INTRODUCTION
Stroke is a condition that results in high mortality rates and severe disabilities. Most stroke survivors can and do experience improvements in their functional abilities, but the amount, rate, timing, pattern, type, and ultimate outcome of the improvements differ across patients and situations [1]. Numerous studies were conducted on the prognostic factors of acute ischemic stroke. Stroke severity and patient age are the main predictors of stroke outcome in the acute phase [2,3,4,5,6]. Additional important predictors include functional status prior to stroke, presence of comorbid medical conditions, etiologies and the vascular territories affected [7,8,9,10].
Diabetes mellitus is one of the established risk factors for stroke. It has been demonstrated that diabetic patients had worse residual neurological deficits and functional outcome when compared with nondiabetic patients [11,12,13]. Hyperglycemia occurred in up to one-third of patients with acute ischemic stroke and was associated with higher mortalities independent of age and stroke severity [14,15]. However, few studies have assessed the effects of prestroke glycemic control status on clinical outcomes in acute stroke patients. In a study published in 2011, the association between prestroke glycemic control status and neurological or functional outcomes was evaluated in 3,627 patients with first-ever ischemic stroke. It was suggested that the serum hemoglobin A1c level on admission was a significant independent predictor for clinical outcomes [16]. However, clinical characteristics such as age, laboratory data, risk factors and stroke subtype were diverse in the previous study [16].
Hemoglobin A1c has a direct relationship with mean glycemia because erythrocytes are continuously glycated during their 120-day lifespan, which means that the rate of formation of glycated hemoglobin, also called HbA1c, is proportional to the ambient glucose concentration [17]. In the diabetes control and complication trial, an HbA1c of 6% corresponded to a mean serum glucose level of 135 mg/dL, and the measurement of HbA1c has been the primary index of glycemia [17]. An HbA1c test can be used to diagnose pre-diabetes or diabetes and check the long-term control of blood glucose levels in people with diabetes. Serum blood glucose level changes during the day for many reasons, including medicine, diet, exercise, and the level of insulin in the blood, while the HbA1c test result is not affected by any recent changes [18]. HbA1c is independent risk factor for diabetic complication, with the risks of macrovascular events, such as cardiovascular death, non-fatal myocardial infarction or non-fatal stroke, and death only clearly lower when down at levels of 7% [19,20].
The middle cerebral artery (MCA) and its branches are the most commonly affected brain vessels in cerebral infarction. The MCA territory is involved in more than twothirds of all brain infarcts in a number of stroke registries. Of MCA territory infarcts, 33% involve the deep MCA territory [21]. Diabetes influences the various vascular lesions in brain ischemia, and the predominant type of brain infarction is deep subcortical brain infarction [22]. In patients with ischemic stroke of the deep branch of the MCA, more than 75% of these patients have hypertension or diabetes [23].
The aim of this study was to elucidate the association between glycemic control status, defined by HbA1c on admission, and clinical outcomes in patients with acute ischemic stroke in the deep branch of MCA y territories. Vascular territories were confined to the deep branch of MCA territories in order to eliminate its effect on outcomes.
MATERIALS AND METHODS
Subjects
Sixty-five stroke patients who were admitted to Dankook University Hospital from May 2008 to December 2014 were enrolled. Inclusion criteria were diagnosis of first-ever ischemic stroke of the deep branch of the middle cerebral artery, the location of which was confirmed by diffusion weighted image and apparent diffusion coefficient of brain magnetic resonance imaging. Exclusion criteria were as follows: 1) insufficient communication skills, 2) unconsciousness, 3) aphasia, 4) visual loss, 5) hearing loss, 6) concurrent neurodegenerative diseases (e.g. Parkinson disease), or 7) prestroke impairment in daily living.
Serum HbA1c levels were measured at admission. Subjects were classified into two groups according to the level of HbA1c. The low HbA1c group consisted of subjects with HbA1c <7.0%, and the high HbA1c group included subjects with HbA1c ≥7.0%. All subjects underwent conventional post stroke rehabilitation programs including exercise therapy and occupational therapy in 30-minute sessions, twice daily, according to their impairments and functions.
