Outcomes of Drug-Resistant Urinary Retention in Patients in the Early Stage of Stroke
Article information
Abstract
Objective
To investigate the prognosis of patients with stroke and urinary retention resistant to alpha blockers and cholinergic agents.
Methods
Post-void residual urine volume (PVR) was measured in 33 patients with stroke (14 men and 19 women) who were admitted to the department of rehabilitation medicine of our hospital within 30 days after stroke onset. An alpha-blocker and cholinergic agent were administered to patients with PVR >100 mL. If urinary retention had not improved despite the maximum drug doses, the patient was diagnosed with drug-resistant urinary retention. We retrospectively reviewed patient's charts, including PVR at discharge and prognostic factors for PVR.
Results
Ten patients (30.3%) could not void or their PVR was >400 mL at discharge (45.7±15.4 days after onset) after rehabilitation. Twelve patients (36.4%) could void, and their PVR was 100-400 mL. PVR was consistently <100 mL in 11 patients (33.3%). These measurements correlated with the Korean version of the Modified Barthel Index score, Functional Ambulation Category, and the presence of a communication disorder.
Conclusion
The results show that 22 patients (66.7%) had incomplete bladder emptying or required catheterization at discharge. Outcomes correlated with functional status, walking ability, and the presence of a communication disorder. Patients with urinary retention and poor general condition require close observation to prevent complications of urinary retention.
INTRODUCTION
Voiding dysfunction is one of the most common complications seen in patients with stroke. Approximately 65% of these patients experience voiding dysfunction during the early stage of stroke [1,2], which includes urinary frequency, urgency, incontinence, and retention. Among these symptoms, urinary retention occurs in >50% of patients with stroke who have a voiding dysfunction [2,3,4]. Urinary retention can result in several complications, including urinary tract infection, bladder calculus, and renal failure [5,6]. Therefore, appropriate management of urinary retention is important.
Urinary retention can be controlled by drugs, including alpha blockers and cholinergic agents [7,8,9]. Some studies have reported successful treatment outcomes in patients with urinary retention following stroke [4]. However, some patients do not respond to drug treatment, and an indwelling catheter or intermittent catheterization must be used. Little is known about the outcomes of patients with urinary retention who do not respond to medication. Detailed knowledge regarding the outcomes of patients with drug-resistant urinary retention would be useful for clinicians to devise appropriate management strategies for voiding dysfunction.
In this study, we investigated the outcomes of patients with drug-resistant urinary retention during the early stage of stroke at discharge after rehabilitation.
MATERIALS AND METHODS
Study subjects
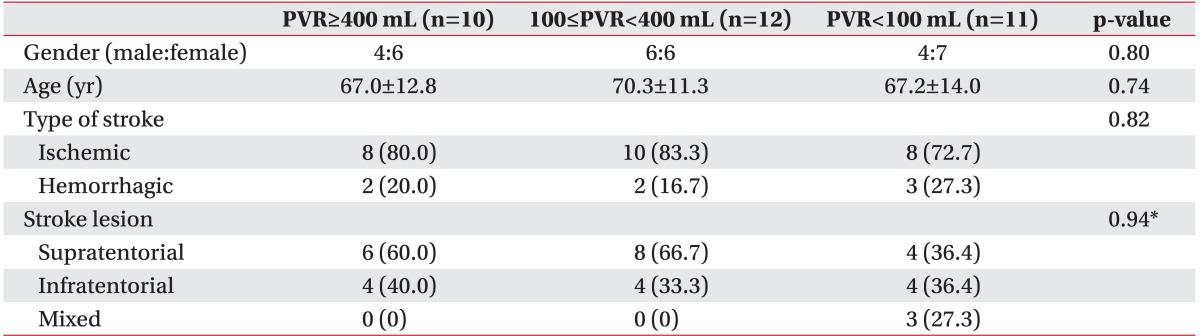
We recruited 33 consecutive patients (14 males and 19 females; mean age, 68.3±12.8 years; 26 with cerebral infarction and seven with cerebral hemorrhage; Table 1) among patients admitted to the Department of Rehabilitation Medicine of Asan Medical Center, according to the following criteria: 1) first stroke; 2) first bladder scan to measure post-void residual urine volume (PVR) within 30 days of onset; 3) PVR >100 mL, despite use of the maximum alpha-blocker dose (0.4 mg tamsulosin) and cholinergic agent (100 mg bethanechol) for 7 days; 4) no history of urinary symptoms before stroke; 5) no abnormal findings on a prostate exam; and 6) no urinary tract infection before admission and no serious medical complications during hospitalization, such as pneumonia or cardiac problems. This study protocol was approved by the Institutional Review Board of the participating university hospital.
