The Effect of Power-walking in Phase 2 Cardiac Rehabilitation Program
Article information
Abstract
Objective
To evaluate the effects of power walking (PW) training on a treadmill in patients with coronary heart disease (CHD) and to compare the cardiovascular effects of PW with usual walking (UW).
Method
Patients were recruited as participants in phase 2 cardiac rehabilitation program after receiving percutaneous coronary intervention (PCI) due to acute coronary syndrome from our hospital. The participants were divided into the PW group (n=16) and UW group (n=18). All participants received graded exercise test (GXT) and significant difference in maximal oxygen consumption (VO2Max) was not observed between the groups. Aerobic exercise training on treadmill was given for 50 minutes per session, three times a week, for six weeks. Physiological and hematological parameters were tested before and 6 weeks after the cardiac rehabilitation program. Exercise duration, VO2Max, heart rate, blood pressure, and rate pressure product were evaluated through graded exercise test. Hematological measurements included serum lipid profile, and high-sensitivity C reactive protein (hs-CRP).
Results
There were no significant differences in resting heart rate, maximal heart rate, resting systolic and diastolic blood pressures, lipid profile, hs-CRP, VO2Max, and RPP between the PW group and UW group. However, after 6 weeks of the intervention, VO2Max in the PW group (36.03±5.69 ml/kg/min) was significantly higher than that in the UW group (29.73±5.63 ml/kg/min) (p<0.05).
Conclusion
After six weeks of phase 2 cardiac rehabilitation program, the PW group showed significant improvement in VO2Max than the UW group. Thus, it will beneficial to recommend power walking in cardiac rehabilitation program.
INTRODUCTION
Improvement in physical activity and exercise capacity is important in primary and secondary preventions of cardiovascular disease.1 The positive effects of walking on exercise capacity and physical health along with metabolic and psychological health2-4 for healthy people, as well as for people with various chronic disorders have been proven through research.5-9 Walking exercise and energy consumption has a U-shaped relationship, where decreased walking speed leads to increased need for energy or oxygen consumption. A normal adult walking at a speed of 4.50-4.86 km/hr has the least aerobic requirement and relatively low exercise intensity. It has been reported that running is preferred over walking at a speed equal to or greater than 8 km/hr, since running at the higher speed consumes less oxygen than walking.10,11 Moreover, the degree of stride width during walking exercise could greatly affect the aerobic demands during walking exercise, since increased speed increases the stride width and vice versa. Walking exercise at a speed around 4.67-4.81 km/hr could especially be effective in improving cardiovascular endurance, as well as weight and percent body fat reduction in middle-aged adults with sedentary lifestyles.12
Power walking is a form of exercise where active upper body movement is added to the usual walking exercise. Power walking is a fast walking exercise done at a speed of 6 to 8 km/h with the back straight and the center of gravity moving from heal, sole, and to hallux. The elbow joints are bent 90 degrees to actively swing back and forth during movement.12
The energy consumption increases up to 55% in walking exercise with the arm movement in comparison to just walking exercise without arm movement. Power walking has advantages of greater energy consumption than with running at a speed equal to or greater than 8 km/hr. Moreover, power walking consumes comparatively greater energy during exercise, while being at a lower intensity. Despite the advantages of power walking, the exercise effects have not been reported in cardiac rehabilitation programs.13
Therefore, the effects of power walking on cardiac rehabilitation have been evaluated in this study by dividing the cardiac rehabilitation patients into the power walking group and regular walking group for their exercise capacities.
MATERIALS AND METHODS
Subjects
The subjects were patients who had been diagnosed with acute coronary syndrome and had undergone percutaneous coronary intervention (PCI). The patients were enrolled at our rehabilitation clinic for graded exercise test and 6 weeks of aerobic exercise program under clinical surveillance; this was a phase 2 of a cardiac rehabilitation program. The patients enrolled as participants to the study after detailed explanations of the purpose and procedures of the study. Those patients with contraindications to exercise or clinical risk factors, such as musculoskeletal, neurological, pulmonary or metabolic disorder were all excluded from the study.
