical nerve root level in the clinical setting.
So in this study, we have tried to evaluate the prevalence of vulnerable blood vessels around each cervical nerve root prior to cervical nerve block in the clinical setting.
MATERIALS AND METHODS
Participants
This study included 74 patients with cervical radiculopathy who received ultrasonography-guided nerve block at an outpatient clinic from July 2012 to July 2014 in CHA Bundang Medical Center and Seoul National University Bundang Hospital. Medical records and ultrasound images were retrospectively analyzed.
Ultrasound evaluation
Before the actual injection of the steroid was performed, we evaluated the vulnerable blood vessels around each C5, C6, and C7 nerve root of the patient's painful side, with Doppler ultrasound imaging. Ultrasound evaluations were performed using a standard ultrasound device (Philips iU22 DS; Philips Medical Systems, Cleveland, OH, USA) and a high-frequency linear transducer (5ŌĆō12 MHz). With patients being placed in a supine position, their heads were rotated 30┬░ to 40┬░ away from the painful side [7].
To determine spinal level, two methods were used. First, to determine the C7 level, the transducer scanned the lateral aspect of the neck transversally to identify the transverse process. The C7 transverse process differs from that of others by its having no prominent anterior tubercle [8]. Another way is to follow the vertebral artery, which runs anteriorly at the C7 level till arriving at the C6 level, where it enters the foramen in 90% of cases [9].
Definition of vulnerable blood vessel
The term ŌĆśvulnerable blood vesselŌĆÖ was defined as being an artery within 2 mm distance from the target of injection or located at the site of the projected pathway of the imaginary needle if it were to be placed in the posterior aspects of the intervertebral foramen [4].
RESULTS
Demographics
Total of 74 patients were included in the study, with an average age of 54.64 years (range, 28ŌĆō77 years). Vulnerable blood vessels around each C5, C6, and C7 nerve root of the patient's painful side were all evaluated with Doppler ultrasound imaging, resulting in imaging of 74 cases of C5, C6, and C7 each.
Evaluation of vulnerable blood vessels
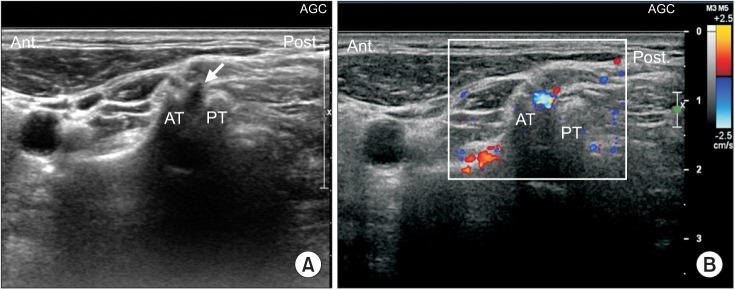
In all cases, cervical transverse processes and spinal nerve levels were well identified in the short axial ultrasound view, with the anterior tubercle and the posterior tubercle well visualized as the ŌĆś2-humped camelŌĆÖ sign (Fig. 2).
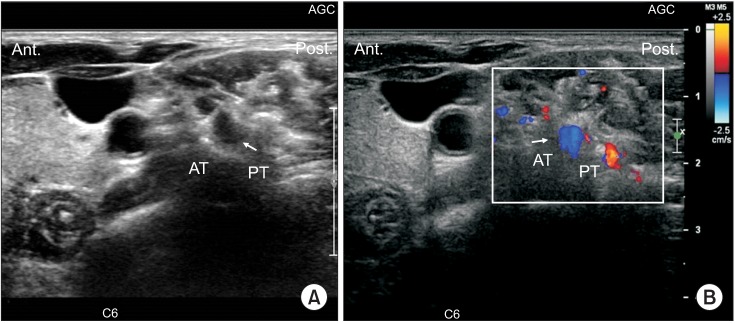
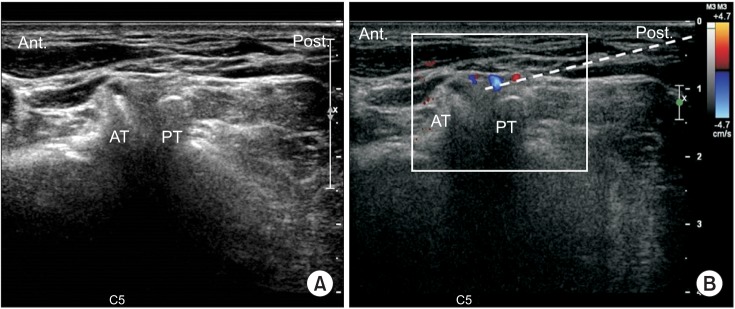
Short axial view of color Doppler ultrasound imaging revealed the presence of a vulnerable blood vessel at the targeted nerve root in the intervertebral foramen at each nerve level (Figs. 2, 3). Out of 74 cases, the C5 level had 2 blood vessels (2.7%), the C6 level had 4 blood vessels (5.45%), and the C7 level had 6 blood vessels (8.11%) close to each targeted nerve root (Table 1). The presence of vulnerable blood vessels at the site of an imaginary needle's projected pathway to the targeted nerve root in the intervertebral foramen were also revealed by short axial color Doppler ultrasound imaging (Fig. 4). Out of 74 cases each, the C5 level had 2 blood vessels (2.7%), the C6 level had 5 blood vessels (6.75%), and the C7 level had 4 blood vessels (5.45%) at the site of the imaginary needle's projected pathway to the targeted nerve root (Table 1). These blood vessels could have easily been injured by a conventional fluoroscopy needle approach.
