INTRODUCTION
Dural arteriovenous fistula (DAVF) is caused by an abnormal arteriovenous shunt in the dura mater of the brain. DAVF are located within or near the wall of the dural venous sinus, and most frequently found in the cavernous sinus, transverse sinus or sigmoid sinus.1 These acquired lesions often occur after suffering dural sinus thrombosis2 and account for 10-15% of all intracranial vascular malformations. People aged 40-60 are generally more prone to suffering from them.1
Spinal DAVF accounts for about 70% of all spinal arteriovenous malformations (AVMs) and is the most frequent disease among all spinal vascular diseases.3 Middle-aged men are prone to spinal DAVF, and lesions are likely to occur around the dorsal surface of thoracolumbar spinal cord. Clinical symptoms are those of progressive myelopathy such as spastic paraplegia, sensory disturbance, bladder dysfunction, and bowel dysfunction, and it is rare that hemorrhage accompanies it.4
This study reports with literature review a very rare DAVF case where the lesion was located on the brain stem and upper cervical spinal cord.
CASE REPORT
A 53-year-old man with major complaints of a sudden onset of headache and mental deterioration came to the emergency center of the hospital. On admission, he was drowsy and his Glasgow Coma Scale (GCS) score was 14, and no focal neurologic signs were detected. He had no medical history of diabetes mellitus, hypertension, tuberculosis, and hepatitis, and as for family history, his mother had suffered from cerebral hemorrhage.
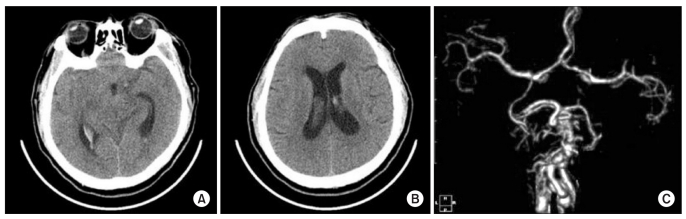
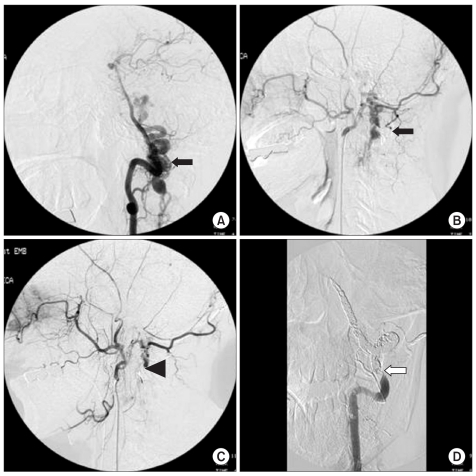
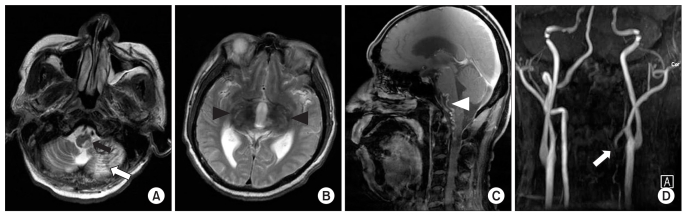
Brain computed tomography (CT) and CT angiography carried out on admission showed a subarachnoid hemorrhage (SAH), intraventricular hemorrhage (IVH) with hydrocephalus, and a tortuous vascular structure that was observed around the brain stem and upper cervical spinal cord (Fig. 1). Cerebral angiography was performed when vital signs had been stabilized and headache had been controlled through conservative treatments. The cerebral angiogram on the left vertebral artery revealed multiple vascular structures around the V4 segment of the left vertebral artery, which were drained to both sides of the sigmoid sinus and vertebral venous plexus. A cerebral angiogram on the external carotid artery showed multiple vascular structures around the occipital artery, which were connected to the drained vein observed via the left vertebral artery angiogram. Embolization was attempted on the left occipital artery and the distal V2 segment of the left vertebral artery, but the treatment was halted due to reflux. Another embolization was performed from the V4 and V3 segment to some of the distal V2 segment of the left vertebral artery. The treatment was terminated after partial occlusion was identified (Fig. 2). As mental deterioration and left hemiplegia were observed after the embolization, cerebral angiography and brain CT were conducted. However, new lesions such as cerebral hemorrhages or vascular occlusions were not found. One week after the embolization, follow-up brain CT displayed subacute cerebral infarction on the left cerebellum and thalamus, and a mild mass effect on the fourth ventricle and brain stem. The patient still felt drowsy and scored 14 on the GCS after being transferred to the department of rehabilitation medicine. Manual muscle tests of the left upper and lower limbs were measured as medical research council (MRC) grade 2 and hypoesthesia of the left face and hemibody was found. The patient also complained of dysarthria and diplopia. Spasticity, bladder dysfunction, bowel dysfunction, or dyspnea was not noticed. The patient scored 6 on the Korean-modified Barthel index (K-MBI), and the functional independence measure (FIM) score was 40. He was able to move in a wheel chair, fully dependent on a caregiver. Brain magnetic resonance image (MRI) and MR angiography performed one month after the onset showed infarctions on the left cerebellum, medial thalami, and the left posterolateral side of the upper cervical spinal cord. The occlusion of the left vertebral artery, as well as reduction in vascular structures that had been located on the brain stem and upper cervical