Graded exercise test (GXT)
Symptom-limited exercise tolerance tests were carried out using a modified Bruce protocol, which is a GXT protocol for cardiovascular disorder patients with a gradual increase in the exercise loads. The test was terminated according to the American Heart Association's (AHA) early termination criteria upon monitoring of abnormal chest pain, blood pressure, pulse, EKG, or subjective symptoms by the patients such as dizziness or light headedness.14 A real-time recording 12-channel EKG for GXT Q4500 (Quinton Instrument Co., Boston, USA), a respiratory gas analyzer Quinton metabolic cart (Quinton Instrument Co., Boston, USA), an automatic blood pressure and pulse monitor Model412, (Quinton Instrument Co., Boston, USA), and a treadmill for GXT Medtrack ST 55 (Quinton Instrument Co., Boston, USA) were used during the test. Resting heart rate, maximal heart rate, resting systolic and diastolic blood pressure, resting diastolic blood pressure, maximum exercise duration, metabolic equivalents (METs), resting and maximal heart rates, blood pressure, maximal and submaximal rate pressure product (RPP), and VO2max were recorded during graded exercise test for all patients. Borg's rate of perceived exertion with 6-20 scale was used to measure the rate of perceived exertion (RPE). Administration of all medications was requested to either discontinue or maintain existing dosage for the duration of graded exercise test and exercise program. All patients received treatment at the department of internal medicine as inpatients, followed by a visit to the cardiac rehabilitation clinic for exercise tolerance tests within a week of discharge. The patients participated in the cardiac rehabilitation program one to 2 days after graded exercise tests with the exercise intensity calculated based on the Karvonen formula15 (maximal heart rate - resting heart rate x exercise intensity (%)+resting heart rate) with the target heart rate (%) between 60% and 85% for exercise intensity. Heart rates and ECG (myocardial ischemia and arrhythmia) were monitored real-time with a wireless EKG attached to the patients during the cardiac rehabilitation exercise program. Blood pressure was measured 2 minutes prior to the termination of exercise. The exercise intensity was limited to the target heart rate of 60 to 85% based on the Karvonen formula.
Exercise procedure and measured parameters
Cardiac rehabilitation exercise was conducted 3 times a week for 6 weeks with the elbow joints flexed to 90 degrees and the arms swung back and forth during walking. The exercise intensities were set at 60% of the target heart rate during the first 2 weeks, 70% during 3rd and 4th weeks, and 85% during 5th and 6th weeks. Identical exercise protocol was prescribed to the UW group except for intermittently holding onto the handles while walking (Fig. 1). Resting heart rate (RHR), maximal heart rate (MHR), resting systolic blood pressure (RSBP), resting diastolic blood pressure (RDBP), maximal oxygen consumption (VO2max), maximal exercise duration, and metabolic equivalent (MET) were measured via graded exercise test (GXT) and lipid profile and hs-CRP were tested through hematological analysis after 6 weeks of cardiac rehabilitation program for comparison.

The power walking group (A) was instructed to swing both arms back and forth while the elbow joint was bent at 90 degrees. The usual walking group (B) was instructed to intermittently grasp on the handles for safety during walking.
Statistical analysis
The results were analyzed for means and standard deviations with SPSS/PC+ version 12.0, a statistical package for Windows. Chi-square test and Wilcox's rank-sum test were conducted to compare age, sex, BMI, diagnosis, lipid profile, and medication between the groups. Wilcoxon's rank-sum test and conducted to compare the test variables before and after exercise between the groups. Wilcoxon's signed rank test was conducted to compare the mean differences of the variables between the groups and pre and post exercise. The significance level was set at p<0.05.
