Retrospective Assessment of the Implementation of Critical Pathway in Stroke Patients in a Single University Hospital
Article information
Abstract
Objective
To evaluate the effects of the implementation of critical pathway (CP) in stroke patients treated at a single university hospital.
Methods
A retrospective medical review collected data from 497 patients who had suffered acute stroke in the rehabilitation center. Stroke outcomes were compared between before and after the implementation of CP based on factors including demographic factors, stroke characteristics, pre-existing medical conditions, medical complications, functional states, and length of stay (LOS).
Results
After the implementation of CP, the patients showed significantly higher stage for upper proximal (p=0.008) and lower extremity (p=0.001) on Brunnstrom stage and significantly lower scores for modified Rankin Scale (p=0.003) at transfer. For those with pre-existing medical conditions, there were significantly increased osteoarthritis (p=0.002) and valvular heart disease (p=0.011). Regarding medical complications during acute inpatient rehabilitation, there were significantly decreased shoulder pain (p=0.001) and dysphagia (p=0.017), and significantly increased gastrointestinal symptoms (p=0.001). Functional gain and efficiency of stroke patients during rehabilitation center hospitalization did not significantly change after implementation of CP. But, shorter LOS of total hospitalization, pre-rehabilitation center hospitalization, and rehabilitation center hospitalization were evident.
Conclusion
After the implementation of CP, patients less often developed complications and displayed no changes in functional gain and efficiency. They had shorter LOS of total hospitalization, pre-rehabilitation center hospitalization and rehabilitation center hospitalization.
INTRODUCTION
Stroke is common in Korea. Stroke may cause serious disabilities. With the Westernization of the Korean lifestyle, the prevalence of stroke is increasing and has become the second cause of death in the nation [1]. Complications during the post-stroke rehabilitation period delay patients' recovery and impede their rehabilitation. To reduce these complications, a systematic and comprehensive treatment plan, such as a critical pathway (CP), is necessary [2,3,4,5].
CP refers to a systematic treatment plan created so that the medical personnel from different fields can sequentially apply efficient and appropriate treatment [6]. The introduction of CP for treatment of stroke dates back to the mid-1980s. The diverse CPs include patient management in the local community after discharge, and as well as acute stroke diagnosis and thrombolysis treatment [7]. In general, CP related to acute stroke is divided into three categories: treatment, rehabilitation, or both [7]. In the United States, 78% and 30% of hospitals have instituted a CP for the treatment of ischemic stroke and cerebral hemorrhage, respectively [8].
Although research thus far has reported that a CP prevents unnecessary treatment delay and decreases hospital stay [9,10,11], most studies were confined to patients experiencing a first-ever ischemic stroke. No study has detailed the changes in the occurrence of complications after CP introduction.
Unlike previous studies, this study was not confined to ischemic stroke patients. Hemorrhagic stroke patients and patients with a history of more than one stroke as well as those with the first onset of a stroke were included. The retrospective study involved patients who visited a single university hospital due to a stroke. The aim was to discern differences in the kinds of complications and their incidence during hospitalization, functional recovery, and the length of stay (LOS).
MATERIALS AND METHODS
Subjects
The subjects of this study were 497 patients who visited the emergency room of Gyeongsang National University Hospital for the first time without treatment in other hospitals after a stroke. The study included patients who were diagnosed with an ischemic or hemorrhagic stroke through brain computed tomography or magnetic resonance imaging based on their history or physical examination findings, transferred to the Department of Rehabilitation after acute-stage treatment and discharged after comprehensive rehabilitation treatment. With January 2010 (the time of implementation of CP) as the reference time point, subjects were divided into two groups. The first group comprised 196 patients who visited the hospital from July 1, 2007 to December 31, 2009, prior to CP introduction. The other group comprised 301 patients who visited the hospital from January 1, 2010 to June 31, 2010, after CP introduction. Both groups were subsequently transferred to the Department of Rehabilitation.
CP-mediated rehabilitation treatment of acute stroke patients involves a physical examination to evaluate the severity of stroke, functional state, and complications within 3 days after the onset of a stroke in collaborative diagnosis with the Department of Rehabilitation and by diligently and swiftly carrying out rehabilitation, thereby preventing and treating complications and enabling early movement of patients. During treatment, when a patient is neurologically stable, comprehensive rehabilitation treatment is provided and whether transfer to the Department of Rehabilitation is possible is evaluated. After transfer or discharge, a follow-up observation is made. When a stroke progresses during early rehabilitation treatment, the patient should be reevaluated and treatment appropriate for the patient's condition carried out (Fig. 1).
