Subacromial Bursa Injection of Hyaluronate with Steroid in Patients with Peri-articular Shoulder Disorders
Article information
Abstract
Objective
To investigate the additive effect of sono-guided subacromial bursa injection of hyaluronate with steroid in patients with peri-articular shoulder disorders.
Method
This prospective randomized controlled trial involved 26 patients who had shoulder pain. Group A, consisting of 13 patients, was treated with a sono-guided subacromial bursa injection containing a mixture of 0.5% lidocaine (5 ml) and triamcinolone 40 mg (1 ml), followed by injection with sodium hyaluronate (2 ml) once a week for 3 weeks. The other 13 patients (Group B) were treated with a sono-guided subacromial bursa injection containing a mixture of 0.5% lidocaine (5 ml) and triamcinolone 40 mg (1 ml) once a week for 3 weeks. The effects were assessed using a visual analogue scale (VAS) of shoulder pain, active range of motion (AROM), shoulder function assessment scale (SFA), shoulder disability questionnaire (SDQ) at study entry and every week from first injection until 4 weeks after the 1st injection (= 2 weeks after 3rd injection).
Results
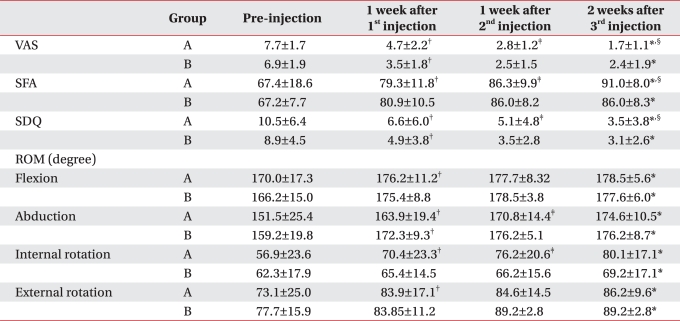
(1) Demographic features and all parameters measured before injection did not show a significant difference between the 2 groups. (2) Statistically significant improvements were shown in VAS, SFA, SDQ during the 1st, 2nd, and 4th week after the first injection in both groups (p<0.05). (3) SFA showed significant improvement at 1 week after injection only in group A (p<0.05). (4) AROM of internal rotation showed significant improvement at week 4 after the 1st injection only in group A (p<0.05).
Conclusion
Subacromial bursa injection of hyaluronate with steroid in patients with peri-articular shoulder disorders has additive effects on functional improvement of the affected shoulder, including the AROM of internal rotation.
INTRODUCTION
Subacromial bursa injection of steroid in a peri-articular shoulder disorder patient is one of the common treatment methods clinically used for pain relief and improvement of function.1-3 Recently, hyaluronate has been reported to be an effective and safe method for treating peri-articular shoulder disorder and adhesive capsulitis of shoulder.4-6 Chou et al.7 suggested hyaluronate as a substitute for steroid, because significant improvement of symptoms was shown in an initial randomized, double-blinded, placebo-controlled trial in rotator cuff disease patients without full-thickness tear where only hyaluronate was injected. Kim et al.8 suggested that subacromial bursa injection of hyaluronate is useful method as a substitute for injection of steroid in adhesive capsulitis patients who cannot be easily treated with steroid, such as diabetes patients; however, it was not more effective than steroid. Studies have been reported where subacromial bursa injection of steroid or hyaluronate was done exclusively to compare their effectiveness in peri-articular shoulder disorder patients or to investigate effectiveness by injecting both of them in adhesive capsulitis patients. However, no study has been conducted to investigate the effectiveness of subacromial bursa injection of both agents in peri-articular shoulder disorder patients.
This study was conducted to determine whether hyaluronate would have additive effectiveness in peri-articular shoulder disorder patients in which a combined formulation of steroid and hyaluronate was injected in the subacromial bursa for 3 times, and results were compared with those from injection of steroid alone.
