Unmet Healthcare Needs in People with Disabilities: Comparison with the General Population in Korea
Article information
Abstract
Objective
To determine the degree of disparity in unmet healthcare needs between people with disabilities and the general population in South Korea, and to analyze their perspective reasons.
Method
Survey results of 9,744 subjects that participated in the 4th Korea National Health and Nutrition Examination Survey and 7,000 people that participated in the 2008 Survey of Disabled people were used in this population-based cross-sectional study. Unmet healthcare needs were identified as reporting experience during the last 12 months when there was a need to see a doctor, but were unable to get it. We assessed unmet healthcare needs by demographic variables, social variables and characteristics of disability. Chi-square test and logistic regression were used to determine which variables were related to unmet healthcare needs.
Results
A total of 22.1% of people with disabilities and 22.8% of the general population had unmet healthcare needs. However, brain impairment (25.3%) and physical impairment (25.2%) had more unmet healthcare needs than the general population and other disabilities. Unmet healthcare needs of people with disabilities was related to sex, age, self-perceived health, marital status, income, occupation and category of disability. Whereas the reasons for unmet healthcare needs in people with disabilities were lack of money (57.3%) and inaccessible transportation (12.8%), those for the general population were no available time (30.2%) and mild symptoms (23.8%).
Conclusion
Brain and physical impairment cases with limitations to accessible transportation had the higher unmet healthcare needs. In addition, the reasons for people with these disabilities were more environmental than those of the general population.
INTRODUCTION
People with disabilities have restrictions on medical use due to physical, social and cultural barriers. Physical barriers include uneven geographical distribution of medical facilities, difficulty of moving to hospitals and restrictions of communication within the health care system.1,2 Social barriers include the burden of health care costs because most disabled persons are in a low-income state.1,3 Cultural barriers include fear of social discrimination.4
Since timely healthcare is somewhat limited in access, the disease becomes aggravated and people with disabilities have unnecessary hospitalization.5 In addition, the prevalence of chronic disease is 2 to 3 times higher in patients with disabilities than in those without. Therefore, secondary functional losses such as heart disease or stroke can be added to their primary disabilities.6
Therefore, people with disabilities meet their healthcare needs less than those without disabilities. In particular, although the introduction of the national medical insurance policy gradually improves their access to medical facilities, the medical insurance policy in Korea has been criticized due to financial burdens and the imbalance of the medical infrastructure.7 Thus, it is necessary to know health care needs from the healthcare consumers' point of view to evaluate the overall health care system.8 Also, while the previous concept of medical needs was to treat diseases, the current one has become more extensive and has included disease prevention and health promotion in areas where unmet healthcare needs have increased.9 In Korea, there have only been a few studies on healthcare needs besides a previous study on the general population based on the Korea National Health and Nutrition Examination Survey (KNHANES).10 Since questions pertaining to unmet healthcare needs and their perspective reasons were added in the 2008 Survey of Disabled People, it has become possible to compare unmet healthcare needs between people with disabilities and the general population.
Therefore, in this study, we examined the degree of disparity and related factors between people with disabilities and the general population to compare the amount and perspective reasons of unmet healthcare needs between people with disabilities and the general population. In addition, we separately analyzed disabilities with mobility limitation. Finally, we searched for a method of promoting healthcare needs in people with disabilities.
MATERIALS AND METHODS
Study subjects
Total responses of 7,000 persons who participated in the 2008 Survey of Disabled People were included in this study. The Survey of Disabled People has been conducted by the Ministry of Health and Welfare and Korea Institute for Health and Social Affairs as a national survey every 5 years since 1980. In 2007, a revised law of welfare of disabled people enacted a provision that the national survey is conducted every 3 years and this was the seventh survey. In the 2008 Nationwide Survey of Disabled People, 7000 persons with disabilities out of 2,137,226 registered persons were surveyed between September and November 2008.
As for the general population, the study included 6802 out of 9,744 subjects who had participated in the fourth KNHANES in 2008 and had reported unmet healthcare needs. The KNHANES has generated representative fundamental statistical data for establishing a goal of national health promotion, evaluating plans and developing health promotion programs by surveys on health status, health behaviors and nutritional status.
