INTRODUCTION
Work-related Musculoskeletal Disease accounts for the largest proportion of white-collar worker's diseases both in Korea and abroad. White collar worker's WMSD as wells as blue-collar workers occurs occasionally, but it still receives relatively less attention.1
Most office workers perform computer-aided work tasks in uncomfortable positions for long hours, causing health problems in the musculoskeletal system. The proportion of WMSD in work-related disease area is gradually increasing. Specifically, workers using visual display terminals (VDT) perform repetitive movements requiring muscular tension, leading to sudden fatigue and pain. One third of VDT workers experience pain in the neck and back. Moreover, VDT workers' static posture leads to forward flexion of the neck and static muscle tension, greatly affecting the neck and shoulder area.2
Once the pain has persisted for more than 3-6 months, it becomes chronic. This becomes a disease itself causing depression, anxiety, somatization, insomnia, etc.3-5 The continuous pain appears to be justified and becomes a problem in daily life and also in the workplace, even to the point of diminished social activities and quality of life.5,6 Therefore if the diagnosis of depression is overlooked, it not only reduces the treatment progress but it also worsens the symptoms. If it becomes a chronic disease, it will lead to a lower quality of life.7-9
Currently throughout the world, many depression scales have been developed and are being used. Many widely-used depression scales, both in Korea and abroad, are the Beck Depression Inventory (BDI), Hamilton Depression Scale, MMPI-Depression Scale, Zung's Self-Rating Depression Scale (SDS), Geriatric Depression Scale (GDS), Center for Epidemiologic Studies Depression Scale (CES-D), and PRIME-MD.10,11
In Korea, the most commonly used depression scales for diagnosis are SDS and BDI. Among these two, BDI consists of 21 questionnaires developed by the author after organizing a comprehensive psychotherapy to patients with depression and their responses.
There have been many studies on screening the emotional discomfort variables of chronic pain patients, such as depression, anxiety and etc, and relativity between the chronic pain and the symptoms,4,12-15 but studies on the connection between the chronic pain, caused by WMSD, and depression are so far lacking. Therefore, the present study was undertaken to evaluate the association of WMSD and depression.
MATERIALS AND METHODS
As part of the WMSD Screening Program focused on white-collar workers of the National Health Insurance and National Pension Service, this study conducted a survey on 724 men and women who mainly use VDTs and experienced WMSD.
From May, 2009 to August, 2009, 5 psychiatrists visited the branches of the National Health Insurance and National Pension Service and conducted diagnosis tests, medical history records and physical examinations to screen WMSD. Patients were classified into 4 groups: "Myofascial pain syndrome (MPS)", "Herniated intervertebral disk (HIVD)", "Tenosynovitis" and "others". The HIVD group was diagnosed by medical records of neck pain, low back pain, muscle weakness in characteristic myotome through the administration of the manual muscle test, nerve segments through a neurological examination, and loss of the deep tendon reflexes through each part of the challenge test. When cervical HIVD was suspected, the Sperling test and axial loading test were performed and shoulder abduction relief signs and Lhermitte's signs were checked. When lumber HIVD was suspected, the straight leg raising test and femoral nerve stretching test were performed and Lasegue's signs were checked. Tenosynovitis group included subjects with lateral and medial epicondylitis of the elbow, the Biceps brachii tendinitis, Flexor carpi ulnaris tendinitis, Flexor carpi radialis tendinitis, DeQuervain's tenosynovitis, and Extensor carpi ulnaris tendinitis, and the group was confirmed with the characteristics of the symptoms and pains of each area. In particular, DeQuervain's tenosynovitis was diagnosed when there were characteristic swelling and pain in the Abductor pollicis longus and Extensor pollicis brevis tendons and positive results in the Finkelstein test. Other groups included patients with Rotator cuff syndrome, adhesive capsulitis, and carpal tunnel syndrome. This group followed examinations of the joint motion range of the shoulder joint, manual muscle test, Supraspinatus or Infraspinatus atrophy for any pain, and provocation tests such as the Neer test and Yergason's test. When carpal tunnel syndrome was suspected, the subject was verified by the Phalen's test and Tinel's sign. The MPS group included pains that other groups did not include, after diagnosing trigger points and taut bands of the pain-related muscle.
In addition, all subjects were asked to fill out the Korean Beck Depression Scale (K-BDI) and expressed their pain using a Visual Analogue Scale (VAS). According to Steer and others,16 depression is classified as 0-9 for normal, 10-15 mild, 16-19 mild to moderate, 20-29 moderate to severe, and 29+ severe based on the BDI score. Therefore, in this study, the subjects were considered having depression when the K-BDI score was higher than 10 points.
