INTRODUCTION
Ataxia is known to occur in a number of neurologic diseases, such as stroke, and often has both clinical and diagnostic significance. Although muscle power is relatively well maintained, appropriate motor functions cannot be performed due to dysmetria and abnormal motor responses [1]. Also, ataxia affects the neurological function of motor coordination, which may in turn affect fundamental activities, such as eye movement, speech, muscle tone, gait, and stance [2]. Ataxia may disturb performance of activities important for daily living as well. Therefore, assessment of ataxia is important for the planning and goal setting of rehabilitation treatment. The evaluation tools used for ataxia assessment include International Cooperative Ataxia Rating Scale (ICARS) [3] and Friedreich Ataxia Rating scale (FARS) [4]. However, ICARS consists of 19 items that the application of this scale in daily practice is limited. FARS is not suitable for ataxic stroke patients, because it was developed for the evaluation of Friedreich ataxia. The Scale for the Assessment and Rating of Ataxia (SARA) is a new ataxia scale that was initially validated in spinocerebellar ataxia (SCA) patients. It includes 8 items reflecting neurological manifestations of cerebellar ataxia, but does not consider nonataxia symptoms [5].
We performed this study to translate SARA into Korean and investigate the intra-rater and inter-rater reliability of the Korean version of the SARA (K-SARA) for ataxic stroke patients.
MATERIALS AND METHODS
Translation of SARA into the Korean language
We obtained permission from Tanja Schmitz-Hubsch, the original author of SARA (Appendix 1), for the Korean translation of the SARA. Two physiatrists fluent in English translated the SARA into the Korean language, version 1-A and 1-B, and they discussed the 2 versions. A reconciled version (version 2) was achieved by consensus and it was back-translated into English by 2 other translators (who majored in English Literature and skillful English and Korean; version 3-A and 3-B). Version 3-A and 3-B were reviewed and compared with the original version by 2 physiatrists.
A preliminary study regarding the final product (K-SARA, Appendix 2) was conducted for ataxic stroke patients who were admitted to the rehabilitation unit of Konkuk University Medical Center.
Study population
The subjects of this study consisted of 60 ataxic stroke patients who were admitted to the rehabilitation unit of Konkuk University Medical Center between September 1, 2012 and July 31, 2013. Patients were excluded if they had previous brain diseases, difficulty in participating due to severe cognitive dysfunction, or severe orthopedic problems, such as loss of their lower extremities, fracture or arthritis, or subarachnoid hemorrhage.
Assessment of K-SARA
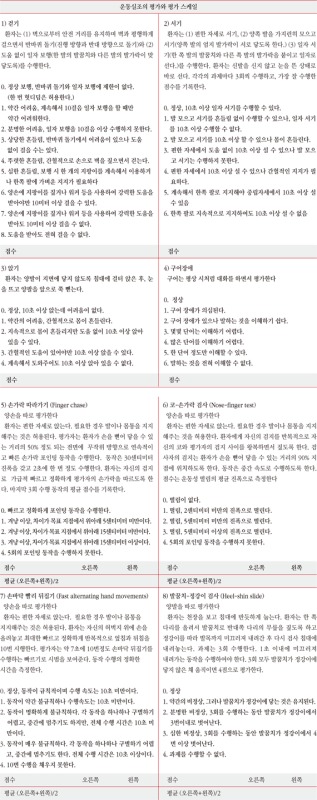
K-SARA has 8 items with a total score rating from 0 (no ataxia) to 40 (most severe ataxia): 1, gait (score 0 to 8); 2, stance (score 0 to 6); 3, sitting (score 0 to 4); 4, speech disturbance (score 0 to 6); 5, finger chase (score 0 to 4); 6, nose-finger test (score 0 to 4); 7, fast alternative hand movement (score 0 to 4); and 8, heel-shin slide (score 0 to 4). Limb kinetic functions (items 5 to 8) are rated independently for both sides, and the arithmetic mean of both sides is included in the SARA total score.
