INTRODUCTION
Movements of the thumb are carried out by 4 intrinsic and 4 extrinsic muscles. The intrinsic muscles of the thumb are comprised of the abductor pollicis brevis (APB), opponens pollicis (OP), adductor pollicis (AP), and flexor pollicis brevis (FPB); the extrinsic muscles include the extensor pollicis brevis (EPB), extensor pollicis longus (EPL), abductor pollicis longus (APL), and flexor pollicis longus (FPL). Congenital anomalies involving these muscles are mostly related to thenar hypoplasia or duplication of EPB or APL [1-4]. Agenesis of thenar muscles could lead to weakness and decreased dexterity of the thumb by limited abduction and opposition. Variations of the EPB or APL tendon, such as duplicated or multiple tendons, are very common. However, these variations have little effect on the hand function, but they could cause wrist pain by occasionally triggering entrapment syndrome.
The EPL muscle, which is one of the thumb extensor muscles, is the only muscle of the 3rd extensor compartment of the wrist. This muscle originates from the dorsal surface of the ulna and inserts on the dorsal base of distal phalanx of the thumb to extend at the metacarpophalangeal (MCP) and interphalangeal (IP) joint. Anatomical variations of this extensor muscle are known to be very rare, and published reports on this topic were focusing on duplication or anomalous course of this muscle. The EPL is considered as the most consistent structure with the least variation among the muscles involved in movement of thumb [5].
We report a rare case of major anatomical variation of the EPL, which was composed of anomalous course of the EPL with absences of thenar muscles and the muscles in the 1st extensor compartment.
CASE REPORT
A 10-year-old girl visited the outpatient clinic to evaluate the flatness of the right hand, which was incidentally noticed by her parents. She is left-handed, and she had no history of specific discomfort or functional limitation in the right hand. There was no special problem during the prenatal and perinatal period, as well as any family history of any hand anomaly.
Severe atrophy of the thenar eminence of her right hand was identified (Fig. 1A). We also recognized that the IP joint of the thumb was not fully extended (Fig. 1B). In addition, the EPB and APL tendons were not obvious enough to make skin fold during extension of the thumb. Passive range of motion of the thumb was normal. Active range of motion in adduction and flexion of her thumb was normal, whereas those of abduction and extension showed limitations. She could extend her thumb to neutral position, whereas the opposite thumb could hyperextend. This limitation did not seem to influence her functional movement of the thumb. Passive and active range of motions of her wrist and other fingers, except the thumb, were within normal range. There were no abnormal physical findings and function in the other extremities. In addition, we could not find any abnormalities in the head and neck, as well as chest and abdomen.
Muscle power was checked by manual muscle testing and precision dynamometer G200 (Biometrics Ltd., Newport, UK). In manual muscle testing, the muscular strength of shoulder, elbow, wrist, and other fingers, except the right thumb was normal. In the right thumb, strength of flexion and adduction exhibited good grade, whereas extension and abduction were fair to good grade. Grip strength of the right hand, checked by the dynamometer, was 60% of that of the left hand. Sensory test of the right upper extremity, including the thumb, was normal. Tinel's sign and Phalen's test on the right side showed a negative result.
In the motor and sensory conduction studies on the right hand, compound muscle action potential of the median nerve was not evoked, but other nerve conduction studies, including the median sensory nerve, ulnar motor and sensory nerve conduction studies, were within a normal range. In the needle electromyography, there were neither insertional activities nor volitional motor unit action potentials in the APB muscle. These findings were in accordance with absence of this muscle.
