INTRODUCTION
Balance is the ability to maintain the center of gravity of the body over the base of support.1 Although various tools are used to measure balance, some measurement tools using scales require not only considerable time but also a considerable effort on the part of the examiner.2-4 In recent studies, some tools for measuring balance have a clinical limitation for use in healthy active people, because they are not sufficiently challenging.2
The Biodex Balance System (BBS) uses a balance platform and has been widely used to evaluate postural balance in recent years. The system is known to be a reliable test for the measurement of balance in healthy people and blind people.5-10 However, no studies have investigated which level of BBS (level 12: most stable and level 1: most unstable) better reflects the balance of patients.
The Timed Up and Go (TUG) test and the Single Leg Stance (SLS) test, both of which are being used to measure balance, are reliable and can be performed quickly and easily. The scores on these tests are also known to have significant association with the risk of falls.2-4 However, no studies have investigated the relationships between scores on these tests and those on the balance test using BBS.
The purpose of this study was to measure balance in healthy adults using the TUG, SLS and BBS and to investigate which stability level on the BBS is most useful for the assessment of balance by analysis of the correlations between TUG or SLS tests and the OSI (Overall Stability Index) at the various different BBS levels.
MATERIALS AND METHODS
Subjects
We recruited 73 patients, who were healthy enough to be capable of independent gait, from among those attending the Department of Rehabilitation Medicine in our hospital during the period June 1 to October 30, 2010. We excluded patients, who were incapable of independent gait for more than 10 meters, and those with hemiplegia, quadriplegia, spinal cord injury, peripheral polyneuropathy, radiculopathy, or a serious musculoskeletal disease. We also excluded patients with severe medical problems, such as severe hypertension, unstable angina, or chronic obstructive pulmonary disease.
Methods
The TUG, SLS, and BBS tests were performed in that order on subjects satisfying the inclusion criteria. The data obtained from the results of the tests were categorized on the basis of age, TUG score (<10 vs. ≥10 seconds) and SLS scores (>30 vs. ≤30 seconds).
Timed Up and Go (TUG) test
TUG is a test of functional mobility.11 When the examiner gave the start signal, subjects stood up from a seated position without the use of their hands, walked for three meters at a normal walking speed and then returned to sit in the chair. The time was measured in seconds, and practice was not allowed. The outcome variable was the mean time over two trials.11,12 High scores (long times) indicate poor balance.
Single Leg Stance (SLS) test
The subjects were asked to stand for as long as possible on their more comfortable leg, and the time was measured in seconds. Each subject performed three trials, and the best result of the three trials was recorded.13 The test was stopped if the stance foot shifted in any way, the non-stance foot touched the ground or the SLS time was 60 seconds or more.14 Low scores (short times) indicate poor balance.
Biodex Balance System (BBS) test
The Biodex Balance System (Biodex Medical Systems Inc., New York, USA) consists of a movable circular platform, and the level of resistance of the foot platform can be altered (Fig. 1). The BBS level indicates the stiffness or stability of the foot platform, with level 12 being the most stable and level 1 the most unstable. The stability settings of 12 through 1 allow the foot platform a full 20 degrees of deflection from level in any direction. The platform is interfaced with computer software, which enables the device to serve as an objective assessment of balance. We assessed bilateral stance using a total of 6 levels between levels 12 and 2.
The subjects were positioned barefoot with arms across their chests and hands on their shoulders. During the assessment, the subjects tried to maintain their balance by themselves looking at a target on a screen and keeping a dot marker at the centre of the target. At each stability level, the test was performed three times (each test lasted for 15 seconds), and the mean stability index was calculated. The resting time between the tests for a given level of stability was 10 seconds, and the interval between tests for different levels of stability was 30 seconds.