All 60 patients were assessed on the same day by 2 examiners (1 physician and 1 occupational therapist). The first assessment was conducted on the day of admission to the rehabilitation unit. A second assessment was conducted the next day to evaluate the inter-test consistency of the test. Rehabilitation treatment or drug adjustment was not performed between the 2 assessments.
Usefulness of K-SARA
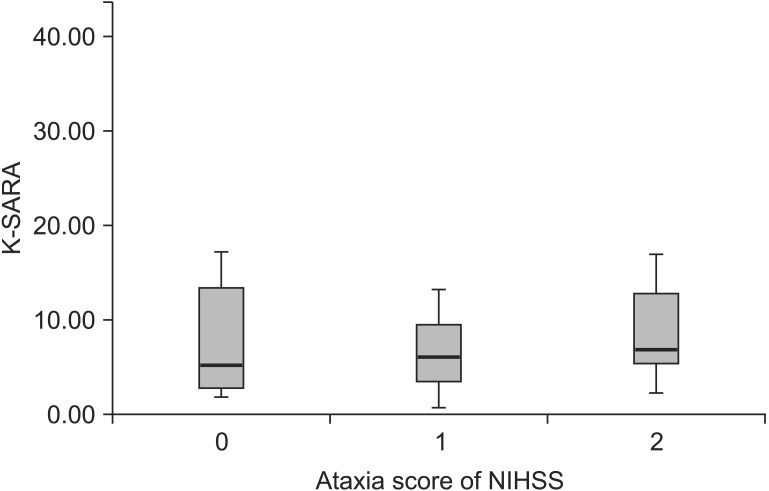
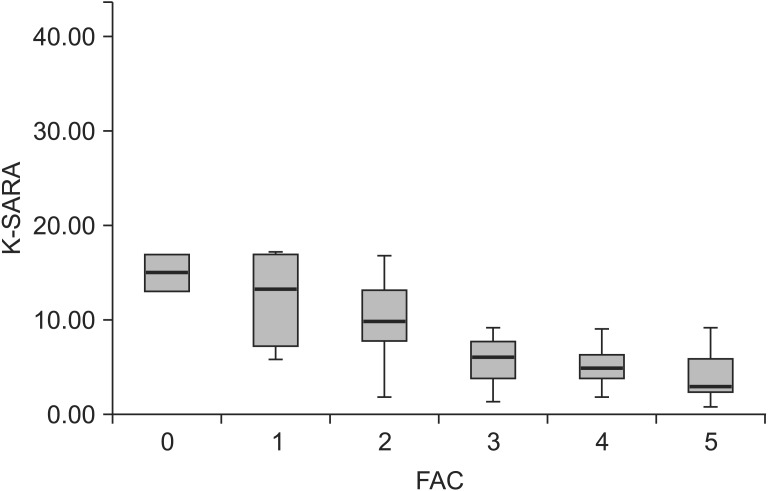
The National Institutes of Health Stroke Scale (NIHSS) and Functional Ambulation Category (FAC) were assessed in all subjects. The patients were divided into 3 groups by the ataxia subscale of NIHSS: 0, no ataxia symptom; 1, ataxia present in the upper limb or lower limb; and 2, ataxia present in the upper limb and lower limb. Additionally, ambulation status was divided into 5 groups according to the FAC: 0, nonfunctional ambulator; 1, ambulator dependent for physical assistance (level II); 2, ambulator dependent for physical assistance (level I); 3, ambulator dependent for supervision; 4, ambulator independent level surface only; and 5, ambulator independent. The mean K-SARA score was compared between the groups.
Statistical analysis
We used the intraclass correlation coefficients (ICC) in order to evaluate the reliability of the K-SARA score. An observed p-value <0.05 was considered statistically significant. Statistical analyses were conducted using SPSS ver. 17.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
General characteristics of the patients
We evaluated sixty patients with ataxic stroke. Table 1 summarized their demographic and clinical characteristics. The mean age at examination was 64.03±12.12 (range, 42 to 87 years). Among the patients, 28 were male and 32 were female. The disease duration was 37.13±42.57 days.