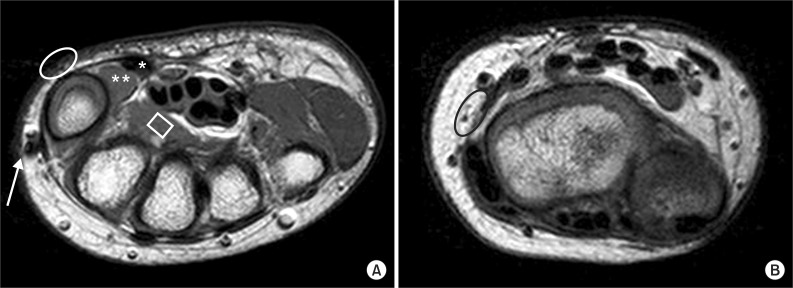
Bones and joint of her right extremity showed no abnormality in the simple X-ray findings. On magnetic resonance imaging (MRI) study, the FPL tendon, AP and FPB muscles were observed in the palmar side, showing a normal course to an insertional point. However, the APB and OP muscles were not seen (Fig. 2A). In the dorsal side, the APL and EPB tendons were not observed (Fig. 2B). The EPL tendon was found, but it showed an abnormal insertion toward the radial side of the proximal phalanx, not to the distal phalanx (Fig. 3).
She could control her right hand as possible as the greater part of the functional movement, and there were no limitations of the activities of daily living, within the range of her age; therefore, we didn't consider surgical intervention. However, we recommend that she needs to get occupational therapy and education to prevent retardation of hand function development, because the affected hand was nondominant and has overt weakness.
DISCUSSION
Unlike relatively common anatomical variation of the APL and EPB, that of the EPL has not been commonly defined. It could be divided into duplication and anomalous course. Duplication of the EPL means supernumerary tendons to the thumb in the presence of normal EPL and accessory tendon split off from other extensor muscles, such as extensor indicis proprius. Anomalous course of the EPL passes through other compartment out of the 3rd compartment. Anomalous course of the EPL is known to be much rare than duplication, as much as 5 cases were reported previously [6]. In our case, the EPL passes wrist though the 3rd compartment, but it is out of the 3rd compartment at the carpal bone level and inserted on the radial side of the thumb as the 1st compartment. Therefore, this case is classified as an anomalous course of the EPL.
Based on MRI findings, severe limitations of the thumb function, including abduction resulting from multiple agenesis of the thumb muscle were presumed in the case. In general, patients with agenesis of thenar muscle are known to have functional limitations in powerful grasp and fine pinch. These limitations are usually associated with the weakness of opposition [7], a complex movement, involving abduction, flexion and pronation of a thumb. However, this patient did not show significant functional limitations in the affected hand, including abduction and opposition. We assumed that her relatively preserved abduction of the thumb was from the abnormal insertion of the EPL muscle, despite absence of the APB muscle. In case of normal insertion to the distal phalanx, the EPL muscle would extend the MCP and IP joint of the thumb. However, her EPL muscle inserted to the radial border of the MCP joint with covering dorsal side of metacarpal bone, and activation of this muscle generated rotation moment of the thumb that diverted the axis of movement from extension to abduction.
If there are functional limitations of hands due to thenar agenesis, surgical reconstruction, such as opponensplasty, can be considered. Opponensplasty is a procedure for restoration of thumb abduction, including transfer of the abductor digiti minimi, flexor digitorum superficialis, and others [8]. If there is a significant weakness in thumb extension or abduction due to the absence of the APL and EPB, transfer of the palmaris longus tendon to the thumb could be performed [9]. Anomalous course of the EPL could be a cause of wrist pain as triggering tenosynovitis. If conservative treatment based upon de Quervain's disease is not effective, releasing or transposing of anomalous tendon could be performed. However, she did not complain of any discomfort, such as limitation of functional activity of hand or wrist pain; thus, we did not consider surgical intervention.
Thumb abnormalities may be present as an isolated anomaly or as a component of a syndrome. Especially, thumb hypoplasia, such as absence of the thumb muscles can be present with congenital heart defects as in Holt-Oram syndrome, or pancytopenic anemia as in Fanconi syndrome, or dwarfism in Cornelia de Lange syndrome, or Duane anomaly of the eyes and deafness as in Okihiro syndrome, or as a part of VACTERL association, or thrombocytopenia with absence of radius [10]. Although our patient showed no abnormality in history and physical examination without thumb anomaly, it is needed to evaluate the overall systemic review and physical examination from head to toe for patients of congenital thumb hypoplasia.