Effect of Pneumatic Compressing Powered Orthosis in Stroke Patients: Preliminary Study
Article information
Abstract
Objective
To evaluate the feasibility and effectiveness of a knee-ankle-foot orthosis powered by artificial pneumatic muscles (PKAFO).
Methods
Twenty-three hemiplegic patients (age, 59.6±13.7 years) were assessed 19.7±36.6 months after brain lesion. The 10-m walking time was measured as a gait parameter while the individual walked on a treadmill. Walking speed (m/s), step cycle (cycle/s), and step length (m) were also measured on a treadmill with and without PKAFO, and before and after gait training. Clinical parameters measured before and after gait training included Korean version of Modified Bathel Index (K-MBI), manual muscle test (MMT), and Modified Ashworth Scale (MAS) of hemiplegic ankle. Gait training comprised treadmill walking for 20 minutes, 5 days a week for 3 weeks at a comfortable speed.
Results
The 10-m walking time, walking speed, step length, and step cycle were significantly greater with PKAFO than without PKAFO, and after gait training (both p<0.05). K-MBI was improved after gait training (p<0.05), but MMT and MAS were not.
Conclusion
PKAFO may improve gait function in hemiplegic patients. It can be a useful orthosis for gait training in hemiplegic patients.
INTRODUCTION
Gait disturbance due to hemiplegia is one of many disabilities caused by stroke and traumatic brain injury [1,2], which limits the independent activities of daily living. One of the most important aims of subsequent rehabilitation is to restore the gait ability [3,4].
A common feature of hemiplegic gait is a limited ankle dorsiflexion in the swing phase due to the foot-drop and spasticity of the ankle joint, which leads to the reduction of the push-off time for the pre-swing phase [5,6]. Hemiplegic patients attempt to avoid toe dragging due to foot-drop during the swing phase, with excessive hip flexion, circumduction, and other abnormal gait patterns [7,8,9,10]. To improve abnormal gait and achieve gait efficiency, ankle-foot orthoses are often prescribed in the clinical environment to control the ankle joint during gait by reducing foot-drop and increasing walking speed and stride length [11,12,13,14].
Various walking aids and orthoses have been developed to improve the gait in hemiplegia, and their effects investigated. The use of a plastic brace in hemiplegic patients reportedly improves walking speed, step length, bow ensuring, step width, and cadence to establish a safe gait [11]. The metal brace provides more resistance to plantar flexion than the plastic brace, the metal brace can more effectively reduce foot-drop and increase the stability of the ankle joint [15].
However, the commonly prescribed hard plastic or metal ankle braces insufficiently provide the role of ankle joint in the gait cycle, lower sensory feedback for integrating motor control, limit the natural scope and flexibility, and can only be worn inside a shoe that is necessarily larger than that of the other side. The shoe is uncomfortable to wear.
An adjustable hydraulic oil damper that uses a hinge generates resistance momentum in the contralateral ankle plantar flexion in the initial swing phase, while also affecting the hip and knee joints, contributing to gait performance [16]. Also, powered devices for gait have been developed recently. Tibialis anterior pneumatic electromyography can activate artificial muscles and assist dorsiflexion in subjects without neurological deficits, thus reducing plantar flexion and preventing foot slap and drag during the swing phase [17]. Many studies used either an electromyography or a footswitch controller to operate the artificial muscle affecting the joint torque, which is reportedly effective for walking [18,19].
However, most previous studies for the powered device for gait have only been tested on healthy subjects or a few patients. There is no clinical study for hemiplegic patients.
In this study, we developed a knee-ankle-foot orthosis powered by artificial pneumatic muscles (PKAFO) for the prevention of the foot-drop and stability of lower limb during gait, and applied to hemiplegic patients to know its effectiveness and feasibility.
MATERIALS AND METHODS
Subjects
Adult subjects ≥18 years of age who had brain lesion from stroke or traumatic brain injury, as confirmed by magnetic resonance imaging, with the onset diagnosed at least 2 weeks after the acute period, were included in the study. Prior to the clinical trial, interviews, medical record review, and neurological cognitive assessments were conducted to check that inclusion and exclusion criteria. The selected subjects scored not fewer than poor grade on manual muscle tests (MMT) of the hip and knee joints, and spasticity on the hemiplegic ankle joint showed levels <3 on the Modified Ashworth Scale (MAS).