Baseline characteristics
Baseline characteristics included age, sex, comorbidities and stroke risk factors such as diabetes, hypertension, atrial fibrillation, hyperhomocysteinemia, hypercholesterolemia, body mass index, and smoking. Diabetes and hypertension were each defined according to previous diagnosis or current treatment with drugs. Microvascular complications of diabetes such as retinopathy and nephropathy were also evaluated. Retinopathy is the development of proliferative retinopathy, macular edema or diabetes-related blindness. Nephropathy is the development of microalbuminuria defined as a urinary albumin/creatinine ratio of more than 33.9 mg or a doubling of the serum creatinine level to at least 200 µmol/L, with the need for renal-replacement therapy. Atrial fibrillation was evaluated through electrocardiography on admission or history of chronic atrial fibrillation. Serum glucose, cholesterol, homocysteine levels and body mass indices were measured on admission. Smoking was defined as history of smoking for more than 5 years.
Outcome measurements
Stroke severities were evaluated by using the National Institutes of Health Stroke Scale (NIHSS) score on admission. The NIHSS is a tool used to objectively quantify the impairment caused by a stroke, and is composed of 11 items: level of consciousness, horizontal eye movement, visual field test, facial palsy, motor arm, motor leg, limb ataxia, sensory, language, speech, extinction and inattention. Each of these specific abilities is given a score between 0 and 4. For each item, a score of 0 typically indicates normal function in that specific ability, while a higher score is indicative of some level of impairment.
Functional status was measured using the Korean version of Modified Barthel Index (K-MBI) and Functional Independence Measure (FIM) at admission and discharge. The MBI is an ordinal scale used to measure performance in activities of daily living. It consists of 10 items: personal hygiene, bathing, eating, toileting, stair climbing, dressing, bowel control, bladder control, ambulation or wheelchair, and chair-bed transfer. The FIM measures the level of a patient's disability and indicates how much assistance is required for the individual to carry out activities of daily living. It has 18 items assessing 6 areas of function. These items fall into two domains, motor (13 items) and cognitive (5 items).
