Ureteral Rupture Caused by a Suprapubic Catheter in a Male Patient With Spinal Cord Injury: A Case Report
Article information

Abstract
Spinal cord injury (SCI) may lead to urinary system disturbances. Patients with SCI usually have neurogenic bladder, and treatment optionss for this condition include clean intermittent catheterization and a permanent indwelling urethral or suprapubic catheter. Complications of catheterization include urinary tract infection, calculi, urinary tract injury, bladder contraction, bladder spasm, renal dysfunction, bladder cancer, and so forth. To the best of our knowledge, ureteral rupture is an unusual complication of catheterization, and ureteral rupture has been rarely reported in SCI patients. Therefore, here we report a case of ureteral rupture caused by a suprapubic catheter used for the treatment of neurogenic bladder with vesicoureteral reflux in a male patient with SCI. Due to SCI with neurogenic bladder, ureteral size can be reduced and the suprapubic catheter tip can easily migrate to the distal ureteral orifice. Thus, careful attention is required when a catheter is inserted into the bladder in patients with SCI.
INTRODUCTION
Spinal cord injury (SCI) may cause interruption of the urinary system. In particular, it commonly leads to bladder dysfunction, often referred to as neurogenic bladder [1]. Non-invasive treatment options for bladder dysfunction include bladder expression, bladder reflex triggering, and drug treatment, while minimally invasive treatment options such as clean intermittent catheterization or the use of a permanent indwelling urethral or suprapubic catheter can also be used [12]. Suprapubic catheter placement is frequently used in patients with SCI. However, the long-term use of an indwelling urethral or suprapubic catheter may cause complications including urinary tract infection, calculi, urethral damage, renal dysfunction, and bladder cancer [13].
Catheter localization in the ureter is a rare complication; in fact, only 17 cases of an indwelling urethral or suprapubic catheter located in the ureter have been reported to date, among which three cases showed ureteral rupture after catheterization [456].
Here we report a rare case of distal ureteral rupture caused by a suprapubic catheter in a male patient with SCI.
CASE REPORT
A 63-year-old man was admitted to Gyeongsang National University Hospital in March 2003 after a motorcycle accident. Magnetic resonance imaging performed on the day of injury revealed a C6-C7 vertebral body fracture and spinal cord contusion. According to the International Standards for Neurological Classification of Spinal Cord Injury, the patient had a complete lesion (American Spinal Injury Association impairment scale A) with a C7 neurologic injury level. An indwelling urethral catheter had been inserted in our patient for the treatment of neurogenic bladder induced at the time of the trauma. Two years and four months after the SCI, left-sided grade II vesicoureteral reflux (VUR) was identified. One month later, the patient was hospitalized for right-sided acute pyelonephritis and a urinary tract infection. A suprapubic catheter was inserted after cystostomy during his hospital stay. Thereafter, the suprapubic catheter (16-Fr) was changed monthly at the Outpatient Clinic of the Rehabilitation Medicine.
Five years after the SCI, voiding cystourethrography revealed bilateral grade II VUR, and it was decided that the patient's condition would be monitored during regular follow-up appointments.
Eleven years after the SCI, the patient underwent a regular suprapubic catheter change at the outpatient clinic in the morning, and he developed hematuria, fever, chills, and dysuria in the afternoon; hence, he was transferred to the Emergency Department. Upon arrival at the Emergency Department, his body temperature was 39℃, and laboratory evaluation showed a white blood cell (WBC) count of 17,460 mm3 and C-reactive protein level of 117.6 mg/L. Urinalysis revealed a WBC count >100 per high-power field. The patient was suspected to be suffering from acute pyelonephritis, and hence, abdominal computed tomography (CT) was performed. The CT scan revealed the presence of retroperitoneal free air and hematoma due to right distal ureteral rupture as well as hydronephrosis of the right kidney (Figs. 1, 2). A kidney, ureter, and bladder radiograph showed radiocontrast extravasation from the ruptured ureter (Fig. 3). The suprapubic catheter was the suspected cause of the injury; thus, it was removed. Subsequently, percutaneous nephrostomy (PCN) was conducted, followed by catheter insertion. Urinary drainage was normal and antibiotics were administered to treat acute pyelonephritis. Nine days after admission, a double J (D-J) stent was inserted, and the PCN catheter was removed on the next day. The patient was discharged with the D-J stent in place.