The inter-rater reliability for K-SARA
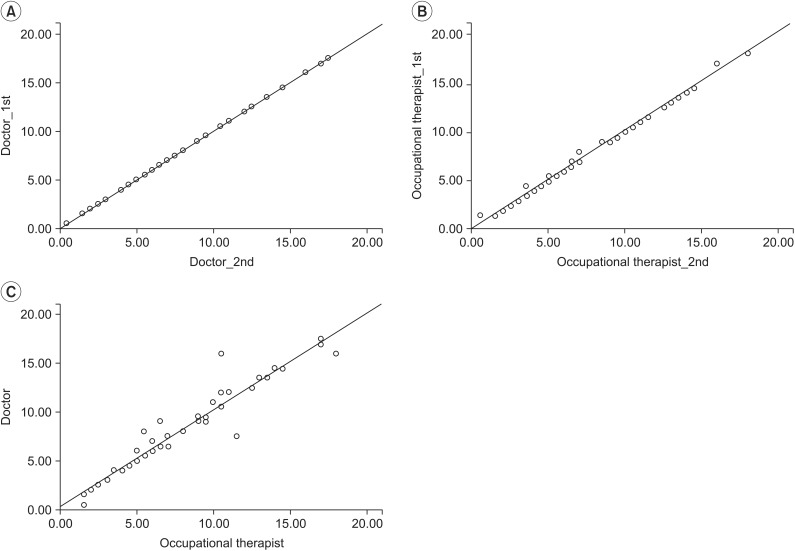
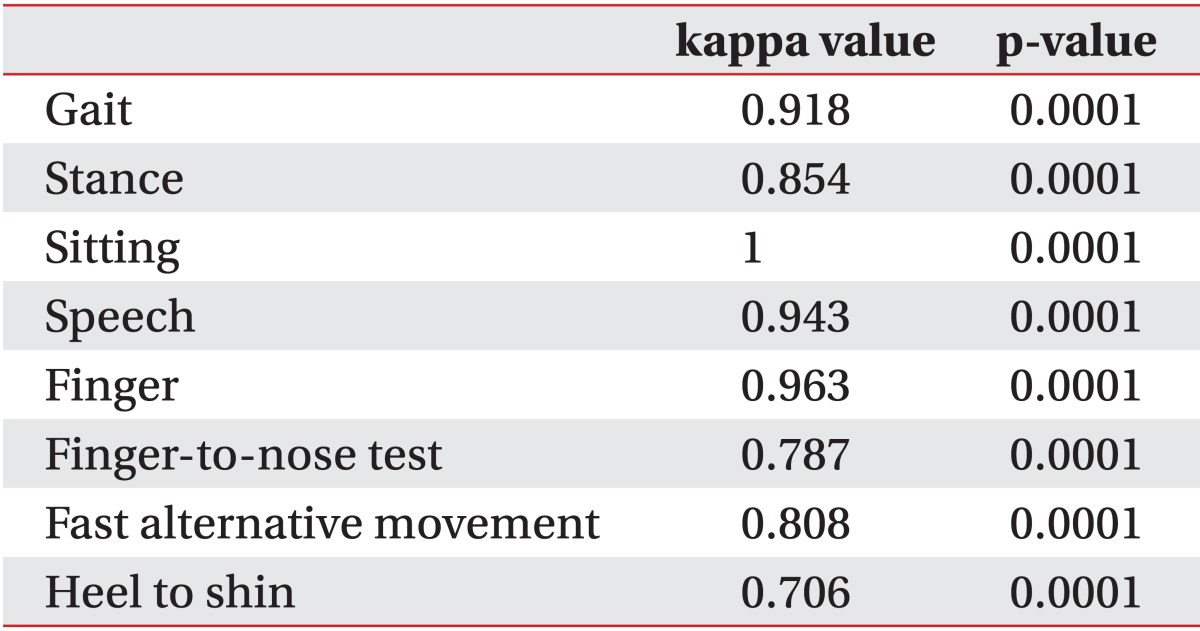
Inter-rater reliability was analyzed based on the results of assessment of each item of K-SARA by 1 occupational therapist and 1 physician. Inter-rater reliability of the total K-SARA score was very high, with an ICC of 0.985 (p<0.01). The inter-rater consistency of each item resulted in weighted kappa scores showing a high level of consistency (Table 2).