MATERIALS AND METHODS
Subjects
Study participants were inpatients who came to rehabilitative medicine with a chief complaint of shoulder pain between April 2010 and August 2010. Subjects eligible for this study had, (1) clinically painful arc and Hawkin's sign or positive Neer's impingement sign, (2) had a partial tear or full thickness tear of a rotator cuff, or subacromial bursitis among peri-articular soft tissue disorders of the shoulder in a sonogram. Criteria for exclusion were: (1) Adhesive capsulitis of the shoulder (diagnosed when the x-ray view was normal, and active and passive elevation of the arm was <100 degree, and passive external rotation of the glenohumeral joint measured with the elbow bent 90 degree with an examiner holding the subject's wrist was 50% reduced compared to the tendon side),9 (2) History of previous shoulder surgery, (3) History of steroid or hyaluronate injection in the shoulder for the same cause, (4) Hemiplegic shoulder pain syndrome, (5) Fracture was suspected in simple x-ray image. Patients who met the criteria were chosen and categorized as group A or group B. Physical examinations, shoulder pain, and functional assessments were conducted, followed by sono-guided subacromial bursa injection.
Procedure and intervention
Confirmation of lesion was done using a sonogram after physical examination and assessment of shoulder pain and function., Patients were asked to rotate their arm internally, extend excessively, and attach their lower arm to the back of himself/herself in a sitting posture. Then, the injection site was sterilized and a sono-guided subacromial bursa injection was done. Injections were done in every patient in both groups at an interval of 1 injection per week for 3 weeks. Group A patients were treated with a mixture of 40 mg triamcinolone acetonide (Dong Kwang Parm., Seoul, Korea) (1 ml), 0.5% lidocaine (5 ml), and hyaluronate Hyruan Plus® ( LG Chemical, Seoul, Korea) at the same site. Group B patients were treated with a mixture of 40 mg triamcinolone acetonide (1 ml) and 0.5% lidocaine (5 ml) (Fig. 1). Administration of any pain reliever or anti-inflammatory drug was ceased starting 1 week prior to injection, and patients were instructed to exercise for stabilization and stretch the shoulder muscle after injection, Also, continuous education concerning exercise was recommended during weekly followup appointments. Additional physical therapy or drug treatment was not used.
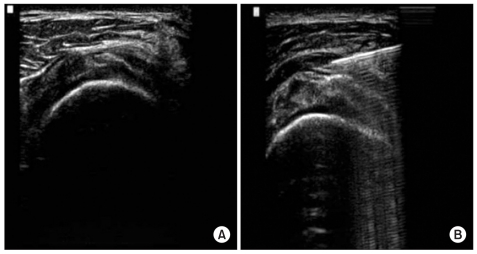
Figure shows ultrasound guided subacromial/subdeltoid bursa injection. The needle tip is positioned at subacromial/subdeltoid bursa (A). Subacromial/subdeltoid bursa is dilatated due to the injection materials (B).
Assessment of effectiveness of injection
Patient assessments were conducted prior to the first injection, 1 week after the first injection (before 2nd injection), 1 week after 2nd injection (before 3rd injection), and 2 weeks after the final 3rd injection. Assessments were carried out by the same physiatrist who had been in charge of assessment before injection. First, VAS was measured (scale of 0 to 10) by assessing the mean value for pain during the previous 24 hours. Second, active movement range of the shoulder joint was measured, and in doing so, movement of the scapula was included. Flexion and abduction of the shoulder joint were measured with the main joint being stretched in a sitting posture and upper limb movement range was measured in sagittal and coronal surfaces, respectively. External and internal rotation were defined as their movement range with the shoulder joint being supinated 90 degree in a sitting posture.
Lastly, a shoulder function assessment scale (SFA) and shoulder disability questionnaire (SDQ) were used to assess shoulder function of the patient. SFA is an assessment tool that is statistically reliable and is composed of 9 items for measuring degree of pain during rest and movement (minimum 0 to maximum 30), functions in daily life, range of motion of shoulder, from a minimum of 0 (shoulder function is the worst) to a maximum of 70 (shoulder function is the best) and scores can range from 0 to 100 by summation.10 The SDQ is a proven assessment tool used to measure the degree of disability that a patient feels and is composed of 22 self reported questionnaires and it ranges from a minimum score of 0 (no disability) to a maximum score of 22 (maximum disability).11
Statistical analysis
Age, sex, and site of occurrence were compared by Chi-square analysis and an independent t-test, and the Wilcoxon signed rank test was used to compare values for pre-injection, 1 week after 1st injection, 1 week after 2nd injection, and 2 weeks after the 3rd injection of both steroid plus hyaluronate injection groups and the steroid only injection group, and also to compare values of the 2 groups at each point. SPSS 12.0 was used as the statistical program and statistical significance was at p-value<0.05.