Methods
Definition of unmet healthcare needs
Each participant was asked the question "Have you ever experienced any difficulties in visiting a hospital when you needed to see a doctor over the last 12 months?" All participants reported either "Yes" or "No." The proportion of the participants who reported "Yes" was calculated, which was defined as unmet healthcare needs during the last 12 months.
Reasons for unmet healthcare needs
The survey questions included ① lack of money ② difficulties in getting appointments at hospitals ③ inaccessible transportation ④ no available time ⑤ discouraged due to a long waiting time ⑥ mild symptoms and ⑦ other reasons.
Dependent variables
Factors that influenced medical use included demographic factors, socio-psychological factors, economical factors, the amount and quality of medical resources in the community, and the distribution of medical resources. In this study, we compared socio-demographic factors between the 2 surveys and additionally analyzed the factors of disabilities in the Survey of Disabled People.
(1) Demographic variables; ① Category: Gender, age, presence of chronic disease and self-perceived health. ② How to measure: The participants were first divided into males and females, and then into 4 age groups: the 0-19 years, 20-39 years, 40-59 years and >60 years. The presence of chronic disease over a period of 3 months was defined as a chronic disease in the Survey of Disabled People. In the KNHANES, it was defined when the subject reported their own disease as chronic. For the evaluation of self-perceived health, each participant was asked the question "What do you think about your health status?" The reports of all participants were divided into 5 categories: ① very good, ② good, ③ moderate, ④ poor and ⑤ very poor.
(2) Sociological variables; ① Category: Marital status, income, occupation, health insurance and educational levels. ② How to Measure: Marital status was divided into married, unmarried or no spouse (widowed/separated/divorced). Income was divided into 4 quartiles. We used monthly household-equalized income. The cutoff of Q1 was 49.5, that of Q2 was 106.07, and that of Q3 was 176.78 (million won).
Monthly household - equlized income = household income / √the number of family members
Occupation was divided into white collar jobs, blue collar jobs and no occupation (housewife, student or unemployed). Medical insurance was classified as 3 categories (employee, self-employed or Medicaid). Education was classified as ≤elementary school, elementary school to high school and ≥university.
(3) Variables of Disability; ① Category: Reclassified category of disability, grade and severity. ② How to measure: The disabled condition was classified into 3 categories: external physical disabilities (physical impairment, brain impairment, visual impairment, auditory impairment, linguistic impairment and facial deformity), internal organ disabilities (renal, heart liver, respiratory, intestinal and urinary tract dysfunctions), and mental disabilities (epilepsy, mental retardation, developmental delay and mental impairment).11 Physical and brain impairments, accompanied by impaired mobility were separately analyzed. Disability severity was classified as mild or severe according to their disability grade.
Weight
A sample weight was assigned to each sample person by the following 3 steps: calculating base weight, adjusting for non-responses and post-stratification adjustment to match the total member of the previous census population control subjects. ① The KNHANES: The concept of the circular sample was introduced for survey results of the 4 different teams. A total of 4,600 households (2,300 households each in the first and second years of the study) were surveyed. There were 9,744 participants and the participation rate was 77.8%. Through a complex sample design implemented in proportional and systematic sampling and post-weighting, our sample reflected the population structure in Korea. ② Survey in disabled people: Of the 12,342 registered disabled participants in 208 sample areas, 7,000 were surveyed between September 6 and November 30, 2008 by stratified 2-phase sampling. We adjusted weight in order to represent the disabled people. We calculated the inverse probability of extraction and adjusted the value by adjusting rank ratio.
Statistical analysis
Statistical analyses were performed using SPSS version 17.0. We assessed unmet healthcare needs using demographic variables, social variables and disability characteristics. The chi-square test and logistic regression were used to determine variables related to unmet healthcare needs.