After that, we investigated the prevalence of depression and the association between each disease and depression. Also, we compared pain intensity between the depression and non-depression groups.
All data was analyzed using SPSS for windows 13.0 version. The correlation of K-BDI score, VAS, and WDSD was confirmed with the Pearson correlation test and χ2 test. When p-value was under 0.05, it was considered statistically significant.
RESULTS
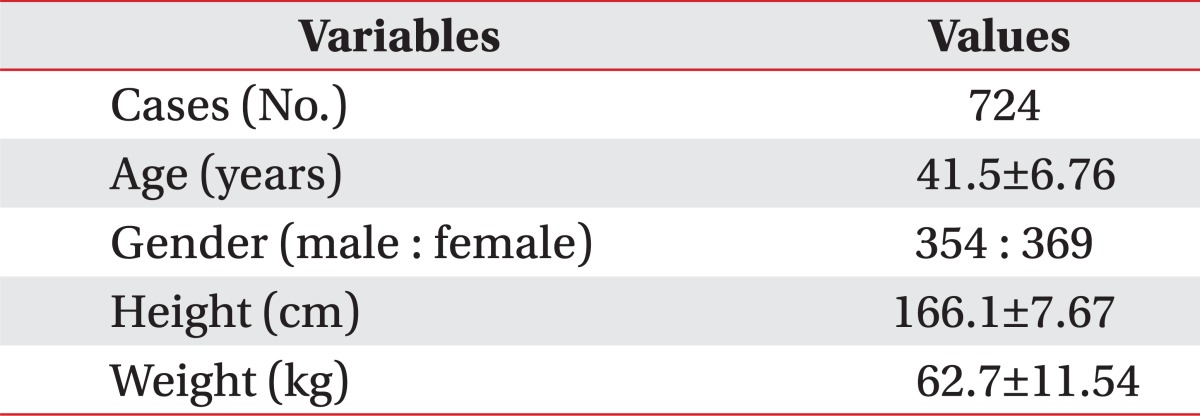
Subjects who participated in this study were a total of 724 people with age of 41.5±6.76 years old, height of 166.1±7.67 cm, and weight of 62.7±11.54 kg. Among all subjects, men were 354 and women were 369 (Table 1). Hours of daily computer use was 7.7±2.08 hours. The MPS group had 466 people (64.4%), the HIVD group had 116 people (16.0%), the Tenosynovitis group had 112 people (15.5%), and other groups had 134 people (18.5%). Patients with 2 or more diseases numbered 167, comprising 23.1% of all subjects.
All subjects' K-BDI scores were 8.7±6.68 points. Subjects with 10 or more K-BDI scores were classified as having depression and 267 subjects, 37.9% of all, were considered as having depression. The prevalence of depression among women was 40.7% (150 people), which was higher than the prevalence of depression among men, 33.1% (117 people). There was no correlation between age and depression.
When the intensity of pain was scaled milde (1-3 points), moderate (4-7 points), severe (8-10 points) according to VAS scores, each intensity scale's prevalence of depression with mild intensity was 25.7%, moderate intensity with 42.3%, severe intensity with 52.5%. As the pain intensity increased, the more a person was likely to have depression.
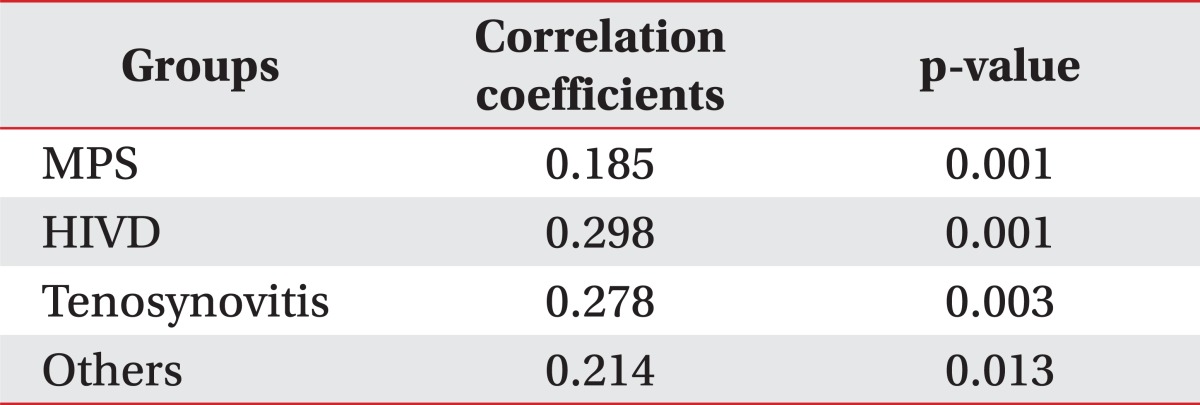
Concerning all subjects, the K-BDI score and VAS score had a weak correlation (r=0.204, p<0.01). In particular, the HIVD group had the correlation coefficient of 0.298 between BDI score and VAS score, showing the highest correlation coefficient (Table 2).