RESULTS
Characteristics of subjects
A total of 26 patients were enrolled in group A and their mean age was 55.5±12.1. The mean age of the 13 subjects in group B was 55.4±10.0. In both groups; 3 were male and 10 were female and there was no statistically significant difference (p>0.05)(Table 1). There also was no statistically significant difference in assessment criteria which were measured before injection (p>0.05) (Table 1). There was no significant difference in sonographic diagnosis that was done prior to injection in both groups (Table 2).
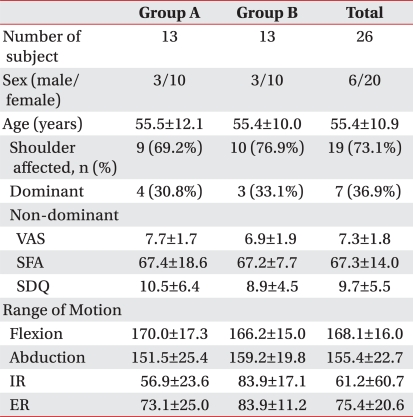
General Characteristics of Subjects
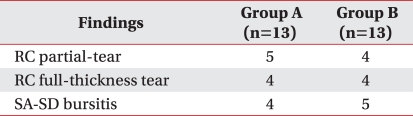
Ultrasonographic Diagnosis before Injection
Change of visual analogue scale (VAS)
There was significant improvement of VAS at 1 week after the 1st injection in both groups compared with pre-injection (p<0.05). Although there was a statistically significant improvement in group A at 1 week after the 2nd injection compared to 1 week after the 1st injection (p<0.05), it was not statistically significant in group B (p>0.05). There also was a significant improvement at 2 weeks after the 3rd injection compared to 1 week after the 2nd injection in group A (p<0.05) (Table 3). However, there were significant improvements in both groups when comparing results at 2 weeks after the 3rd injection to those at pre-injection (p<0.05) (Fig. 2). Although there was a greater improvement in group A when comparing degrees of improvement at 2 weeks after the 3rd injection and pre-injection in both groups, it was not statistically significant (p>0.05) (Table 4).
Summary of Treatment Effects in Group A and B
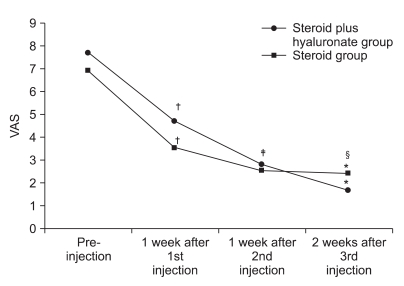
Figure shows the changes of visual analogue scale (VAS) after 3 consecutive injections. *p<0.05 pre-injection vs 2 weeks after 3rd injection. †p<0.05 pre-injection vs 1 week after 1st injection. ‡p<0.05 1 week after 1st injection vs 1 week after 2nd injection. §p<0.05 1 week after 2nd injection vs 2 weeks after 3rd injection.
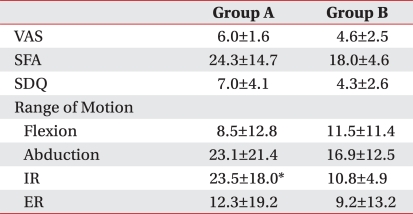
Degree of Changes in Measurement Values of Group A and B
Change of SFA
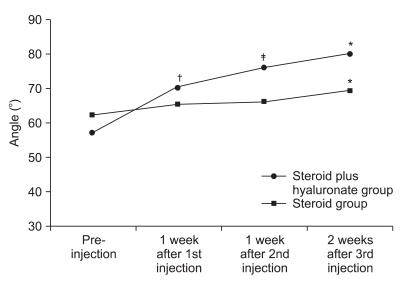
For SFA, there was a statistically significant improvement only in group A when comparing results at 1 week after the 1st injection to results at pre-injection (p<0.05), but there was no significant difference (p>0.05) in group B.