RESULTS
Demographic characteristics
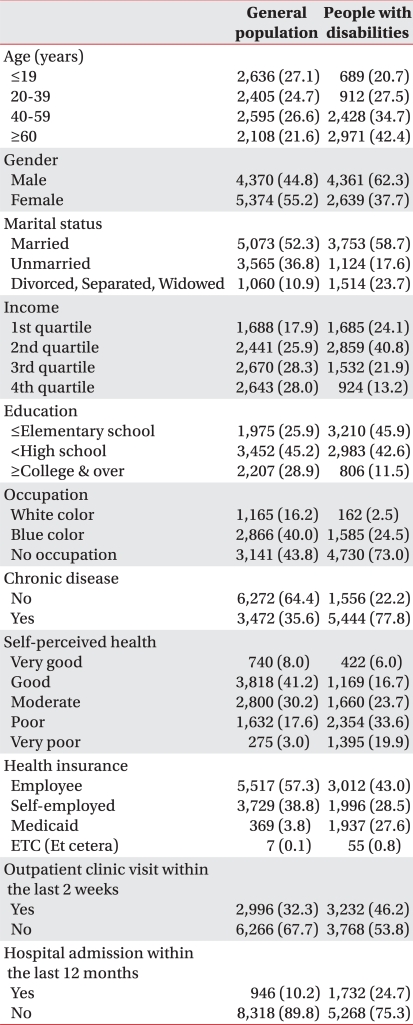
The average age of the respondents was older in the general population than in people with disabilities (38.4 versus 52.2 years). The proportion of males was higher in people with disabilities than in the general population (62.3 versus 44.8%). Income and educational status, which represented socioeconomic level, were lower in people with disabilities than in the general population. Also, the proportion of blue collar jobs or unemployment was higher in people with disabilities than in the general population. These results demonstrated the poor socioeconomic status of disabled people.
As for health insurance, the proportion of medicare was lower in the general population than in people with disabilities (3.8% versus 27.6%). The prevalence of chronic disease was lower in the general population than in people with disabilities (35.6% versus 77.8%). As for self-perceived health, the proportion of participants who reported "good" was the highest in the general population (41.2%), while the proportion of participants who reported "bad" was the highest in people with disabilities (33.6%) (Table 1). As for disability variables, physical disability occupied the highest percentage (11.8%), followed brain impairment (11.2%) and auditory impairment (9.3%). As reclassified by disability characteristics, external physical disability had the highest proportion (51.3%). Severe disability was found in 63.9% of people with disabilities (Table 2).
Demographic Characteristics of Study Subjects

Disability Characteristics According to the Korea Disability Act
Factors related to unmet healthcare needs
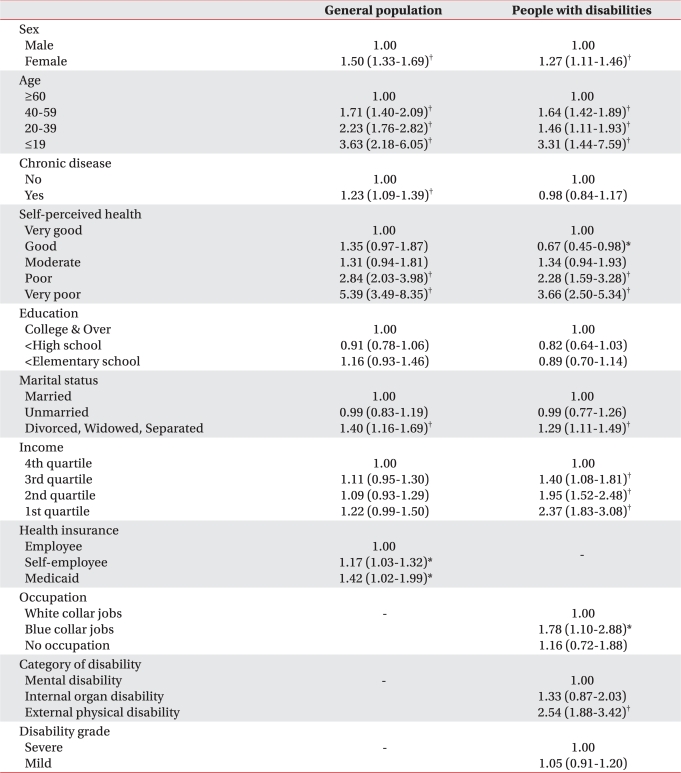
The proportion of unmet healthcare needs was not different between people with disabilities and the general population (22.1% versus 22.8%). By univariate analysis, unmet healthcare needs related to gender, age, chronic disease, education, marital status, income and occupation in people with disabilities, whereas those of general population correlated with gender, age, chronic disease, self-perceived health, education, marital status, income and health insurance. Then, we performed multivariate analysis using statistical significant variables as determined by univariate analysis. In people with disabilities, unmet healthcare needs significantly increased in terms of female gender, younger age, bad self-perceived health, no spouse, blue worker and external physical impairment. In contrast, unmet healthcare needs of the general population increased in cases of female gender, younger age, poor self-perceived health, no spouse, chronic disease and medicare, but the correlation between income and unmet healthcare needs was not statistically significant (Table 3).