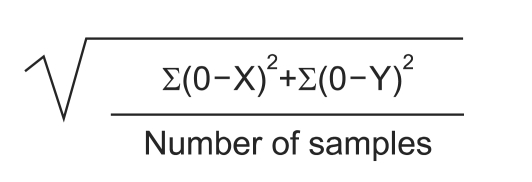
The OSI was used as the stability index. The BBS software sampled the degree of tilt from level in the mediolateral (X) and anteroposterior (Y) directions, and these signals were converted to OSI values (Fig. 2). A high stability index represents the angular excursion of the subject's center of gravity and is indicative of a high degree of movement during a test (i.e.poor balance). If the subjects took their hands from their shoulders, they were asked to return them to their initial position. However, if they were going to fall or grasped the hand-rail, the test was stopped.
Statistical analysis
SPSS 14.0 version for Windows was used for all statistical analyses. The Mann-Whitney U and Kruskal-Wallis tests were used to compare by group the mean times on the TUG and SLS, and the mean OSI values on the BBS. Correlation coefficients were calculated to assess the degrees of association between the BBS and OSI values and the TUG or SLS scores by group. When the number of subjects was 30 or more, the Pearson correlation coefficient was used; and when the number of subjects was less than 30, the Spearman correlation coefficient was used.
RESULTS
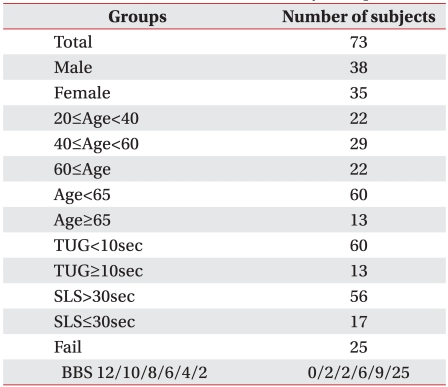
Characteristics of the subjects (Table 1)
The gender distribution of the 73 subjects was approximately equal (38 males, 35 females), and the mean age was 48.9±15.4 years. The numbers of subjects aged 20-39, 40-59 and 60 or more years were 22, 29 and 22, respectively. The numbers less than 65 years of age and 65 years or older were 60 and 13, respectively. When the subjects were grouped on the basis of their TUG test scores, the numbers of subjects taking less than 10 seconds and 10 seconds or longer to complete the task were 60 and 13, respectively. Similarly for the SLS test, the numbers of the subjects standing for 30 seconds or less and longer than 30 seconds were 17 and 56, respectively. A total of 25 subjects failed to perform at level 2 on the BSS, which the most unstable of the six settings used.
Comparison of groups on the TUG and SLS (Table 2)
On the TUG test, the older subjects showed worse balance (p<0.01) and, while the group with SLS times of 30 seconds or less showed worse balance on the TUG than the group with SLS times over 30 seconds, this difference was not statistically significant.
On the SLS test, the older groups again showed worse balance (p<0.01), and, although the group with TUG times of 10 seconds or more showed worse balance than the group with TUG times under 10 seconds, this difference was not significant.
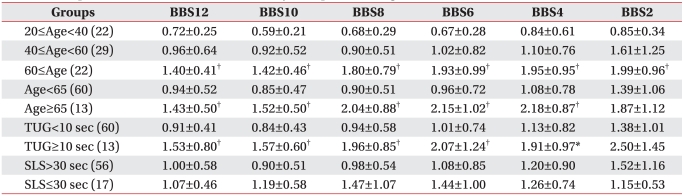
Comparison of groups on the OSI according to BBS levels (Table 3)
On the OSI, the older age group showed worse balance at all six BBS levels. When the subjects were grouped in terms of under 65 years or 65 years and older and on the basis of under 10 seconds or 10 seconds and longer on the TUG test, the 65 years and older group and the group with TUG times of 10 seconds or more both showed worse balance at all BBS levels, except at level 2. When the subjects were grouped on the basis of the SLS test, the group with SLS times of 30 seconds or less showed worse balance at every BBS level than the group with times over 30 seconds, but none of the differences were significant.