spinal cord, were detected (Fig. 3). At that time, somatosensory evoked potential (SSEP) obtained by stimulating the right median nerve and motor evoked potential (MEP) recorded from the right abductor pollicis brevis and abductor hallucis were normal. However, SSEP of the left median nerve and MEP from the left abductor pollicis brevis were not evoked, while the latency of MEP recorded from the left abductor hallucis was delayed. The patient was put on anti-thrombotic drugs and medications for improving cognitive function, while continuing to take active assisted range of motion exercise, Bobath neurodevelopmental treatment, mat exercise, and occupational therapy. Six months after the onset, he recovered enough to bring his Korean Mini-Mental Status Examination (K-MMSE) score to 21 points, while manual muscle tests of the left upper limb were grade 3, and those of left lower limb corresponded to grade 3-4. The patient showed a significant recovery by scoring 73 on the K-MBI and 86 on the FIM. He was able to take gait training with minimum dependence on a caregiver.
DISCUSSION
About 2% of DAVF occur around the cervical spine, and in most cases they take form of myelopathy.5 It is very rare that lesions are located on the brain stem and upper cervical spinal cord, and there have been reports that such case accompany the symptoms of progressive myelopathy.6 It has been considered that spinal DAVF drained upward or inside the cranium are often related to SAH,7 and venous hypertension is thought to cause it although the exact mechanism has not been confirmed to date.8
The patient in this case had initial symptoms of SAH and IVH such as headache and mental deterioration. Through a cerebral angiography, a DAVF was diagnosed, which was fed by the left vertebral artery and occipital artery, and drained to both sides of the sigmoid sinus and vertebral artery plexus. According to the classification of Spetzler et al., this case corresponded to the intradural ventral arteriovenous fistula.9 When the causes of intracranial SAH are not found on an initial cerebral angiography, spinal DAVF fed by right vertebral artery should be considered.8 Delayed diagnosis of DAVF had a possibility to worsen its prognosis. However, the vascular malformation of our patient was located around the brain stem and upper cervical spinal cord and was large enough to be detected. In addition, recent initial cerebral angiographic protocol includes bilateral vertebral arteries, making it relatively easy to diagnose DAVF.
There have been various reports on incidence and mortality rates of DAVF in the upper cervical spinal cord. Ricolfiet al.10 reported that patients with intracranial DAVFs accompanied by venous drainage around the medulla oblongata tend to have symptoms of paraplegia or tetraplegia, sensory disturbance, and anal sphincter dysfunction. Among five cases reported, two patients completely recovered, one showed considerable improvement, and two died.10 Aviv et al.7 described that 45% of 44 cervical DAVF patients presented with SAH, 43% of them presented with myelopathy. Other symptoms such as radiculopathy, 6th cranial nerve palsy were also reported.7 Among two cervical DAVF patients who had headache and mental deterioration without focal neurological deficits, one died of shunt-related complications before planned surgical treatment was performed, while the other made good recovery after surgical removal of cervical DAVF supplied by right vertebral artery.7 As DAVF has rarely been reported to be located on the brain stem and upper cervical spinal cord, forecasting its prognosis is very difficult.
The patient in this case was affected by left hemiplegia after undergoing the embolization, but drug treatment and rehabilitation were continued, as the hemiplegia was diagnosed early. The left vertebral artery was occluded after the embolization, reducing the size of the tortuous vascular structures. We believe that areas affected by the infarctions had little influence on motor functions, and therefore a significant functional recovery was seen six months after the onset.
We report a DAVF case with literature review, where the DAVF was located on the brain stem and upper cervical spinal cord, which has rarely been considered as a cause for SAH and IVH.