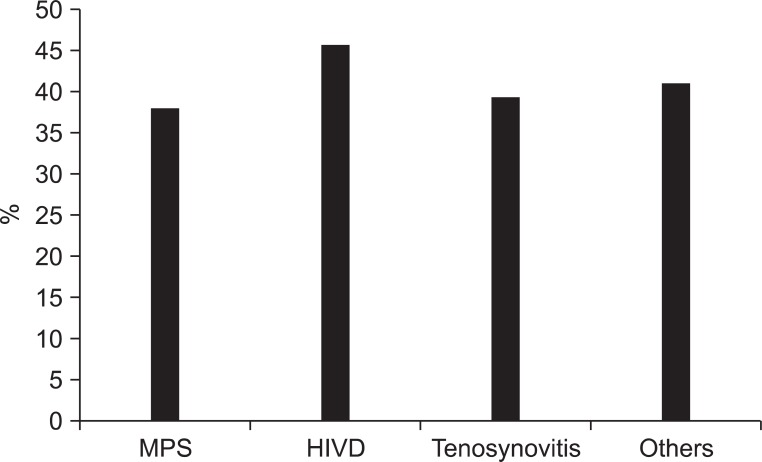
Each disease group had the prevalence of depression as follows: MPS group with 38%, HIVD group with 45.7%, Tenosynovitis group with 39.3%, and others group with 41% (Fig. 1).
The VAS score of the group with depression was 5.02 points, significantly higher than the group without depression, with 4.10 points. The comparison result between groups with or without depression was the same as Fig. 2 shows. Within the MPS group, the group with depression had aVAS score of 4.82±1.94 points, relatively higher than the group without depression, 4.10±2.14 points. Also, within the HIVD group, the group with depression had a VAS score of 5.87±1.82 points, relatively higher than the group without depression, 4.62±2.20 points. Within the Tenosynovitis group, the group with depression had a VAS score of 4.95±1.78 points, higher than the group without depression, 3.81±2.19 points. Same in others group, the group with depression had 5.15±2.10 points, significantly higher than the group without depression, 3.91±2.27 points (p<0.01).
DISCUSSION
Since 1980, there has been many depression-related studies after it became known that depression is an important factor affecting the status of patients.17 It is already known that the intensities of pain and depression are closely related, especially to the pain in the backbone and other chronic pain.18-21 This present study was conducted to investigate the association between WMSD and depression.
According to Cho and others,22 the average prevalence of depression among Korean male workers is 14.7% and among females 18.6%. This study's subjects who are workers in the health and social services had a prevalence of 24.1%. This is far lower than this study's result of 36.9% as WMSD subjects' prevalence of depression. We can assume that WMSD is closely related to the prevalence of depression. According to the subtypes of WMSD, the prevalence of depression had great differences. Specifically, the HIVD group showed 45.7% of the prevalence of depression, far higher than other disease groups. These results explain the association between pain and depression that other studies already have revealed. We can consider diseases like HIVD that have high tendency to develop as chronic pain have a closer relationship to depression.
The VAS score, which assesses the intensity of pain, appeared to be higher in groups with depression than in groups without depression. Considering the existence of significant association between K-BDI score and VAS score, we can conclude depression and the pain intensity have a mutual influence on each other. This shows the same result of previous studies.2-4,18-21 The correlation of BDI and VAS scores was also the highest in the HIVD group.
The limitation to this study is that it is unclear whether the depression among computer-using office workers is caused by the pain of WMSD or other causes, such as stress coming from tasks using a computer or other environmental factors. Also when subjects were diagnosed with the disease, the diagnosis was simply conducted with an examination of medical records and physical examination, not with methods of imaging diagnostics or blood sampling. In the previous studies, it has been revealed that chronic WMSD has an association with depression and that work-related stress also affects depression. However, this study focused on only the office workers who perform computer-related tasks, which led to discovering the association between the prevalence of WMSD and depression.
Since the HIVD group had a high prevalence rate of depression and also a correlation between K-BDI and VAS scores, greater than any other groups, future studies are needed to investigate the difference of various WMSD and HIVD and the effect of depression on HIVD by examining the psychology of patients. Also, a more efficient method of depression diagnosis is needed to offer a better environment for office workers.