There was a statistically significant improvement in group A only when comparing results at 1 week after the 2nd injection and 2 weeks after the 3rd injection to prior results (p<0.05), but there were significant improvements in both groups when comparing results at 2 weeks after the 3rd injection to those at pre-injection (p<0.05) (Table 3, Fig. 3).
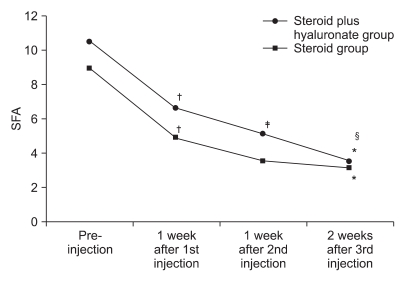
Figure shows the changes of shoulder function assessment scale (SFA) after 3 consecutive injections. *p<0.05 pre-injection vs 2 weeks after 3rd injection. †p<0.05 preinjection vs 1 week after 1st injection. ‡p<0.05 1 week after 1st injection vs 1 week after 2nd injection. §p<0.05 1 week after 2nd injection vs 2 week after 3rd injection.
There was a greater improvement in group A when comparing degree of improvement at 2 weeks after the 3rd injection and pre-injection; however, it was not a statistically significant (p>0.05) (Table 4).
Change of SDQ
There were significant improvements of SDQ at 1 week after the 1st injection compared to pre-injection in both groups (p<0.05). There was a statistically significant improvement in group A only when comparing results at 1 week after the 2nd injection and 2 weeks after the 3rd injection to prior results (p<0.05) (Table 3). However, there were significant improvements in both groups when comparing the results at 2 weeks after the 3rd injection to those of pre-injection (p<0.05) (Fig. 4).
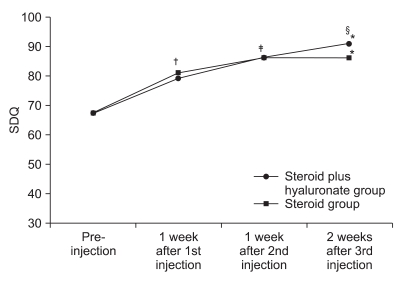
Figure shows the changes of shoulder disability questionnaire (SDQ) after 3 consecutive injections. *p<0.05 pre-injection vs 2 weeks after 3rd injection. †p<0.05 pre-injection vs 1 week after 1st injection. ‡p<0.05 1 week after 1st injection vs 1 week after 2nd injection. §p<0.05 1 week after 2nd injection vs 2 weeks after 3rd injection.
There was a greater improvement in group A when comparing the 2 groups' degree of improvement at 2 weeks after the 3rd injection and pre-injection, but the difference was not a statistically significant (p>0.05) (Table 4).
Change of active range of motion
Although there was statistically significant improvement for active range of motion of abduction at 1week after 1st injection in both groups compared to pre-injection, there were significant improvement for active range of motion of flexion, internal and external rotation at 1 week after 1st injection in group A only compared to pre-injection (p<0.05) (Table 3). There were statistically significant improvements for active range of motion of flexion, abduction, internal and external rotation at 2 weeks after the 3rd injection in both groups compared to pre-injection (p<0.05) (Table 3, Fig. 5-8). When comparing degree of improvement in flexion of the shoulder joint, there was a greater difference in group B, but it was not statistically significant (p>0.05) (Table 4). However, in cases of abduction of the shoulder joint and internal rotation and external rotation, there was a greater improvement in group A, and it was not statistically significant for abduction and external rotation, but it was statistically significant for internal rotation (p<0.05) (Table 4, Fig. 9).