Cognitive functions were evaluated using the Korean version of Mini-Mental State Examination (MMSE-K) and Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) at admission. The MMSE-K is a brief 30 point questionnaire test that is used to screen for cognitive impairment. It is composed of 8 categories: orientation to time, orientation to place, registration, attention and calculation, recall, language, repetition, and complex commands. LOTCA includes 25 subtests in 6 cognitive areas: orientation, visual and spatial perception, praxis, visuomotor organization, and thinking operations.
Statistical analysis
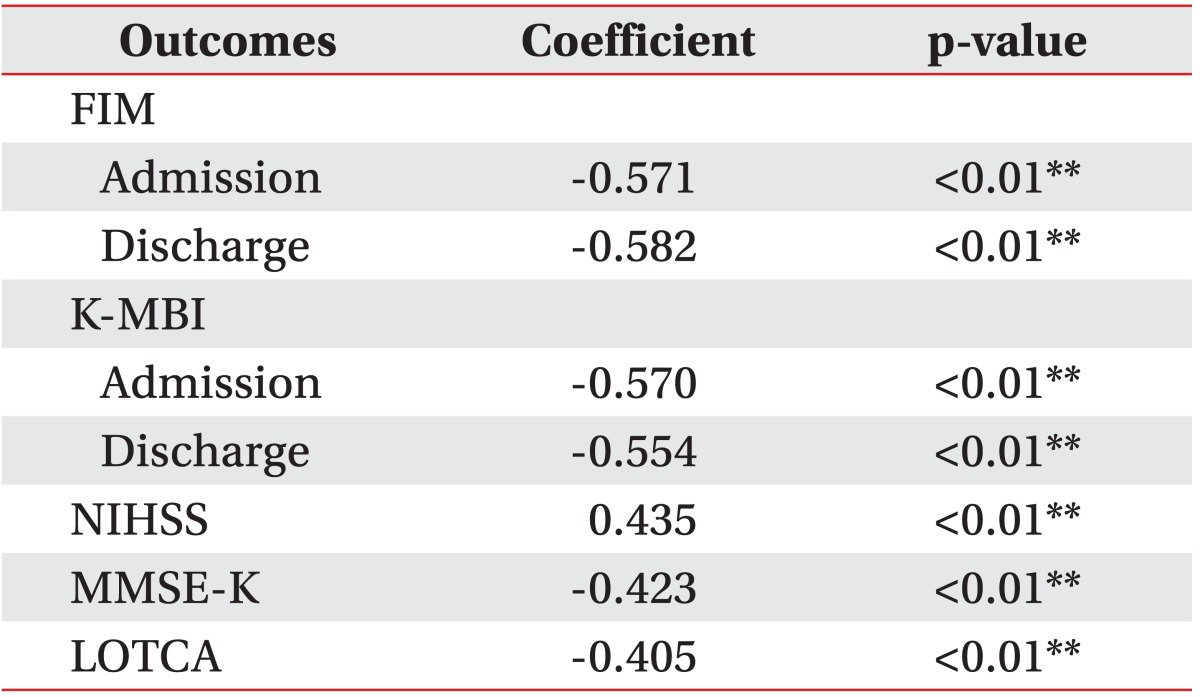
The baseline characteristics and outcome measurements between the two groups were compared using the chi-square test or Fisher exact test and the independent t-test. The paired t-test was used to compare changes in K-MBI and FIM scores during hospitalization. The Pearson correlation analysis was performed to delineate the relationships between serum blood glucose and outcome measurements. Statistical significance level was set at 0.05. Data are given as mean±standard deviation. Statistical analyses were performed using SPSS ver. 12.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Baseline characteristics
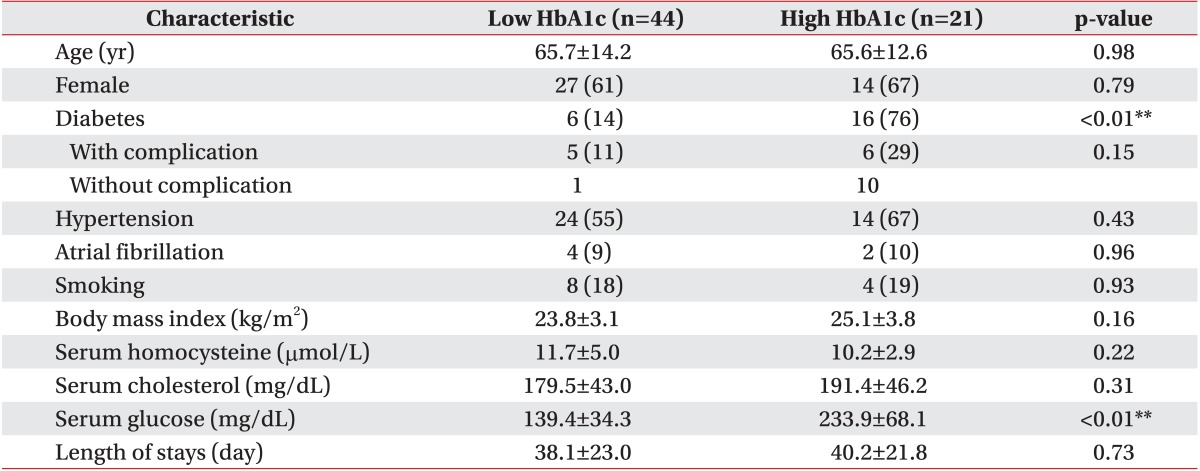
Of the 65 subjects, 24 were male and 41 female with age of 67.3±13.1 years. The low HbA1c group consisted of 44 subjects (aged 65.7±14.2 years), while the high HbA1c group consisted of 21 subjects (aged 65.6±12.6 years). No statistically significant difference was found between the groups for age and gender.
The mean HbA1c levels were 5.8%±0.5% in the low HbA1c group and 8.5%±1.4% in the high HbA1c group. Twenty-six subjects had diabetes and 11 subjects had diabetic complications. Diabetes was significantly higher in the high HbA1c group (p<0.01) but complications were not different between both groups. Thirty-eight patients had hypertension and six patients had atrial fibrillation. Other risk factors for stroke are shown in Table 1. Both groups did not have any difference in risk factors for stoke. The length of stays was 38.1±23.0 days in the low HbA1c group, and 40.2±21.8 days in the high HbA1c group.