In total, the C5 level had 4 blood vessels (5.45%), the C6 level had 9 blood vessels (12.16%), and the C7 level had 10 blood vessels (13.51%) either at the targeted nerve root or at the site of the imaginary needle's projected pathway to the targeted nerve root (Table 1).
DISCUSSION
Until now, there has been no study showing the prevalence of vulnerable blood vessels around each cervical nerve at the root level, by ultrasound, in the clinical setting. While the previous studies of researchers such as Huntoon [4] and Hoeft et al. [5] have shown blood vessel distributions in cadavers, what was remarkable about this study is that it tried to actionably reveal the actual distribution and prevalence of such blood vessels in the clinical setting.
Cervical spinal arterial branches arise mainly from the vertebral, ascending cervical, superior intercostal, and deep cervical arteries. These spinal arterial branches pass through the intervertebral foramina just adjacent to the spinal nerves and continue as radicular arteries. Then, the radicular artery penetrates the dura to supply the nerve roots and to join the anterior and posterior spinal arteries. This radicular artery is a major source of blood for the nerve root and the spinal cordŌĆöso damage to this artery, such as through intra-articular injection, can lead to serious complications [5].
In the study by Baker et al. [10], even real-time contrast fluoroscopy was considered to be insufficient, so it is recommended to check arterial filling using real-time fluoroscopy with digital subtraction, for the detection of unintentional intravascular injections. Also, the fluoroscopy method can increase the patient's and the operator's exposure to radiation. So to overcome the shortcomings of fluoroscopy, ultrasonography has recently and rapidly been becoming an alternate technique for intervention [11]. In the previous study, showing the effectiveness of ultrasound as compared with fluoroscopy, ultrasound-guided intervention showed comparatively equal efficacy in pain relief and comparatively equal efficacy in functional assessment with fluoroscopy-guided injection [6,12]. Other than the advantage of involving no radiation exposure, ultrasonography has the capability of visualizing structures such as soft tissues, blood vessels, nerves, and needle-tip placement on real-time imaging scans; and it can also allow for the observation of the spread of injectate [6].
Back to the results of this study: There was an unneglectable prevalence of vulnerable blood vessels either at the targeted nerve root or at the site of the imaginary needle's projected pathway to the nerve root. This result means that if transforaminal epidural injection with fluoroscopy were to be done as the usual protocol (to approach from the posterior aspect) without ultrasound examination in those patients, then the likelihood of injuring a critical blood vessel is high. The likelihood that unexpectedly injuring a critical blood vessel located in the posterior aspect of a patient's foramen (either at the targeted nerve root or at the site of the imaginary needle's projected pathway to the nerve root) is approximately one out of 10. Also, it shows that lower the cervical spinal nerve roots, a higher prevalence of vulnerable blood vessels both at the target site and at the site of the imaginary needle's projected pathway to the nerve root. Therefore, needs to be more cautious while conducting lower cervical nerve root block and ultrasonography can be helpful to avoid the unintentional blood vessel injury.
Ultrasound, however, has some drawbacks such as limited visualization at deeper levels, especially under bony structures, and relative dependency on operator experience for fine imaging and intervention. In contrast to ultrasound, fluoroscopy-guided injection has the advantage of making bony structures clearly visible. By using ultrasound as a prior examination before fluoroscopy-guided transforaminal injection, we can not only maximize the benefits of these two examinations, but we can also minimize the cost of catastrophic complications that patients could suffer.
Our present study had some limitations. Firstly, we only examined the C5-7 cervical root level, rather than the whole cervical level. However, the prevalence of C5-7 cervical radiculopathies accounts for about 80% of total cervical radiculopathies [13]. Considering the prevalence of cervical radiculopathies as shown in the previous study, our study result may be useful in clinical settings. Still, though, further evaluation of the upper cervical level may be needed. Secondly, the study lacks detailed clinical data, sociodemographic data, and long-term clinical outcome data. In this study, we could not evaluate the efficacy of ultrasound-guided cervical root block, but rather we only showed the prevalence of vulnerable arteries at each cervical root level. Therefore, assembling a conglomeration of more clinical data regarding long-term outcomes and correlating these outcomes with the prevalence of vulnerable arteries near the cervical root will enhance the value of the present study.
Also, this study did not distinguish between whether each proposed ŌĆśvulnerable blood vesselŌĆÖ was an artery or a vein. If it were an artery, we still could not recognize which artery it was and where it had come from. So in a future study, it would be more worthwhile to distinguish between arteries and veins and to trace each blood vessel to see where it branches from.
In conclusion, to prevent unexpected critical complications involving vulnerable blood vessel injury during the cervical nerve root block, it is recommended to routinely evaluate the vulnerable blood vessels around the cervical nerve root using Doppler ultrasound imaging prior to the fluoroscopy-guided cervical nerve root blockŌĆöespecially for lower cervical nerve root level injections.