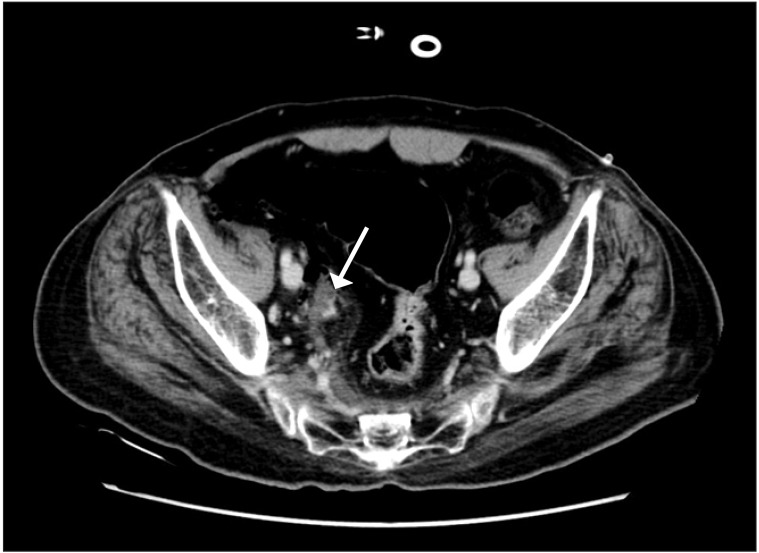
Contrast computed tomography (axial section) showing retroperitoneal free air and a hematoma (arrow).

Contrast computed tomography (coronal section) showing retroperitoneal free air and hematoma due to right distal ureteral rupture (arrow).

A radiograph of the kidney, ureter, and bladder showing extravasation of the radiocontrast from the ruptured ureter (arrow).
DISCUSSION
A total of 17 cases of inadvertent placement of an indwelling urethral or suprapubic catheter within the ureter have been reported to date (Table 1). Among them, 12 patients were female and 5 patients were male. This discrepancy may be due to the sex-specific difference in urethral structure. The female urethra is 2.5–4 cm long, short, thick, and close to the anus, whereas the male urethra is 20–25 cm long, thinner, and more curved. Therefore, urethral or suprapubic catheter insertion in female patients would more frequently result in incorrect positioning within the ureter than that in male patients [7]. Eleven of the 17 cases included patients with diseases such as stroke, malignant gynecological tumor, chronic renal failure, and ossification of the posterior longitudinal ligament accompanying neurogenic voiding dysfunction [478]. There were 6 patients with neurogenic bladder caused by SCI, but all patients had indwelling urethral catheters.