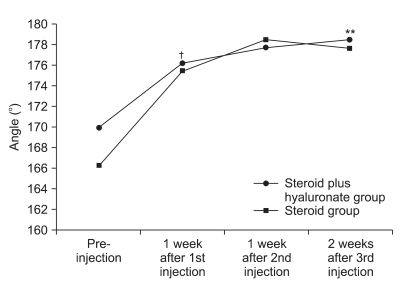
Figure shows the changes of AROM of shoulder flexion after 3 consecutive injections. *p<0.05 pre-injection vs 2 weeks after 3rd injection. †p<0.05 pre-injection vs 1 week after 1st injection. ‡p<0.05 1 week after 1st injection vs 1 week after 2nd injection. §p<0.05 1 week after 2nd injection vs 2 weeks after 3rd injection.
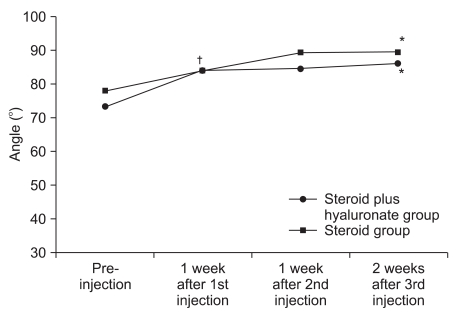
Figure shows the changes of AROM of shoulder external rotation after 3 consecutive injection. *p<0.05 pre-injection vs 2 weeks after 3rd injection. †p<0.05 pre-injection vs 1 week after 1st injection. ‡p<0.05 1 week after 1st injection vs 1 week after 2nd injection. §p<0.05 1 week after 2nd injection vs 2 weeks after 3rd injection.
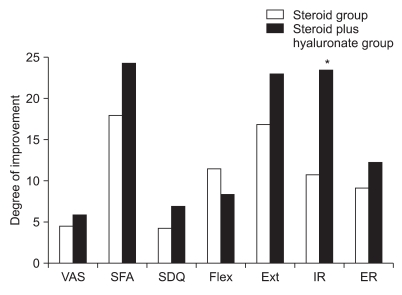
Degree of changes in measurement values (VAS, SFA, SDQ, AROM) of the 2 groups. *p<0.05 steroid vs steroid plus hyaluronate.
DISCUSSION
Subacromial bursa injection of steroid in shoulder disorders such as subacromial bursitis is often done repeatedly, but there is controversy concerning the appropriate number of injections, interval, and dose of steroid.12-15
Concerning the dose of steroid, Yoon et al.15 compared results at 1, 3, and 6 weeks after a 1st injection of triamcinolone 10 mg and 40 mg respectively, and there was no difference in effectiveness depending on dose at 1 and 3 weeks, but they reported that there was a greater significant improvement in pain, range of motion, and shoulder function of at 6 weeks after injection of 40 mg triamcinolone compared to 10 mg.
Concerning the number of repetitions, Tillander et al.13 reported that there were findings of fragmentation of collagen, necrosis, and local inflammation at 8 weeks after repeated injection, although there was no histological change of rotator cuff after 3 repeated injections of triamcinolone when they investigated histological change of rotator cuff by injecting saline and triamcinolone 8 times in total, consisting of 3 time injections at an interval of 1 week and 5 time injections at an interval of 2 weeks. Also, Bhatia et al.16 reported that subacromial bursa injection of steroid in patients with subacromial impingement syndrome was not the cause of damage to rotator cuff because there was no statistically significant difference between 2 groups of 230 patients with clinical findings of subacromial impingement syndrome who were treated with triamcinolone >3 times and patients who were treated <3 times when comparing the 2 groups by determining whether there was of rotator cuff damage using MRI.
In this study we injected 40 mg of triamcinolone with 0.5% lidocaine (5 ml) 3 times at an interval of 1 week consecutively in the subacromial bursa of 26 patients with peri-articular shoulder disorder diagnosed with clinical findings of subacromial bursitis or damage of the rotator cuff by sonogram, and simultaneously injected hyaluronate in addition to steroid in the patients who were randomly chosen.