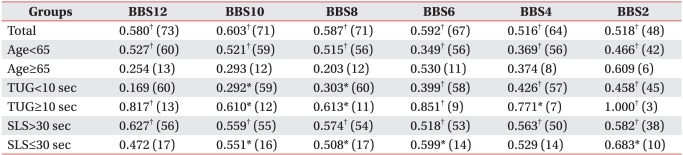
Correlations between the TUG and OSI by groups (Table 4)
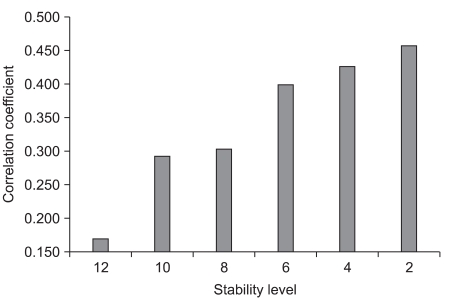
In the total group of subjects and in the groups of subjects aged under 65 years, those with TUG times of 10 seconds or more and those with SLS times over 30 seconds, the TUG scores and OSI values were significantly correlated at all BBS levels. The correlation was highest at level 10 (0.603, p<0.01) in the total group of subjects. For those aged under 65 years and for those with SLS times over 30 seconds, the correlations (0.527, p<0.01 and 0.627, p<0.01, respectively) were the highest at all 12 levels. In the group with TUG times of 10 seconds or more, excepting the levels at which the numbers of subjects included in the analysis were 10 or less, the correlation was highest at level 12 (0.817, p<0.01). In the group with TUG under 10 seconds, significant correlations were observed from levels 10 to 2, with level 2 showing the highest correlation (0.458, p<0.01). In this group, it is notable that the correlation gradually increased from level 10 to 2 (Fig. 3). No significant correlations were observed in the other groups.
Correlation between the SLS and OSI by groups (Table 5)
In the total group of subjects, a significant correlation was observed only at level 8 (-0.299, p<0.05). In the group with TUG times of 10 seconds or more, significant correlations were observed only at levels 8 (-0.598, p<0.05) and 10 (-0.598, p<0.05). For the other groups, no significant correlations were found at any BBS level.
DISCUSSION
This study of healthy adults examined the OSI values obtained from the BBS and compared them with the measures on two existing manual balance tests, which that do not use a mechanical device. When the TUG and OSI values were compared, the correlation was highest at level 12 of the BBS in the groups with ages under 65 years, TUG times of 10 seconds or longer, and SLS times over 30 seconds. However, in the group with ages under 65, correlation coefficient varied little between levels 12 to 8 (from 0.527 at level 12 to 0.515 at level 8). In the group with TUG times of 10 seconds or more, the correlation coefficient was higher at levels 6 (0.851, n=9) and 2 (1.000, n=3) than at level 12, but these correlations were difficult to interpret because of the small number of subjects at each level (less than 10). In the group with SLS times over 30 seconds, except for level 12 (0.627) and level 6 (0.518), the differences between the correlations at the other levels were small (from 0.559 at level 10 to 0.582 at level 2). In the total group of subjects, although the correlation was highest at level 10, the differences between the correlations were small from level 12 to 6 (from 0.580 at level 12 to 0.603 at level 10). In previous studies in which balance was measured using the BBS, different levels of the BBS were used, and no specific explanations were provided for why a particular level was chosen.5-10 Based on these result, we concluded that the OSI value is significant correlated with the TUG score, and that healthy adults can be satisfactorily assessed at relatively easy BBS levels.