Subjects were excluded if they were unstable medically or had abnormalities in visual and vestibular functions, if gait training was impossible owing to emotional instability, and if they had severe peripheral polyneuropathy or history of musculoskeletal fracture with difficulty in walking.
The 23 participants included 17 men and 6 women, with a mean age of 59.6±13.7 years. The disease distribution included infarction (n=11), cerebral hemorrhage (n=5), traumatic brain injury (n=7), right hemiplegia (n=12), and left hemiplegia (n=11). The Mini-Mental States Examination (MMSE) score was 25.8±4.6 points (Table 1). The Presbyterian Medical Center Institutional Review Board approved the protocol.

Clinical characteristics of the subjects (n=23)
PKAFO
The novel PKAFO induced ankle dorsiflexion using pneumatic actuators. The device comprises a knee joint brace, a pneumatic actuator for ankle dorsiflexion, and a sole with forefoot and heel pressure sensors fixed with foot by the forefoot and ankle band. It was designed to be used while wearing shoes (Fig. 1). Film-type forefoot and heel sensors with a diameter of 4 mm in the sole of brace were designed to detect a pressure of 1 kg/cm2. Detection initiated signal generation in the lateral malleolus area and signal transmission to the receiver to activate an actuator in the brace through the line pressure controller and an air tube. The actuator was designed to operate at an air pressure of 5.5 bars, with an air injection time of 0.2 seconds and an emission time of 0.5 seconds. The same pressure was used irrespective of the subject used. When the heel contacted the ground, the heel sensor would be activated in the early stance phase with the actuator supporting eccentric plantar flexion, allowing the foot to softly touch the ground in the gait. Lifting of the heel at the end of the stance phase activated the heel sensor to start the work for dorsiflexion. The forefoot sensor was designed to provide powerful dorsiflexion, which prevented foot drag at the early swing phase and aided in the preparation for heel contact with the ground by weakening ankle dorsiflexion at the end of the swing phase. During clinical training, the PKAFO was fixed on the hemiplegic lower leg and foot with Velcro to eliminate pain and discomfort. The knee brace was composed of duralumin and had a dial lock on the knee, which helped prevent hyperextension (Fig. 2).
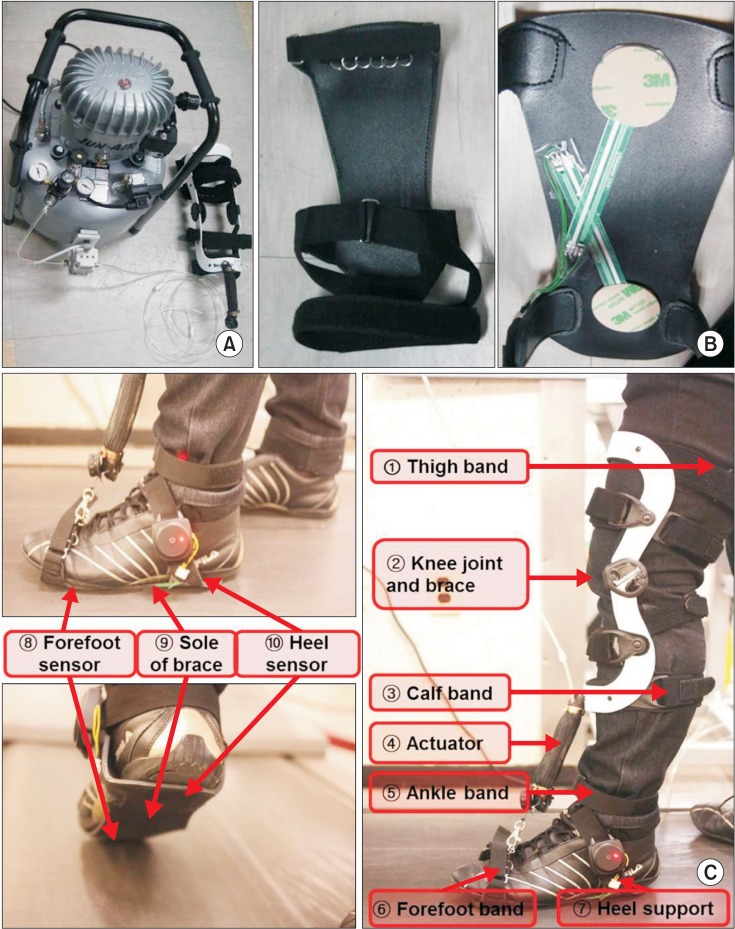
Components of powered knee-ankle-foot orthosis. The actuator (A) was activated by pushing sensor on forefoot and heel (B) of a powered knee-ankle-foot orthosis (C).