Patients' demographic data
Evaluation of post-void residual urine volume
Indwelling catheters were removed from patients with urinary retention. PVR was measured in each patient within 24 hours of their transfer or admission. A bladder scan was used to measure PVR, which was checked more than three times each day. The accuracy of measuring PVR using a portable bladder scan has been demonstrated [10,11]. PVR was measured within 30 minutes after urination using the battery-powered, portable BladderScan BVI 3000 (Verathon Inc., Bothell, WA, USA). The scanner was placed on the suprapubic area and held stationary during scanning. Bladder diameter and urine volume were calculated from the scan data. After scanning, a B-mode image and an indication of bladder urine volume (in mL) appeared on the screen. All clinical procedures were performed by well-trained nurses. Urinary catheterization was performed if PVR was ≥400 mL. If a patient was unable to void, we measured urine volume every 2-4 hours until it was ≥400 mL, at which time catheterization was performed. The alpha-blocker was administered after 2 days of measuring PVR, and the alpha-blocker dose was increased if PVR was >200 mL. A cholinergic drug was administered when PVR remained >200 mL, despite administration of the maximum alpha-blocker dose for 2 days.
Voiding diaries were documented, including frequency of urination and voided volume. Residual urine was measured by BladderScan three times per day until discharge. Urinary retention was defined as PVR ≥100 mL. If PVR was always <100 mL, the drug dose was reduced in the order of the cholinergic agent and then the alpha-blocker. Drug-resistant urinary retention was defined as PVR ≥100 mL, despite maximum doses of the alpha-blocker and cholinergic agent for 7 days.
The outcomes of drug-resistant urinary retention at the early stage of stroke were divided into three groups according to PVR at discharge, i.e., <100 mL, ≥100 mL but <400 mL, and ≥400 mL or incapable of voiding.
Urodynamic assessment
An urodynamic study (UDS) was performed once during admission in patients who still had urinary retention after 7 days of drug administration to analyze the voiding dysfunction pattern. Drugs for managing urinary retention were discontinued the day before the UDS. The UDS was performed as described in the International Continence Society guidelines. Filling cystometry was performed with the patient in the supine position on an urodynamic table. The bladder was filled with normal saline at a medium (10-100 mL/min) filling rate. Bladder filling was terminated when maximum bladder capacity was reached, and a rectal catheter was inserted to measure intra-abdominal pressure. Vesical, abdominal, and detrusor pressures were monitored simultaneously during the filling and voiding phases. The drugs were restarted after the UDS. The mean duration from onset to the UDS was 24.6±9.4 days.
The UDS findings were defined as areflexic, if there was no contraction of the detrusor, and hyper-reflexic, if there were involuntary detrusor contractions during the filling phase.
Clinical data
Clinical data included the presence of diabetes mellitus, urinary tract infection after transfer or admission, a communication disorder, functional status, walking ability, cognitive function, and kidney function. A patient's communication problem was assessed by a speech therapist, and the presence of aphasia or a cognitive communication disorder was determined. Patient functional status was assessed using the Korean version of the Modified Barthel Index (K-MBI), as the validity and reliability of the K-MBI has been demonstrated [12]. Walking ability was assessed using the Functional Ambulation Category (FAC), which is based on the level of assistance required during a 15-m walk. The six categories are: 0, non-ambulatory; 1, need for continuous support from one person; 2, need for intermittent support from one person; 3, requires verbal supervision only; 4, help required on stairs and uneven surfaces; and 5, able to walk independently anywhere. The reliability and validity of the FAC have been well established [13]. Cognitive function was assessed using the Korean version of Mini-Mental State Examination (K-MMSE). The reliability and validity of the K-MMSE have been established [14]. Kidney function was assessed using estimated glomerular filtration rate (eGFR) from the Modification of Diet in Renal Disease formula [15]. If eGFR was <60 mL/min/1.73 m2, the patient was diagnosed with impaired kidney function.
Statistical analysis
Data were analyzed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). We divided the patients into two groups to evaluate differences in drug-resistant urinary retention according to brain lesion location, i.e., patients who had a supratentorial lesion (supratentorial group) and those with an infratentorial lesion (infratentorial group). Demographic data (i.e., sex, age, type of stroke, and lesion site) were compared between the patient groups using the Kruskal-Wallis test. The relationships between continuous variables (i.e., days from onset to transfer, total hospital days, K-MBI, FAC, and K-MMSE scores) and outcome were analyzed using Spearman correlation analysis, and the relationships between the categorical variables (i.e., diabetes mellitus, communication disorder, upper urinary tract infection, and kidney function) and outcome were analyzed using a linear-by-linear association analysis. Lesion type was analyzed after excluding patients with mixed lesions; thus, leaving only 30 patients.
