INTRODUCTION
Fractures of the scapula are relatively rare, representing 3%-5% of all shoulder injuries and 0.4%-1% of all fractures [1,2]. Acromial fractures account for only 8% of all scapular fractures [3]. Avulsion fractures of the acromion occur as a result of an acute injury without direct trauma. Patients with this type of fracture usually recover quickly with non-operative treatment [4]. For the diagnosis of fracture simple radiography is usually sufficient. However, for avulsion fracture of acromion, it is difficult to diagnose through simple radiographs because there are few cases with displacement. In cases with non-displaced fracture, ultrasonography might be helpful. Investigators have reported the advantage of ultrasonography in the diagnosis of the non-displaced fractures of the greater tuberosity of the humerus and clinically suspected scaphoid fracture [5,6].
To our knowledge, no case report has described the usefulness of ultrasonography in the diagnosis of avulsion fracture of acromion. Herein we report a case of avulsion fracture of acromion diagnosed with ultrasonography, in which simple radiography revealed small calcific deposit over acromioclavicular joint.
CASE REPORT
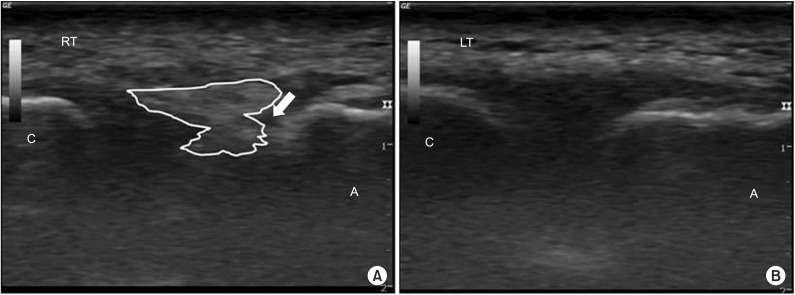
A 55-year-old man visited our outpatient clinic with shoulder pain and restricted movement. He had severe shoulder pain which occurred suddenly during the lifting of a steel reinforcement 4 days previously. He had no remarkable trauma or surgical history. It was a first time that he had shoulder pain. In physical examination, a range of motion of the right shoulder was decreased slightly with pain. He had tender points at the right acromioclavicular joint and acromion. There was a positive response in the acromioclavicular joint compression test. We requested radiographs of the shoulder for initial evaluation. There was no definite abnormality in the anterior-posterior view obtained with the both clavicles of the patient bearing weight (Fig. 1). The radiograph of shoulder in anterior-posterior view showed only small calcific deposit at right acromioclavicular joint (Fig. 2). For further evaluation, we conducted ultrasonography of the shoulder. A minimally displaced extracapsular calcifications and defect of the cortical surface at the posterior area of the acromial process was noted (Fig. 3). We could diagnose avulsion fracture with ultrasonography. There was no deltoid or rotator cuff tear. Using real-time ultrasonography, lidocaine hydrochloride 0.5 mL and 40 mg (1 mL) of triamcinolone acetonide was injected around the avulsion fracture of acromion. Anti-inflammatory medication was prescribed and the patient was advised not to do any activities that included lifting. After 4 days, the shoulder pain of patient was subjectively judged to be lessened by half. One month later, the shoulder pain was completely resolved and the patient achieved excellent shoulder function.
DISCUSSION
Avulsion fractures of acromion are thought to occur as a result of deltoid muscle forces, or as a result of strain from the acromioclavicular ligament [7,8]. In our case, the patient was found to have this type of fracture as a result of deltoid muscle forces.
In the diagnosis of non-displaced avulsion fractures, ultrasonography has advantages over simple radiographs. In a study that compared the diagnostic accuracy of simple radiography and ultrasonography for non-displaced shoulder fractures, initial detection rate for humeral fracture using simple radiology was only 45%. With ultrasonography, the detection rate increased up to 59%. Of 17 patients in whom initial radiologic examination was negative or equivocal, 10 were diagnosed as having fracture with ultrasonography [5].
Usually acromion can be observed well with simple radiographs, such as axillary lateral view and transthoracic lateral view. However, fractures of acromion rarely have displacement. Simple radiography has higher chances to miss the fracture. Although three-dimensional computed tomography could be useful as an additional examination, it is not appropriate as the screening test. It is relatively expensive and poses excessive radiation exposure. On the other hand, ultrasonography is a useful imaging modality for the diagnosis. Although ultrasonic beam cannot pass through the cortical bone, bony irregularities and defects of the cortical surface of bone could be readily detected. Usefulness of ultrasonography for the diagnosis of fractures had been also verified in an experimental study. An experimental study found that fractures may appear as interruptions of the cortical echo or as dorsal bands of echoes limited to the fracture site depending on their size [9].
However, in the acute phase of the stress fractures, there are cases in which ultrasonography did not reveal cortical defects. In the acute phase of the stress fracture, only a thin hypoechoic line by local congestion, periosteal reaction and edema of soft tissue can be found. This may be difficult to detect using ultrasonography. Additionally ultrasonography cannot disclose internal bone structure.
This case study has several limitations. Bilateral ultrasonographic images of acromioclavicular joint with oblique coronal view were not exactly symmetrical mates. Ligament of acromioclavicular joint was obstructed by extracapsular calcifications. We wanted to compare ultrasonographic images of pretreatment with those of post-treatment. However the patient did not revisit. More definite ultrasonographic images are needed to overcome these limitations.
In conclusion, we report the first case report of non-displaced avulsion fracture of the acromion that was confirmed with ultrasonography where simple radiography failed. Ultrasonography can be used in the early diagnosis of avulsion fracture. It can provide an early recovery through the proper treatment. Ultrasonography can be an excellent tool to identify a non-displaced fracture of acromion.