Comparison of Factors Related to Unmet Healthcare Needs between the General Population and People with Disabilities
The reasons for unmet healthcare needs
In people with disabilities, the reasons for unmet healthcare needs were the lack of money (57.3%), mild symptoms (13.8%) and inaccessible transportation (12.8%) in decreasing order of frequency. In the general population, the reasons were no available time (30.2%), mild symptoms (23.8%) and the lack of money (20.9%) in decreasing order of frequency.
Unmet healthcare needs of physical and brain impairment
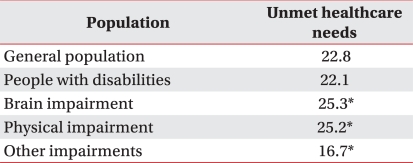
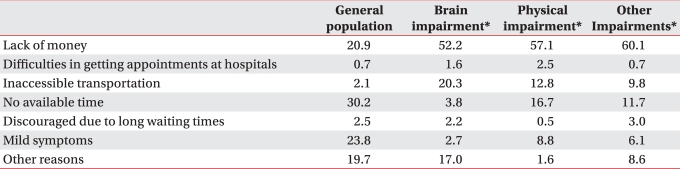
Unmet healthcare needs represented 25.3% in brain impairment and 25.2% in physical impairment cases, which were higher than in the general population (22.8%) and in the other impairments (16.7%) (Table 4). Economic reason was 52.1% of all reasons for unmet healthcare needs in brain impairment and 57.1% in physical impairment, which were different from 20.9% in the general population, but not significantly different from 60.1% in the other impairments. Inaccessible transportation was 20.3% of all reasons for unmet healthcare needs in brain impairment and 12.8% in physical impairment, which were different from 2.1% in the general population and 9.8% in the other impairments (Table 5).
The Amount of Unmet Healthcare
The Reasons of Unmet Healthcare Needs
DISCUSSION
In the past, people with disabilities only referred to somatic disability, but in recent years, the concept has been extended to people with significant limitations on the activities of daily and social lives.12 In Korea, while the registration criteria only included physical/visual/auditory impairment and mental retardation in the past, the criteria has been extended to include brain impairment, development delay, mental impairment, renal function impairment, heart function impairment, respiratory function impairment, liver function impairment, intestinal/urinary tract function impairment, epilepsy and facial deformities since 2000. In addition, with an increasing elderly population, acquired disabilities have increased. As a result, the number of registered disabled persons increased over 10 times (176.7 thousand in 1988 to 2,247 thousand in 2008).13
People with disabilities want general medical services, including health screening and rehabilitation for the treatment of current disabilities.14 In order to develop healthcare policies that prevent the occurrence of possible diseases and the progression of disabilities, it is necessary to evaluate appropriate healthcare services.15
In particular, identifying unmet healthcare needs is crucial to measure access to medical services, as well as the availability and acceptability of healthcare services.16 Unmet healthcare needs have 3 characteristics, such as availability, accessibility and acceptability. Availability is reduced when people do not receive medical services due to the lack of medical facilities or long waiting time. Accessibility can be determined by economic status and available transportation. Finally, acceptability can be lower in patients who are not interested in their health, and those who do not know which hospitals to visit or are dissatisfied with the quantity and quality of medical services.17
To identify problems with accessibility to medical services, questionnaire surveys are commonly used.18 It is advantageous to consider personal and social factors when demonstrating unmet healthcare needs that respondents perceived, compared to medical utilization alone. However, subjective assessment of unmet healthcare needs may have some limitations reflecting actual differences if socioeconomic levels are correlated with the differences in perceived treatment needs.19,20 Therefore, it is important to objectively estimate unmet healthcare needs in diseases. Generally, in terms of equity in healthcare utilization, objective indicators such as Le Grand index (HILG) and HIwv index have been used for measuring unmet healthcare needs.21,22 However, many studies using these indicators have difficulty in generalization because they have been limited to specific diseases.