RESULTS
General characteristics of the subjects
The subjects were randomly assigned into either the power walking group (PW) or usual walking group (UW) for the study. The mean ages were 55.25±10.28 and 59.00±9.4 for PW (n=16) and UW (n=18), respectively. PW was composed of 14 men and 2 women, and UW was composed of 17 men and 1 woman. There were no significant differences in body mass index (BMI), medication, past history, physical status, exercise capacity, pre-exercise lipid profile or hs-CRP, between the groups (Table 1).
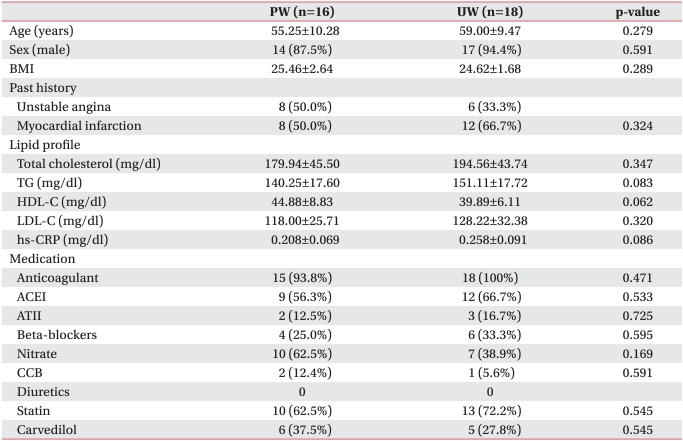
General Characteristics of the Subjects
Changes in exercise capacity
Resting heart rate (RHR), maximal heart rate (MHR), resting systolic blood pressure (RSBP), resting diastolic blood pressure (RDBP), rate pressure product (RPP), metabolic equivalent (MET), exercise duration, and VO2max were compared for test variables pre- and post-6-week intervention in both groups. Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), metabolic equivalent (MET), and exercise duration did not show significant differences between the groups. However, VO2max and metabolic equivalent (MET) were significantly higher in PW than in UW after 6 weeks of exercise (Table 2).
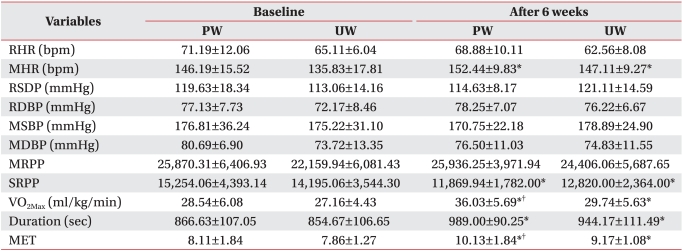
Comparison of Hemodynamics 6 Weeks after Exercise Program between PW and UW
Differences in lipid profile and hs-CRP
Changes in lipid profile and hs-CRP were measured between PW and UW before and after 6 weeks of exercise intervention. All variables of lipid profile and hs-CRP did not show significant changes before and after 6 weeks of exercise between the groups (Table 3).
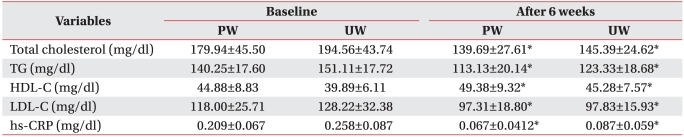
Comparison of hs-CRP and Lipid Profile 6 Weeks after Exercise Program between PW and UW
DISCUSSION
Improved exercise capacity is believed to be more closely related to the peripheral effects than to central effects of the heart in the field of cardiac rehabilitation.16 It was noted that peripheral muscles utilize oxygen obtained from aerobic exercises more effectively by increasing the number and size or aerobic related enzymes and mitochondria, as well as increase the level of myoglobin and capillary vessels to the striated muscles.17,18 Patients with coronary artery disease can avoid possible physical disability and further prevent recurrence of CAD and mortality.