Usefulness of K-SARA
There was no significant difference in the mean K-SARA between the groups divided by the ataxia subscale of NIHSS (Fig. 2). The K-SARA score for the gait status had means of 15.12, 12.41, 9.92, 6.03, 5.18, and 4.16 points for FAC grades 0, 1, 2, 3, 4, and 5, respectively (p<0.001) (Fig. 3). Significant differences in the K-SARA scores were found in the aforementioned classifications.
DISCUSSION
The objective of this study was to translate and validate SARA into Korean. In order to perform this goal, 60 ataxic stroke patients were assessed using the K-SARA. The results showed high intra-rater reliability not only for physiatrist but also occupational therapist and high inter-rater correlation.
Recently, many disease-specific scales for some types of ataxic disorders have been developed, including FARS for Friedreich ataxia [4] and the Unified Multiple System Atrophy Rating Scale (UMSARS) [6] for multiple system atrophy. Schmahmann et al. [7] developed a Brief Ataxia Rating Scale (BARS), based on a modified form of the International Cooperative Ataxia Rating Scale (ICARS). The ICARS has been widely used as a tool for the evaluation of the severity and treatment efficacy of cerebellar ataxia. ICARS is a semi-quantitative 100-point scale, consisting of 19 items divided into 4 subscores: posture and gait, kinematic functions, speech, and ocular movements. However, the daily use of this scale in ataxic patients is difficult due to its many assessment items [3].
Schmitz-Hubsch et al. [5] recently proposed a SARA. This new assessment tool has fewer assessment items than ICARS and therefore has the advantage of easier daily assessment of ataxia. SARA has been demonstrated for its reliability and validity in 64 ataxic patients [8]. Studies on the usefulness of SARA have been conducted to compare it with the existing ICARS and Barthel Index in cerebellar ataxia patients [9]. Kim et al. [10] reported that SARA is useful in ataxic stroke patients and showed a significant correlation with the Modified Barthel Index, Berg Balance Scale, and gait status. Thus, SARA has been proven helpful in predicting the dependency of ADL and gait status and developing treatment plans [10].
However, these tools were developed in the West and verified in English. A standardized assessment tool for Koreans was needed, with translation and modification suited to the Korean language and culture.
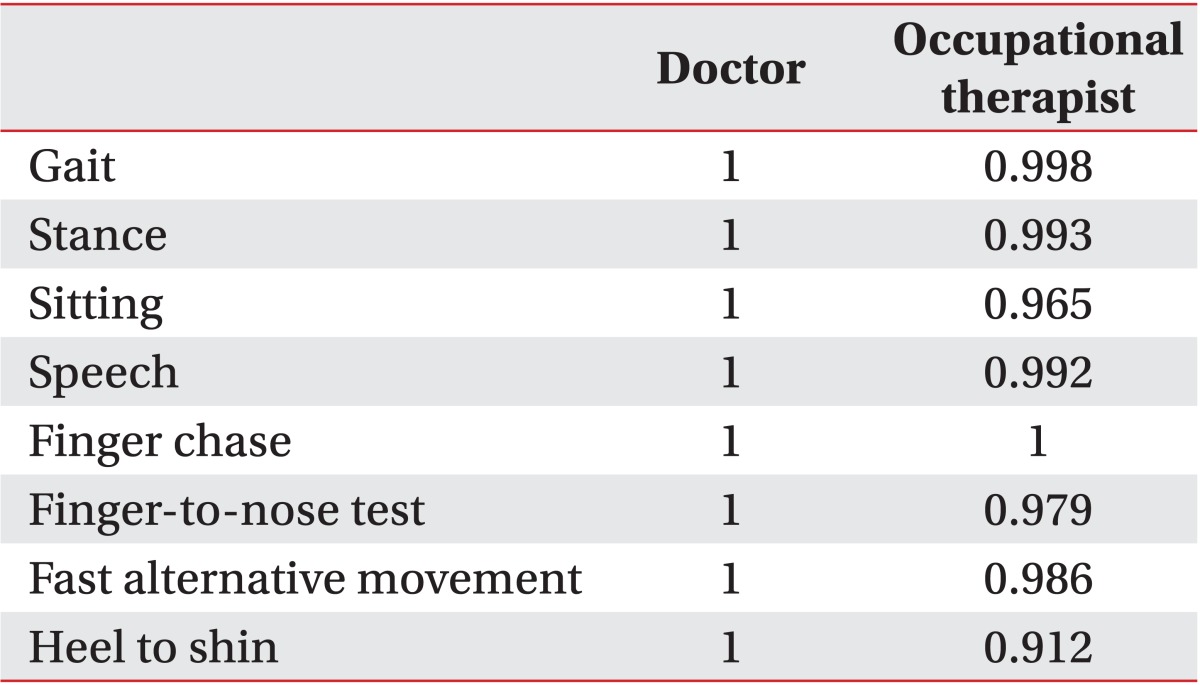