RESULTS
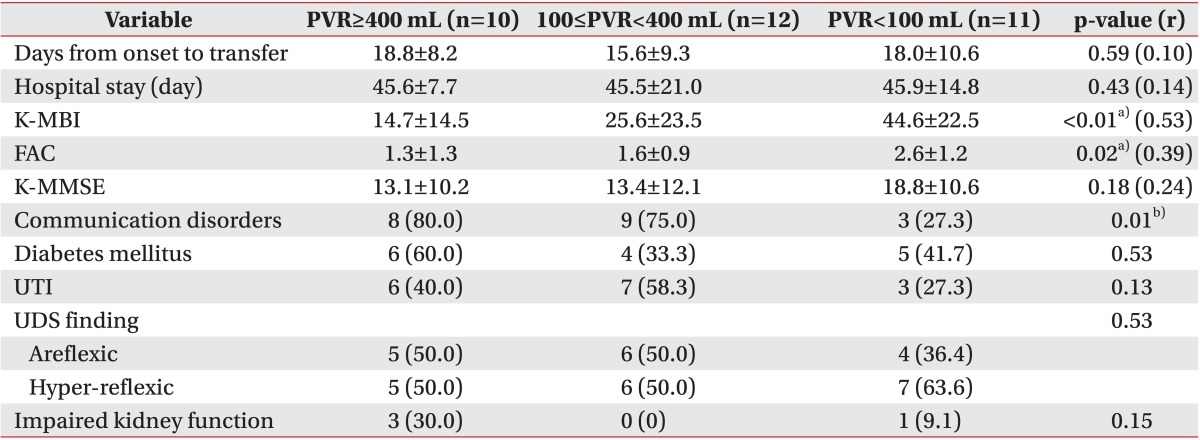
The mean time from onset to transfer of the 33 recruited patients was 17.4±9.3 days. The total number of hospital stay days was 45.7±15.4 (Table 2). At the time of discharge after rehabilitation, 10 patients (30.3%) could not void or their PVR was >400 mL more than once each day, nine needed intermittent catheterization and one patient had an indwelling catheter at discharge. Twelve patients (36.4%) could void, but their PVR was >100 mL but <400 mL. PVR of 11 patients (33.3%) was always <100 mL. As a result, 22 patients (66.7%) still had urinary retention at discharge.
Clinical characteristics according to post-residual volume
Eighteen (54.5%) of the 33 patients at admission showed an areflexic bladder on the UDS, and 15 (45.5%) showed a hyper-reflexic bladder. The mean K-MBI score was 28.6±23.6, the mean FAC score was 1.8±1.2, and the mean K-MMSE score was 15.1±11.0. Twenty patients (60.6%) had communication problems due to aphasia or a cognitive deficit. Fifteen patients (45.5%) were diagnosed with diabetes mellitus. Sixteen patients (48.5%) developed a urinary tract infection after transfer or admission and were administered antibiotic (ciprofloxacin or third-generation cephalosporin). In addition, we divided the patients into supratentorial and infratentorial groups according to lesion location. Eighteen patients (60.0%) were in the supratentorial group and 12 (40.0%) were in the infratentorial group, of the 30 patients after excluding the three with mixed lesions. eGFR of four patients (12.1%) was <60 mL/min/1.73 m2, but all values were >40 mL/min/1.73 m2.
Higher K-MBI score (r=0.53, p<0.01), FAC (r=0.39, p=0.02), and absence of a communication disorder (p=0.01) were correlated with urinary retention outcome. Other factors, such as patient sex (p=0.80), age (p=0.74), stroke type (infarction or hemorrhage; p=0.82), lesion type (supratentorial or infratentorial; p=0.94), days from onset to transfer (p=0.59), number of hospital days (p=0.43), K-MMSE score (p=0.18), diabetes mellitus (p=0.53), urinary tract infection (p=0.13), type of detrusor activity on the UDS (areflexic or hyper-reflexic; p=0.53), and impaired kidney function (p=0.15) were not correlated with patient prognosis.