Outcome measures
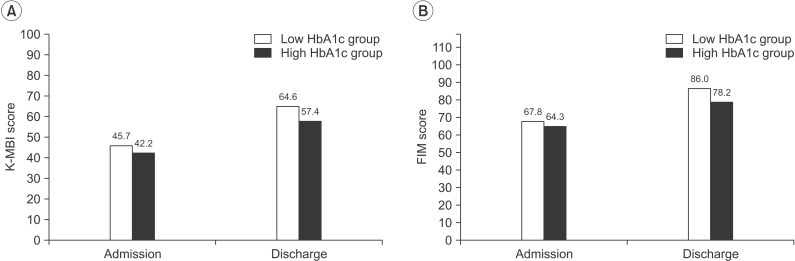
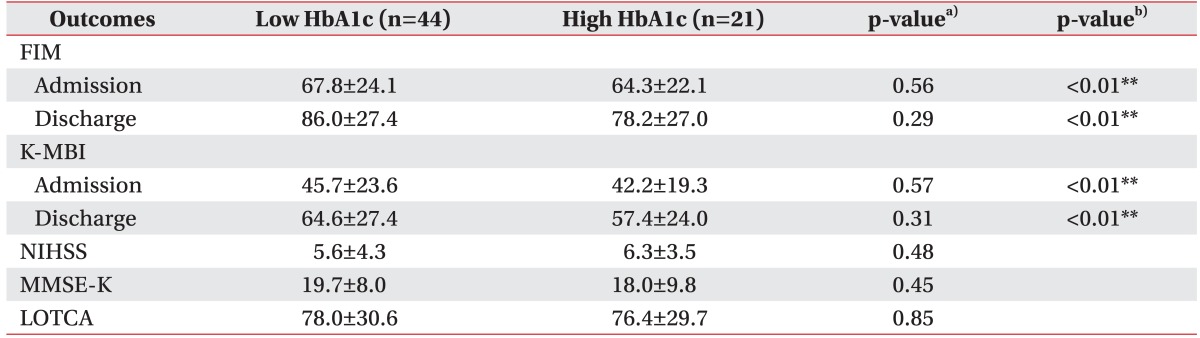
No statistically significant differences were found in the K-MBI, FIM, NIHSS, MMSE-K, and LOTCA scores between two groups (Table 2). Functional status confirmed by FIM and K-MBI was improved in all the subjects at discharge, but there were no differences between the groups in the degree of improvements (Fig. 1).
DISCUSSION
We investigated whether glycemic control status affects the clinical outcome of acute ischemic stroke. The results of our study indicate that all the subjects showed significant functional recovery and similar clinical outcomes regardless of HbA1c levels, and a higher serum blood glucose level tended to be associated with poor clinical outcomes.
Several previous studies have found that neurological deterioration and a poor functional outcome were more common in patients with poor prestroke glycemic control. The level of HbA1c on admission was a predictor for poor survival and unfavorable functional outcomes [16,24,25,26]. In contrast, no statistically significant differences were found between the two groups in our study in terms of clinical outcome and functional recovery.
Several studies suggest that hyperglycemia after stroke had adverse effects on the clinical course of ischemic stroke, and was associated with the expansion of infarct volume as a result of neurotoxicity [26,27,28,29]. These results were also shown in the present study. However, in some studies, prestroke hyperglycemia was not associated with poststroke fasting blood glucose level [30,31]. A high proportion of stroke patients might have developed hyperglycemia even in the absence of preexisting diabetes since acute stroke itself is an acute stress condition [32,33].
Other studies have demonstrated that blood glucose level after stroke was associated with stroke severity, but glycosylated hemoglobin (HbA1c) did not show any association with stroke severity [34,35]. This is consistent with our results. Therefore, clinical outcomes of ischemic stroke might be associated with poststroke hyperglycemia rather than prestroke glycemic control status (HbA1c on admission).
It should be noted that this study has several limitations. First, our study has low power attributable to the small sample size, and thus the results should be interpreted with caution. Second, neurological and cognitive improvements were not assessed on discharge, and only functional evaluations have been conducted in follow-up. Third, patients with insufficient communication skills, unconsciousness, aphasia, visual loss and hearing loss were excluded. We therefore do not know the effect of HbA1c in stroke patients with severe sensory deficits. Fourth, our sample was restricted to acute patients with ischemic stroke. Further studies are needed with larger samples of patients with severe deficits, and with long-term follow-ups.
In conclusion, it is suggested that HbA1c might not have any predictive value for clinical outcome in patients with ischemic stroke in the deep branch of the middle cerebral artery.