Gait training with pneumatic powered knee-ankle-foot orthosis on treadmill: (A) the anterior view and (B) the lateral view.
Intervention and outcome measurements
Subjects wore their own shoes. To ensure PKAFO effectiveness, evaluations were performed before and after gait training. Two trials were done each time. The patients received 3 weeks of training on a Gait Trainer treadmill (Biodex Medical Systems, Shirley, NY, USA). The training was conducted by two physical therapists 30 minutes per day, 5 days per week. Gait parameters included a 10-m walking test (10MWT), walking speed (m/s), step cycle (cycle/s), and step length (m). Walking speed, step cycle, and step length were measured automatically when the most comfortable walking speed has been attained. The parameters were measured with and without the PKAFO, before and after gait training. Clinical parameters-Korean version of Modified Barthel Index (K-MBI), MMT on the hemiplegic side of hip flexion, knee flexion and extension, ankle dorsiflexion and plantar flexion, and the MAS of hemiplegic ankle-were measured before and after gait training.
Statistical analysis
Wilcoxon signed-rank test was used to analyze the results of gait training with the PKAFO and the immediate effectiveness of gait with the PKAFO. SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA) was used. A p-value less than 0.05 was considered statistically significant.
RESULTS
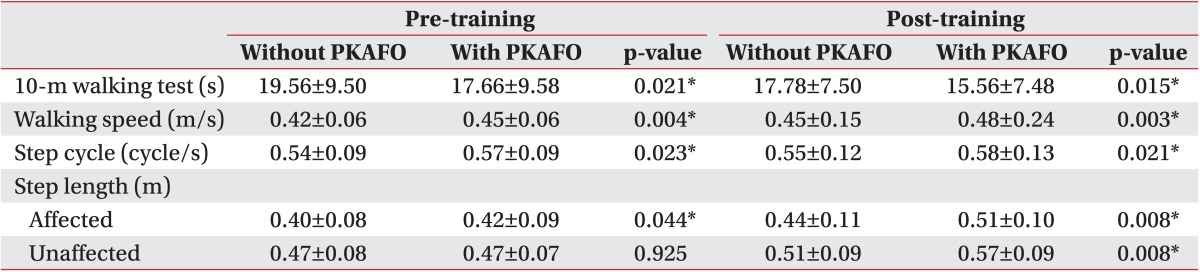
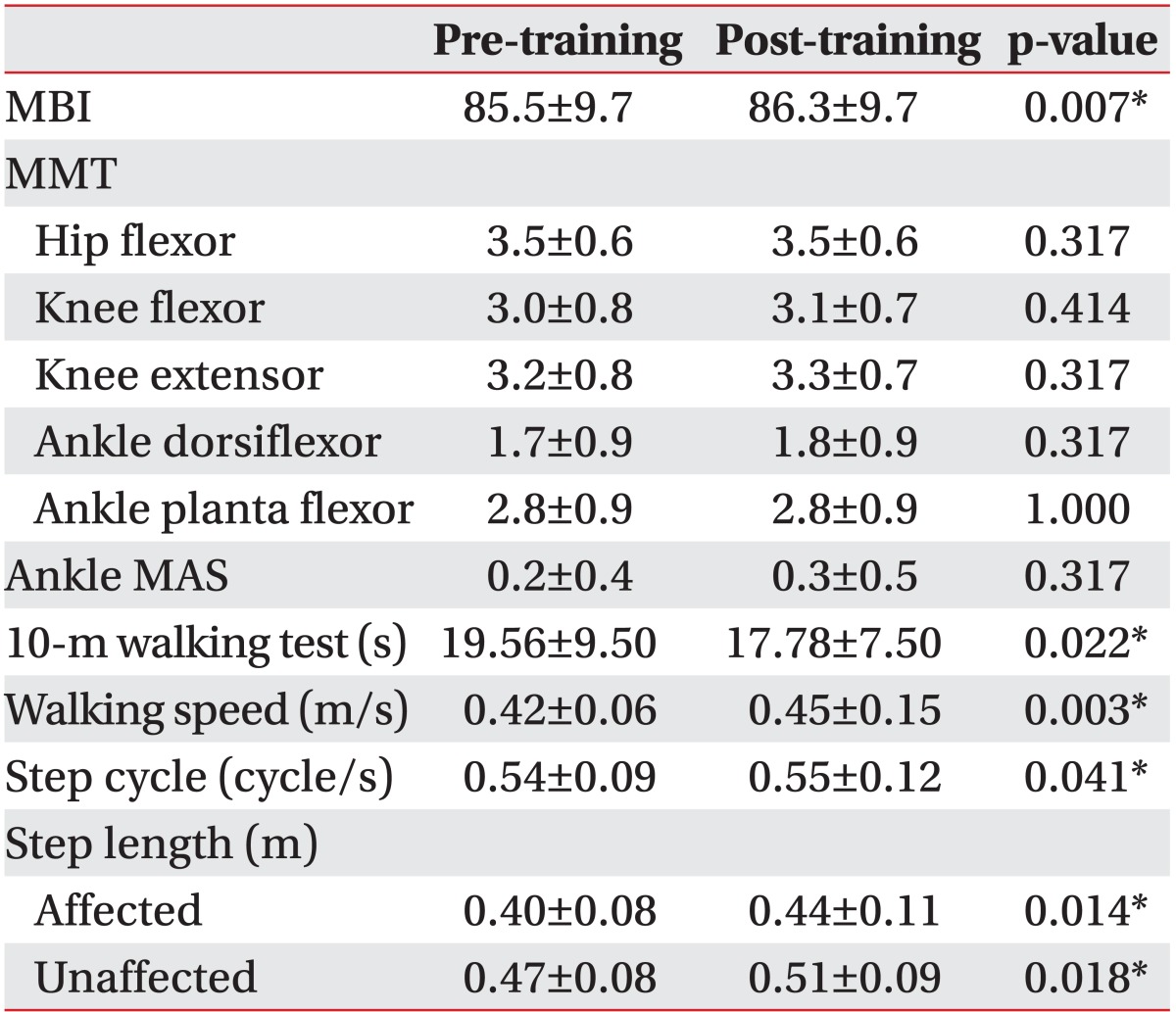
The use of the PKAFO significantly improved performances of 10MWT, walking speed, and step cycle before and after gait training (all p<0.05) (Table 2). Step length with the PKAFO in the affected side significantly increased, but there was no change in the other side before gait training. However, step length was significantly improved on both sides after 3 weeks of gait training (p<0.05) (Table 2). Before and after gait training, the clinical parameter of K-MBI score improved (p=0.007), while no significant differences (all p>0.05) were evident after gait training in hip flexion MMT, knee flexion MMT, knee extension MMT, ankle dorsiflexion MMT, ankle plantar flexion MMT, and MAS score in the ankle. 10MWT, walking speed, gait cycle, and step length significantly improved after 3-week gait training with the PKAFO (all p<0.05) (Table 3).