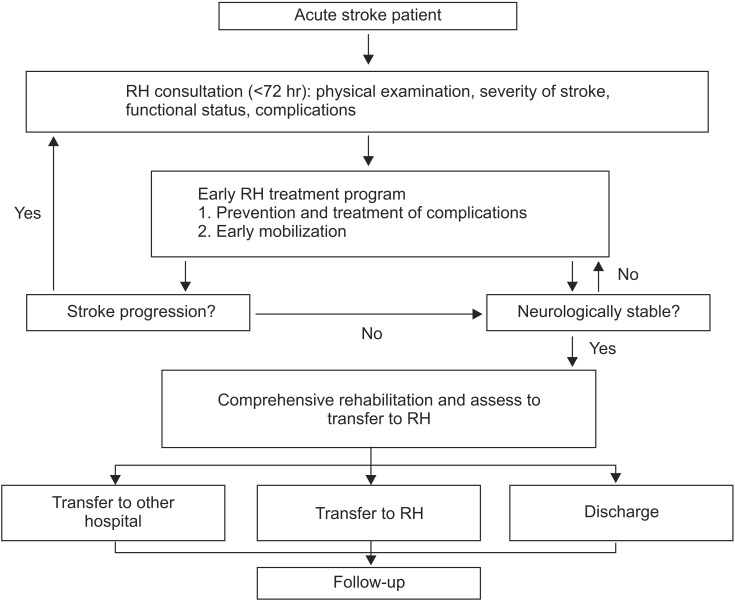
Critical pathway of comprehensive rehabilitation (RH) and transfer to Department of Rehabilitation.
Methods
Retrospective review of the medical records was conducted. Demographic and stroke characteristics prior to and after the introduction of CP including age, gender, cause of stroke (ischemic or hemorrhagic), stroke location (cortical, subcortical, or infratentorial lesions), and the hemiplegic side resulting from a stroke (right, left, or bilateral sides) were investigated and the National Institutes of Health Stroke Scale (NIHSS) was used to assess the patients' condition at the time of visit to the emergency room.
Patient history including previous stroke, hypertension, diabetes mellitus (DM), dyslipidemia, seizure, osteoarthritis, osteoporosis, alcohol abuse, smoking, chronic obstructive pulmonary disease or asthma, coronary artery disease, cardiac arrhythmia, valvular heart disease, renal failure, and hydrocephalus was investigated.
Concerning complications, the presence of shoulder pain after a stroke, seizure, depression, heterotopic ossification, decubitus ulcer, urinary tract infection, pneumonia, electrolyte imbalance, tracheostomy, Foley catheter insertion, hydrocephalus, dysphagia, deep vein thrombosis, gastrointestinal symptoms (gastritis, gastric ulcer, gastric bleeding, and enteritis), progression of a stroke, a fall, and sudden death was inspected.
For functional evaluation, stroke patients were classified as ischemic stroke patients and hemorrhagic stroke patients according to stroke cause and their modified Rankin Scale (mRS) and Brunnstrom stage were investigated by dividing their lesions into the upper limb proximal, upper limb distal, and lower limb at the time of transfer to the Department of Rehabilitation. At this time and at discharge, Korean version of Modified Barthel Index (K-MBI) score was assessed and functional acquisition (score at the time of discharge - score at the time of transference to the Department of Rehabilitation) was also investigated to examine efficiency of the rehabilitation treatment (functional acquisition/LOS) to examine the differences between the two groups.
In addition, to analyze the effects of the introduction of CP on the number of hospital stay days, the period of hospitalization until transfer to the Department of Rehabilitation, the period of hospitalization in the Department of Rehabilitation, and the entire period of hospitalization from when visiting the emergency room until discharge from the hospital were investigated.
Statistical analyses
Medical record data for the recent 5 years were used to assess the condition of patients who experienced ischemic or hemorrhagic stroke prior to and after the introduction of CP using independent t-test. Age, NIHSS, mRS, Brunnstrom stage, K-MBI, and LOS are reported as averages±standard deviations. Gender, cause of a stroke, location of brain lesion, hemiplegic side resulting from a stroke, pre-existing medical conditions, and complications occurred prior to discharge were compared using chi-square test. SPSS ver. 17.0 for Windows software (SPSS Inc., Chicago, IL, USA) was used for the analyses, with significance set at p<0.05.
RESULTS
Demographic and stroke characteristics
The total number of the subjects was 497. Among 196 patients prior to the introduction of critical pathway, 96 (49.0%) were male and 100 (51.0%) were female. Average age was 66.4±13.4 years. Among 301 patients after the introduction of CP, 153 (50.8%) were male and 148 (49.2%) were female. The average age was 64.1±12.6 years.
One hundred eleven (56.6%) patients experienced ischemic stroke and 85 (43.4%) experienced hemorrhagic stroke prior to the introduction of CP. The respective numbers following CP implementation were 132 (43.9%) and 169 (56.1%). Cortical, subcortical, and infratentorial lesions comprised 8 (4.1%), 55 (79.1%), and 33 (16.8%) patients, respectively, prior to CP introduction and 15 (5.0%), 242 (80.4%), and 44 (14.6%) patients, respectively, after the introduction of CP. Right hemiplegia, left hemiplegia, and bilateral hemiplegia comprised 78 (39.8%), 80 (40.8%), and 38 (19.4%) patients, respectively, prior to CP and 124 (41.2%), 123 (40.9%), and 54 (17.9%) patients, respectively, after CP implementation. NIHSS measured to evaluate patient conditions at the time of the emergency room visit was 9.1±4.2 and 9.6±5.9 prior to and following the introduction of CP, respectively. There were no significant differences between the two groups (Table 1).