In Korea, a previous study analyzed the factors related to unmet healthcare needs in the third KNHANES (2005) after defining unmet healthcare needs as events during the last 12 months where the participants could not receive medical services when they needed to see a doctor.10 Since 2000, some studies have consistently shown that although high-income participants receive unnecessary health care, low-income participants receive less medical services than they need.8 These results imply that the disparity of unmet healthcare needs differs depending on income levels.
However, in our study, there was no significant difference in unmet healthcare needs between people with disabilities and the general population. Unmet healthcare needs was higher in people with limitations of mobility, such as brain impairment and physical impairment, than one in the general population or other impairments. This is because mental retardation and autism, which were classified as other impairments, occurred in a higher percentage of the pediatric population, and their priority of social requirements was set for education and nursery. In mental impairment, which mostly occurred in people aged <60 years, the priority of social requirements was guaranteed income, whereas healthcare was the priority of social requirements in brain and physical impairments. There was no significant difference in the frequency of unmet healthcare needs between severe and mild grades of disabilities. This may be because economic factor, which was a main reason for unmet healthcare needs, was not always correlated with disability severity.
In addition, there was significant difference in the reasons for unmet healthcare needs between people with disabilities and the general population. People with disabilities showed environmental reasons, such as economic status and the limitations of transportation, whereas the general population showed personal reasons, such as no available time or mild symptoms. In the 2 groups of participants, unmet healthcare needs was correlated with gender, self-perceived health, marital status, income, occupation, health insurance and the presence of chronic disease, but economic status primarily influenced unmet healthcare needs in people with disabilities. However, self-perceived health had a significant impact on unmet healthcare needs in the general population.
People who had unmet healthcare needs due to economic factors showed more medical utilization and higher unmet healthcare needs. The main reason of unmet healthcare needs may be economic burdens from low payment. However, the reasons for unmet healthcare needs in the high-income participants were personal, such as mild symptoms and lack of time. In particular, people who visited outpatient clinics during the last 2 weeks showed higher unmet healthcare needs than those who did not. This shows limitations of our health insurance system, which ensures access to medical services but imposes high economical burdens on medical utilization.23 In addition, the older people became, the lower the frequency of unmet healthcare needs became. However, if they had unmet health needs, the main reason was economic deprivation. This indicates that although elderly people could have less limitation of time, they have lower accessibility due to the economic reason.
Our subjective survey could not demonstrate unmet healthcare needs in terms of specific diseases, symptoms and services.24 In addition, because the recognition and attitude of a patient have a significant influence on subjective healthcare needs, actual need assessed by the medical standard are mandatory to establish an effective policy.25 A possible explanation for this may be that it is difficult to make definite policies by general evaluation of unmet healthcare needs, whereas the assessment of unmet healthcare needs by healthcare professionals has the advantage of establishing countermeasures in clinical practice and other types of medical services. Therefore, we should develop objective methods for measuring unmet health care needs about general medical services, as well as specific medical services related to disabilities, such as rehabilitation and assistive devices.
In addition, because the 2008 Survey of Disabled People targeted only registered people with disabilities, unregistered disabled people were not evaluated in the study. However, the registration rate of people with disabilities has steadily increased due to the expansion of disability criteria and compensation of welfare services for the disabled. For this reason, it is conceivable that this survey may reflect the actual status of disabled persons.
CONCLUSION
This is the first study that compared unmet healthcare needs between the general population and people with disabilities in Korea. There was no significant difference in unmet healthcare needs between people with disabilities and the general population in Korea. However, subjects with brain and physical impairments had higher unmet healthcare needs. In addition, people with disabilities had more environmental reasons than the general population. Therefore, we should decrease unmet healthcare needs by making efforts to reduce economic and physical barriers.