Gait parameters measured in walking conditions
Parameters compared before and after the training
DISCUSSION
An efficient gait is a key goal in stroke rehabilitation. Many of hemiplegic patients can regain their ability to walk after rehabilitation, but show high energy expenditure, aberrant kinematic and kinetic data, and atypical muscle activity during gait [5].
Motor function and stability change of hemiplegic patients gait after stroke include weakened strength, balance disorder, foot drop, and joint instability, which result in a decrease in walking speed and cadence, short step length and compensation gait posture [20]. These changes severely diminish the quality of life of hemiplegic patients.
Patients with hemiplegia experience difficulties with voluntary muscular control in the gait due to the spasticity and impaired muscle strength of the lower limb in the hemiplegic side, which considerably reduce walking speed. Thus, walking speed can serve as a practical marker for determining the degree of improvement in the level of post-stroke walking ability and is closely associated with the recovery of muscle strength [21]. A post-stroke hemiplegic patient wearing an AFO reportedly demonstrated increased walking speed in the 6-minute walk test [13]. The present study verified that the application of the novel, non-plastic and non-metal PKAFO using a pneumatic actuator, immediately produced increased treadmill walking speed. The gait training with PKAFO may be attributed to the increased stability induced by the active ankle dorsiflexion, knee support by the orthosis and the activation of ankle kinematics on the paretic side. This is also consistent with the results of the other studies of AFO in hemiplegic patients [11,15]. Differences in speed between the treadmill-determined 10MWT and velocity likely reflected gait improvement.