Hyaluronate is glycosaminoglycan, a main component of synovia, and it plays important roles in lubrication of joints, and preservation of cartilage tissue. Also, bursa injection of hyaluronate in osteoarthritis of the knee and shoulder is being suggested as one of the treatment methods that can substitute for using steroids for reducing join pain, having an anti-inflammatory effect, increasing range of motion of the joint, inhibiting denaturalization of cartilage tissue, and normalizing abnormal articular fluid.7,17-21 Hyaluronate is injected at intervals of 1 week and in general, its effects are shown after 2 weeks.18,22
In this study, as set by the clinical protocol, we monitored results of the last 3rd injection for 2 weeks, which is thought to be the time required for hyaluronate to show an additive effect, but we fully reflected the additive effect because we monitored for longer than 4 weeks after the 1st injection.
There were statistically significant improvements in VAS, SFA, SDQ and full range of active range of motion of the shoulder in both groups 2 weeks after 3 consecutive injection. However, there was a greater improvement when injecting hyaluronate combined with steroid in all assessment criteria except for the flexion range. There was a statistically significant improvement especially in active internal rotation range in hyaluronate additive group, and this improvement is thought to be a meaningful result considering the fact that the symptoms were seen in internal rotation usually in peri-articular shoulder disorder.
When comparing measurement values at each time interval, group B showed statistically significant improvement only in VAS, SDQ and abduction at 1 week after 1st injection compared to pre-injection. However, Group A showed statistically significant improvement in VAS, SDQ, abduction, and SFA, which is a more functional assessment tool, and also forward flexion, internal rotation, and external rotation. These results indicate that one time injection of a combination of hyaluronate plus steroid could be an alternative of one time injection of steroid in patients who cannot be treated with repeated injections of steroid to achieve better functional improvement.
Kim et al.23 reported that there was a better treatment effect in a steroid injection group than a hyaluronate injection group in terms of speed and degree of pain relief, although their results were similar for improvement in range of motion of joint in a comparative study on effectiveness of injection of hyaluronate and steroid in patients with adhesive casulitis. The reason treatment with hyaluronate was comparatively less effective was judged to be the result of hyalurontate's initial failure rate being high in the injection group.
We ruled out using a single injection of hyaluronate when deciding the method of study because we thought initial failure rate and patients' dissatisfaction rate would be high because subacromial bursa injection of hyaluronate was less effective than injection of steroid only. We believe that studies on the effectiveness of subacromial bursa injection of steroid only and hyaluronate only as well as intra-articular shoulder injection will be necessary in the future.
Kim et al.9 reported on the effectiveness of combined therapy of hyaluronate and steroid in patients with adhesive capsulitis, but it was different from this study in subject and method of study because steroid was injected at the first week and hyaluronate only was injected in the articular capsule of the shoulder for 2 weeks at an interval of 1 week.
Also, Cho et al.6 injected a combination containing Depo-Medrol to patients in a study and reported on the effectiveness of 5 time subacromial bursa injection of hyaluronate, but it was different from this study that excluded adhesive capsulitis patients.
This study is thought to be meaningful because that we chose peri-articular shoulder disorder as the object of the study, chose subacromial bursa as an injection site (not intra-articular injection) and attempted to determine whether there was added efficacy by injecting a combination of steroid and hyaluronate.
However, the number of subjects in this study was not large, the duration of follow-up observation was short, and it is thought that additive studies including patients with a wider variety of disease are necessary. However, it is expected that the results of this study will assist in choosing medicine to be injected in bursa and deciding the number of injections in the future.
CONCLUSION
This study was conducted to determine whether there was additive effectiveness of hyaluronate when being injected with a steroid by comparing the effectiveness of treatment in a group where steroid only was injected for 3 times at an interval of 1 week with a group where hyaluronate was injected with steroid in the subacromial bursa of patients with peri-articular shoulder disorder.
There was a greater improvement at 2 weeks after the 3rd injection when a combination of steroid and hyaluronate was injected as assessed by VAS, SFA, and SDQ, but the difference was not a statistically significant. Also, SFA improved with statistical significance only in the group where hyaluronate plus steroid was injected together at 1 week after the 1st injection, and there was a statistically significant difference in active internal rotation at 2 weeks after the 3rd injection, which showed a greater improvement.
Based on the results above, it is considered that there is an additive effectiveness in improving shoulder joint movement and function, including active internal rotation when hyaluronate are used adjunctively with steroid, although there are differences depending on the number of injections.