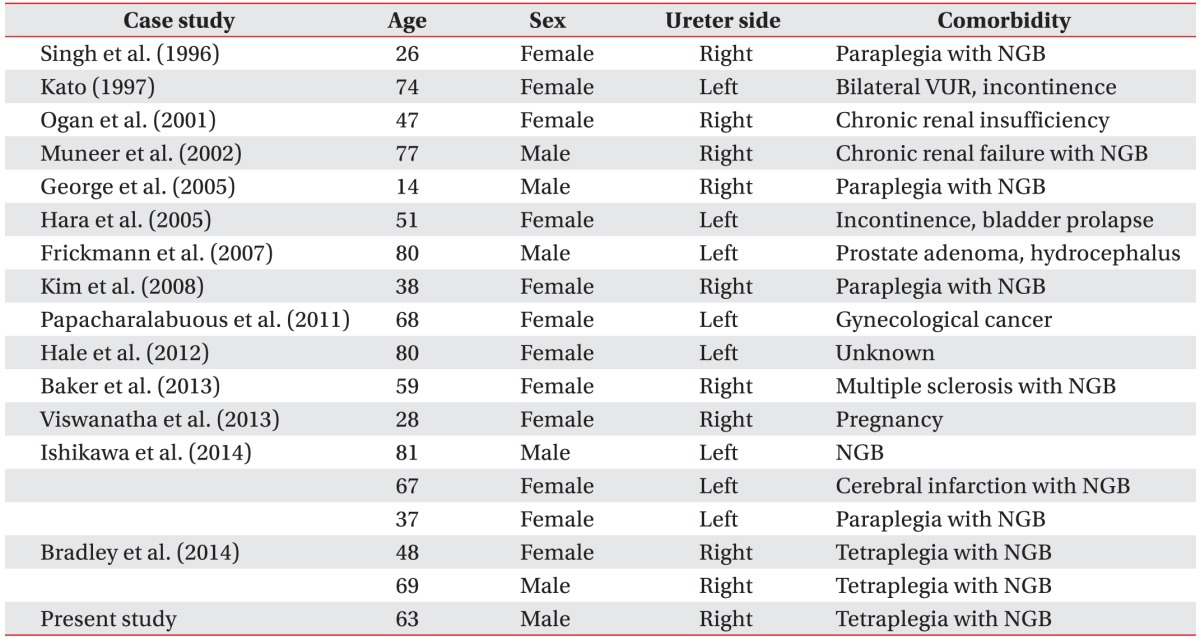
Patient characteristics in the reported cases of inadvertent placement of an indwelling urethral or suprapubic catheter within the ureter
Ureteral rupture is a rare disease entity that can result from penetrating injuries and blunt trauma or iatrogenic events that occur during urological, gynecological, or general surgery or after the insertion of an indwelling urethral or suprapubic catheter [478]. Rupture may also by induced by non-traumatic factors such as a change in urinary tract pressure due to the existence of a urinary stone or an abdominal or pelvic tumor. In three of the 17 cases, ureteral rupture was caused by catheterization. Frickmann et al. [4] reported one case of ureteral rupture during a suprapubic vesical catheter change in a patient with prostate adenoma. The other two cases of ureteral rupture after urethral Foley catheterization were reported in female patients [56]. The case reported here is the first case of ureteral rupture induced by an indwelling suprapubic catheter in a male patient with neurogenic bladder caused by SCI.
Permanent indwelling urethral or suprapubic catheters used to treat neurogenic bladder, a complication in SCI patients, can cause bladder fibrosis, which leads to a reduced bladder volume and VUR [9]. In the current case, it is also possible that the inserted catheter entered the ureter more easily since the bladder volume was reduced due to prolonged suprapubic catheterization, and thus, the distance between the suprapubic opening and the ureter was shortened. Moreover, the patient had a grade II VUR for several years, which probably affected the distal ureter diameter and facilitated entry of the suprapubic catheter into the ureter.
Changing a permanent indwelling urethral or suprapubic catheter is a simple procedure that is commonly performed in hospitals, but it carries the risk of complications in SCI patients, as seen in the current case. Therefore, during catheter insertion, basic principles must be followed such as the selecting a suitable catheter size, considering the ureteral length in males and females, considering bladder size, and checking balloon inflation after insertion as well as urine drainage. When patients with a VUR undergo a catheter change, the use of simple abdominal radiographs or ultrasonography is recommended to identify urinary tract trauma such as bladder rupture and ureteral rupture.
Here, we have reported our observation of rare misdirection of a suprapubic catheter into the distal ureter followed by ureteral rupture after a catheter change as well as the literature review. This is the first case of ureteral rupture caused by a suprapubic indwelling catheter in an adult male patient with SCI.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.