Presently, all gait parameters were improved by applying the PKAFO, but no significant change was observed in the step length of the non-hemiplegic side with the PKAFO before gait training, which may be attributable to the insufficient pre-intervention period of PKAFO acclimation. However, gait training with the PKAFO significantly increased the step length of the paretic and non-paretic sides after the 3-week intervention.
Hemiplegic patients often demonstrate common gait problems that include inadequate dorsiflexion of ankle causing foot-drop due to weakness of the muscles responsible for dorsiflexion and plantar flexor spasticity or stiffness, which causes decreased push off and foot-drop [5]. Rehabilitation of patients with hemiplegia has explored various treatment methods to manage the foot-drop, reflecting the importance of the ankle dorsiflexion in gait. Ankle dorsiflexor strength is independently associated with the walking endurance of stroke survivors with spastic ankle plantar flexors [22]. The two most frequently used methods to manage foot-drop are the AFO and functional electrical stimulation (FES) on the peroneal nerve or muscles for ankle dorsiflexion [8,23,24]. A study of 197 patients, for whom it had been 3 months after a stroke compared the AFO with the foot-drop stimulator to treat foot-drop. The authors concluded that both approaches resulted in a significant improvement in gait speed and functional outcomes [25].
The traditional treatment for foot-drop is an AFO that holds the foot in a neutral position. The most common type of AFO is a solid plastic brace, although it may be made of metal or composite materials, with any number of modifications including an articulated or hinged ankle joint. In general, AFOs support ankle dorsiflexion during the swing phase and improve knee stability in the early stance phase in individuals with foot-drop [1,26]. In recent years, power transmission devices like a powered AFO have been developed to control foot-drop in hemiplegic gait [18,27,28].
FES has been used to treat chronic hemiplegia since the 1960s. Electrical stimulation for the treatment of foot-drop in hemiplegic patients was first performed by Liberson et al. [23], and a single-channel functional electrical stimulator to manage foot-drop with electrodes attached to the skin surface has been reported [24]. Another study utilized 2-channel FES electrodes in the peroneal nerve of patients with foot-drop after stroke, which led to improvement of walking speed [8]. FES for foot-drop in stroke reportedly aided patients in walking and also served as a safe treatment option for ankle dorsiflexion [29].
However, there are several significant disadvantages in the two most frequently used methods to manage foot-drop. Limitations of AFOs include limited ankle mobility that may contribute to the development of contracture [26] and difficulty with standing-up from a sitting position, along with discomfort and unfavorable aesthetics. Furthermore, an AFO can induce an unnatural gait pattern and can lead to compensatory patterns at the knee and hip in the hemiplegic side [30,31]. FES disadvantages include difficulty in exact positioning of the electrode and movement of the electrode while walking, which can cause discomfort and muscle fatigue [24].
Presently, a pneumatic power transmission device was constructed to remedy these shortcomings of AFO and FES. The goal was to minimize discomfort and muscle fatigue with dorsiflexion of the hemiplegic ankle, and to induce a natural gait pattern, which would allow the ankle joint to move freely.
Walking speed and gait symmetry can improve as muscle strength recovers [32]. However, presently there was no significant difference in muscle strength, so the effectiveness of muscle strengthening for gait velocity was excluded.
During this study, no change in muscle strength and spasticity occurred, but gait function and K-MBI seemed to be improved. Because the subjects were trained by the therapist for the concurrent rehabilitation treatment of gait, the increase in gait parameters and K-MBI after gait training could not be ruled out in the effectiveness of the general rehabilitation management. Long-term studies that incorporate a control group are needed. Other limitations include the short training period and the absence of measurement from a two- or three-dimensional gait analysis. In other words, comparison between experimental and control groups, comparison with other devices, such as the AFO and FES, and an analysis of gait as the kinetic and kinematic data are needed. Evaluation of patient comfort would be useful.
In conclusion, this clinical study documents that applying the PKAFO improves gait ability in patients with hemiplegia by activating the dorsiflexion. Long-term use of the PKAFO is potentially helpful in the recovery of gait in hemiplegic patients.
ACKNOWLEDGMENTS
This study was supported by grants from the Korean Healthcare Technology R&D Project (A091220 and HI12C0118), Ministry of Health & Welfare, Korea.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.