DISCUSSION
Approximately 30% of the patients with drug-resistant urinary retention at the early stage after stroke required catheterization, as self-voiding was not possible, and their PVR after self-voiding was >400 mL. Nearly 40% of our study patients (PVR, 100-400 mL) still had urinary retention at discharge. Therefore, approximately one-third of the patients had resolved urinary retention at discharge after rehabilitative treatment. Post-stroke urinary retention is usually transient [4,16]. Unlike the outcomes of most patients with urinary retention, drug-resistant urinary retention did not fully recover in 70% of our patients. Therefore, clinicians can predict a poor outcome due to urinary retention in patients with drug-resistant urinary retention at an early stage of stroke in cases that cannot be controlled with an alpha-blocker and cholinergic agent.
Aphasia, diabetes mellitus, lower functional status at the time of admission, and urinary tract infection are factors associated with urinary retention [4]. In our study, higher functional status, walking ability, and the absence of a communication disorder were related with better urinary retention outcomes. Patients with lower functional status have more problems with transfer, and those with less walking ability are more likely to be bed ridden. Thus, they have a higher possibility of voiding in bed. Patients cannot use abdominal pressure to help void effectively when voiding in bed; thus, PVR may be higher. Patients with a communication disorder cannot voice their desire to void, so they are more likely to void in bed. The K-MBI score is an overall reflection of stroke severity. Patients with a lower K-MBI score have greater stroke severity and may have a higher risk for urinary retention.
Detrusor activities measured by the UDS were not correlated with outcome in our study. In one study, all patients with an areflexic bladder during the acute stroke period were normal on subsequent UDS findings [16]. Abnormal detrusor activity findings may be transient, so detrusor activities may not be correlated with outcome.
We also evaluated whether outcomes of drug-resistant urinary retention in patients at an early stage of stroke differed according to stroke lesion location. We divided the patients into supratentorial and infratentorial groups because the micturition centers are known to exist in the frontal lobe and pons. Burney et al. [2] performed a UDS in 60 patients with stroke and reported that patients with supratentorial lesions showed detrusor hyperactivity due to loss of voiding inhibition, whereas patients with infratentorial lesions showed detrusor hypoactivity due to loss of the excitation signal. Park et al. [17] reported that 11 patients (50%) with suprapontine lesions showed hyperactive detrusors, six (27.3%) with pontine lesions showed hypoactive detrusors, one (25%) of the patients had normal detrusor activity, and three (75%) were hypoactive. However, other studies have reported that urinary symptoms are not simply related to the location of a stroke lesion [3,18,19]. In one study, the UDS results were not characterized by the cerebrovascular injury site [20]. In agreement with these studies, we revealed that the voiding dysfunction pattern was not related to the location (supratentorial and infratentorial lesions) of the stroke lesion.
Kidney function did not correlate with urinary retention outcome. Kidney function can affect outcome, but nearly 90% of our patients had an eGFR >60 mL/min/1.73 m2. Additionally, four patients with mild kidney dysfunction had an eGFR >40 mL/min/1.73 m2. Therefore, the effects of kidney function may have been underestimated.
Only two studies have reported urinary retention outcomes. In 1980, Maru [16] reported that seven of 31 patients who had detrusor areflexia 48 hours after stroke experienced normalized bladder function, as seen on a subsequent UDS. In 2000, Kong and Young [4] reported that 22 of 23 patients (95.6%) resolved their urinary retention, 19 (82.6%) resolved it by discharge, and three (13.0%) within 2 months after discharge. In these two studies, urinary retention in patients at an early stage of stroke presented with a good prognosis. However, those studies did not consider urinary retention severity or responses to an alpha-blocker or cholinergic agent when enrolling patients. We only recruited patients who were drug-resistant to maximum doses of these drugs and revealed that drug-resistant urinary retention at the early stage of stroke resolved in only one-third of patients, compared to urinary retention in most patients with stroke.
In summary, the outcomes of patients with drug-resistant urinary retention at an early stage after stroke tended to be poor. Patients with poor functional status, walking ability, or a communication disorder had poorer outcomes. Urinary retention can cause several urinary system complications. A clean intermittent catheter (CIC) or Foley catheter should be applied for patients with a large volume of urine retained after self-voiding. However, several complications, such as urinary tract infection or catheter-related trauma, can occur in patients using Foley catheters [21]. Thus, clinicians should teach use of a CIC to patients with drug-resistant urinary retention before discharge, particularly those with low functional status.
This is the first study to evaluate outcomes of patients with drug-resistant urinary retention at an early stage of stroke. However, some limitations of our study should be considered when interpreting the results. First, we were unable to show more detailed patient data because this study was performed retrospectively. Second, the follow-up periods for urinary retention were of broad duration following stroke onset. Lastly, the number of study subjects was relatively small. Thus, further complementary studies are needed to verify our results.
Notes
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.