Myocardial oxygen demands during active daily activities can be diminished through aerobic exercise by increasing maximum oxygen consumption, and decreasing maximal heart rate and rate pressure product.17 The rate of oxygen consumption is determined by the difference between cardiac output and arteriovenous oxygen difference. Cardiac output is decided by stroke volume and heart rate which in turn increase the maximum oxygen consumption.19 Although the differences were not observed in systolic blood pressure, diastolic blood pressure, resting heart rate, maximal and sub-maximal rate pressure product before and after 6 weeks of exercise intervention between the groups, significant difference in VO2max was observed between the groups.
The results of the EMG measurements of the upper and lower limbs by Cho et al.20 indicated that the muscular activities observed in all upper and lower limb muscles in power walking subjects were greater than that found in those subjects that walked at a slower pace. EMG activities were especially higher in biceps brachii of the upper extremity, and medial gastrocnemius, lateral gastrocnemius, and soleus of the lower extremity. Such results suggest that comparatively higher physical activity ranges and muscular activities during power walking may be related to higher maximal oxygen consumption in comparison to usual walking.
One metabolic equivalent (MET) refers to the amount of oxygen consumed during one's resting state (3.5 ml/kg/min). MET is obtained by dividing the value of VO2max, acquired during graded exercise test with a gas exchange analyzer, by 3.5 ml/kg/min. Increased 1 MET is related to decreased risk of death by coronary artery disease in healthy subjects in comparison to unhealthy subjects. Increased 1 MET in those with and without CVD risk factors showed 28-51% reduction in fatal cardiac death and 17-29% reduction in non-fatal cardiac death. Therefore, increased 1 MET is a strong risk prognosis factor in cardiac death.21 Myers et al.22 did a follow-up study with 3,679 patients with coronary artery disease for 6.2±3.7 years after measuring their VO2max with graded exercise tests. Exercise capacity of the patients with METs of ≤4.9 METs and ≤10.7 METs had mortality risks of 4.1 and 1.0, respectively. Dorn et al.23 reported that the mortality rates of the acute myocardial infarction patients decreased approximately 10% for every 1 MET increased through the patient progression observations. A significant increase in VO2max alone could have adequate significance, despite the insignificant changes in other variables between PW and UW, based on such previous results. Aerobic exercise plays an important role in cardiovascular disease prevention and offers therapeutic effects by decreasing total cholesterol, triglycerides and increasing high-density lipoprotein-cholesterol.24 Moreover, it has been proven that hs-CRP, a major risk factor marker for mortality in acute myocardial infarction patients, can be decreased through aerobic exercise. Fallon et al.25 reported that regularly played soccer decreased hs-CRP concentration. Mattusch et al.26 reported that 9 months of endurance running decreased hs-CRP concentration by 31%. Smith et al.27 reported that high risk patients (n=43) with ischemic cardiovascular disease had 35% reduction in TNF-α and hs-CRP after 6 months of exercise. In this study, hs-CRP and lipid profile significantly decreased post-exercise in both groups without significant changes in between groups.
Myocardial oxygen consumption during exercise indicates the rate pressure product (RPP) during equal workloads. It plays a vital role in decreasing the incidence of angina due to its close relationship to angina threshold. Additional previously studies have reported that an increased myocardial ischemic threshold by physical activity for anti-ischemic effects further increased the ability to perform at greater work intensities.28 Ahn et al.29 reported that the rate pressure product was significantly lowered in myocardial ischemia patients that exercised in comparison to myocardial ischemia patients that did not exercise, with a significant decrease in maximal pressure rate product at equal workloads. Such significant improvement can be credited to regular aerobic exercise by improving exercise tolerance and exercise duration, as well as increasing heart rates and systolic blood pressure.
There are some limitations to this study, which should be considered in future studies. The limitations include an inadequate number of patients and 6 weeks of short-term exercise intervention for adequate observation of the significant changes in variables. Further studies should be conducted with an adequate number of patients with long-term observation of their progress.
CONCLUSION
The significantly increased maximum oxygen consumption (VO2max) of the power walking group with acute coronary syndrome in comparison to the usual walking group with coronary syndrome suggests the possibility that power walking should be part of the recommendation for a more aggressive mode of cardiac rehabilitation exercise.