Therefore, we translated the SARA to Korean with adequate internal consistence. We were not required to change the words or sentences as the scale was very simple. The assessment time of K-SARA was within 5 minutes. All investigators commented that the Korean version was as easy to understand as the original version. Additionally, the intra-rater reliability of K-SARA (ICC=0.965 or ICC=1) was similar with intra-rater reliability (ICC=0.99) of the original version [8], indicative of no problems in the Korean adaptation of SARA items.
To establish the treatment goal and predict the prognosis of stroke patients during rehabilitation treatment, their status before the initiation of rehabilitation treatment must be accurately assessed.
The NIHSS is used for evaluation of initial impairment and follow-up of the neurologic status in stroke patients [11,12]. NIHSS is useful in the assessment of overall neurologic status of stroke patients, but has just 1 item to assess limb ataxia. The finger-nose-finger test and heel to shin test use the following scale: 0, no ataxia symptoms; 1, ataxia present in the upper limb or lower limb; and 2, ataxia present in the upper limb and lower limb. However, these 2 tests only assess the presence of limb ataxia, which are insufficient for the assessment of the overall ataxia symptoms, including truncal ataxia. There are 1 item to evaluate dysarthria (dysarthria score of K-SARA=6) and 3 items to evaluate truncal ataxia such as sitting and standing balance and gait status (total truncal ataxia score of K-SARA=18), other than items that evaluate limb ataxia (total limb score of K-SARA=16) in K-SARA. Additionally, more detailed evaluation for limb ataxia is possible because there are 2 more items for evaluation of limb ataxia (finger chase test, fast alternative hand movements test), besides items of NIHSS (nose-finger test, heel-shin test). We found no difference in K-SARA score between 0, 1, and 2 points. As mentioned above, the main reason for this may lie in the limitation of NIHSS to assessment for truncal ataxia or severity of limb ataxia. Thus, if ataxia symptoms are present, the K-SARA should be evaluated for more appropriate treatment planning.
K-SARA also showed significant differences in scores depending on the gait status assessed by FAC. The lower FAC showed higher K-SARA score. The results presented here closely resembled those previous reported in ataxia stroke patients [10], where patients with more severe ataxia showed poor gait status. Proper management planning can be accomplished by predicting the patient's balance and gait status by K-SARA.
In conclusion, the SARA was translated and validated into Korean language with good reliability and validity. The Korean SARA can be clinically useful for disorder assessment and rehabilitation planning.