Before our study began, it was expected that balance would be better in younger subjects and among subjects, who obtained times of less than 10 seconds in the TUG test and longer than 30 seconds on the SLS test. In addition, we predicted that in these groups, the correlations would be higher at a lower BBS level. In particular, the group with TUG times under 10 seconds was expected to have excellent balance. For this group, the correlation was higher as the difficulty level on the BBS increased. However, for the group with SLS times over 30 seconds, which was also expected to have a good balance, the correlation was high at a relatively easy level. Based on these results, we have concluded that, although both 10 seconds in the TUG test and 30 seconds in the SLS test could be predictors of fall risk, 10 seconds in the TUG test is a stricter criterion.3,4 Indeed, when TUG, SLS, and OSI values were compared for the group with SLS times over 30 seconds or TUG times under 10 seconds (Table 2), the balance was better in the group with TUG under 10 seconds. In the group with ages under 65 years, the correlation was also higher at a relatively easy level; in the groups classified by age, no significant correlation was observed. We therefore further concluded that the criterion of either age or 30 seconds in the SLS test has no important function in predicting balance in healthy adults. The other possible explanation is that, because a low BBS level is too unstable, even people with good balance may achieve a poor OSI, making it difficult to distinguish people with good balance from those with poor balance. In fact, only 48 subjects (65.75%) completed up to level 2 of BBS, which is lower than expected, even if the subjects were healthy adults. There was also a possibility that the subjects with poor balance might have achieved better balance results than their actual balance because of the learning effect as they advanced to the lower BBS level. In this study, a total of 18 measurements of balance (three for each level) were performed in each subject, and the test was conducted in the order of the highest level (most stable) to the lowest level (most unstable) of BBS, which is a limitation of this study. Based on these results, we considered that an adult, who is an athlete and therefore expected to have excellent balance, should to be tested at a difficult BBS level. However, in relation to this, further studies with different subject groups are needed.
When the SLS and BBS were compared in the total group of subjects, although the correlation was highest at level 8 on the BBS (-0.299, p<0.05), it was lower than the correlations between the TUG and the BBS. In the group with TUG times of 10 seconds or longer, although the correlations were relatively high at levels 10 (-0.589, p<0.05) and 8 (-0.679, p<0.05), these values may be inconsequential because the correlations were based on only 12 and 11 subjects, respectively. In the other groups, no significant correlations in the expected direction were observed, and where a significant correlation did arise, it was a positive rather than negative correlation. Based on these results, we concluded that the OSI values and SLS results are less correlated than the OSI values and TUG results. In the SLS test, the patients are allowed to stand on their comfortable leg.3,15 However, further studies are required to find ways to measure the SLS value by having the patients stand on their more uncomfortable leg.
In previous studies involving the SLS test, a time limit was used to reduce the ceiling effect and ensure accurate time distribution; the time limit varied by study (e.g., 30, 45, and 60 seconds).14,16-18 However, because a fall high-risk group was identified in recent reviews using a cut off of 30 seconds, it was considered that the ceiling effect would occur well beyond 30 seconds. In our use of the SLS test, we therefore decided 60 seconds was the time limit and that the subjects would be subdivided into groups based on a time score of 30 seconds.3,14
The BBS has three stability indices: the anteroposterior index, mediolateral index, and the OSI. Previous studies reported that the mediolateral stability index had almost no impact on the OSI and that the OSI was the most appropriate marker of the overall balance capability of a patient on a balance platform.5,19 For this reason, we used the OSI as the BBS measure in our investigation of the associations between the TUG, SLS and BBS scores. However, future studies are needed to explore the relationships between TUG, SLS and the other BBS indices.
Another limitation of this study was that not all BBS levels (from level 1 to 12) were used in the assessments of balance. Finally, this study was conducted on relatively healthy adults. This meant that, when the subjects were subdivided into groups based on factors, which could affect their balance, the numbers of subjects in the groups with an expected poor balance was too small.
CONCLUSION
In this study, we compared TUG and SLS measures with OSI values on the BBS in 73 healthy adults, who were capable of an independent gait. The results showed that the OSI of the BBS was correlated with the TUG scores and that, in most cases, it was highly correlated with the TUG scores at a relatively easy BBS level. It is therefore considered that the assessment of balance using the BBS should be performed at a relatively easy level, except for those patients expected to have excellent balance, such as athletes, whose balance assessment might more helpfully be performed at a relatively difficult level.