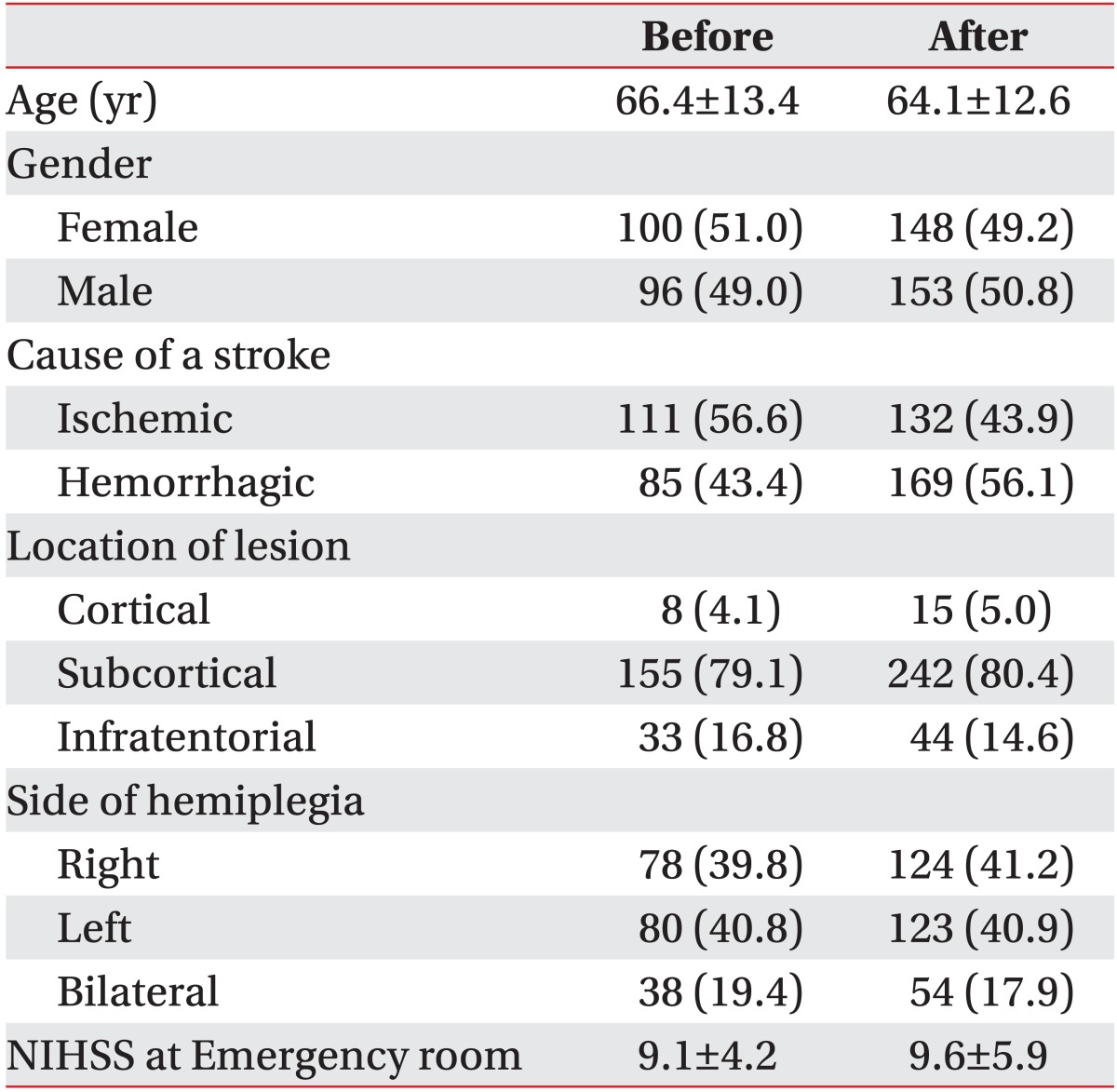
Comparison of demographic and stroke characteristics before and after CP implementation
Pre-existing medical conditions
Pre-existing medical conditions included hypertension (n=132, 67.3%), DM (n=47, 24.0%), alcohol abuse (n=47, 24.0%), osteoarthritis (n=46, 23.5%), smoking (n=40, 20.4%), and previous stroke (n=35, 17.9%), prior to the introduction of CP. Following CP implementation, pre-existing medical conditions included hypertension (n=215, 71.4%), osteoarthritis (n=110, 36.5%), alcohol abuse (n=81, 26.9%), smoking (n=79, 26.2%), DM (n=70, 23.3%), and previous stroke (n=58, 19.3%). The increased rate of osteoarthritis and valvular heart disease with the implementation of CP was significant (p=0.002 and p=0.011, respectively). There were no other significant differences (Table 2).
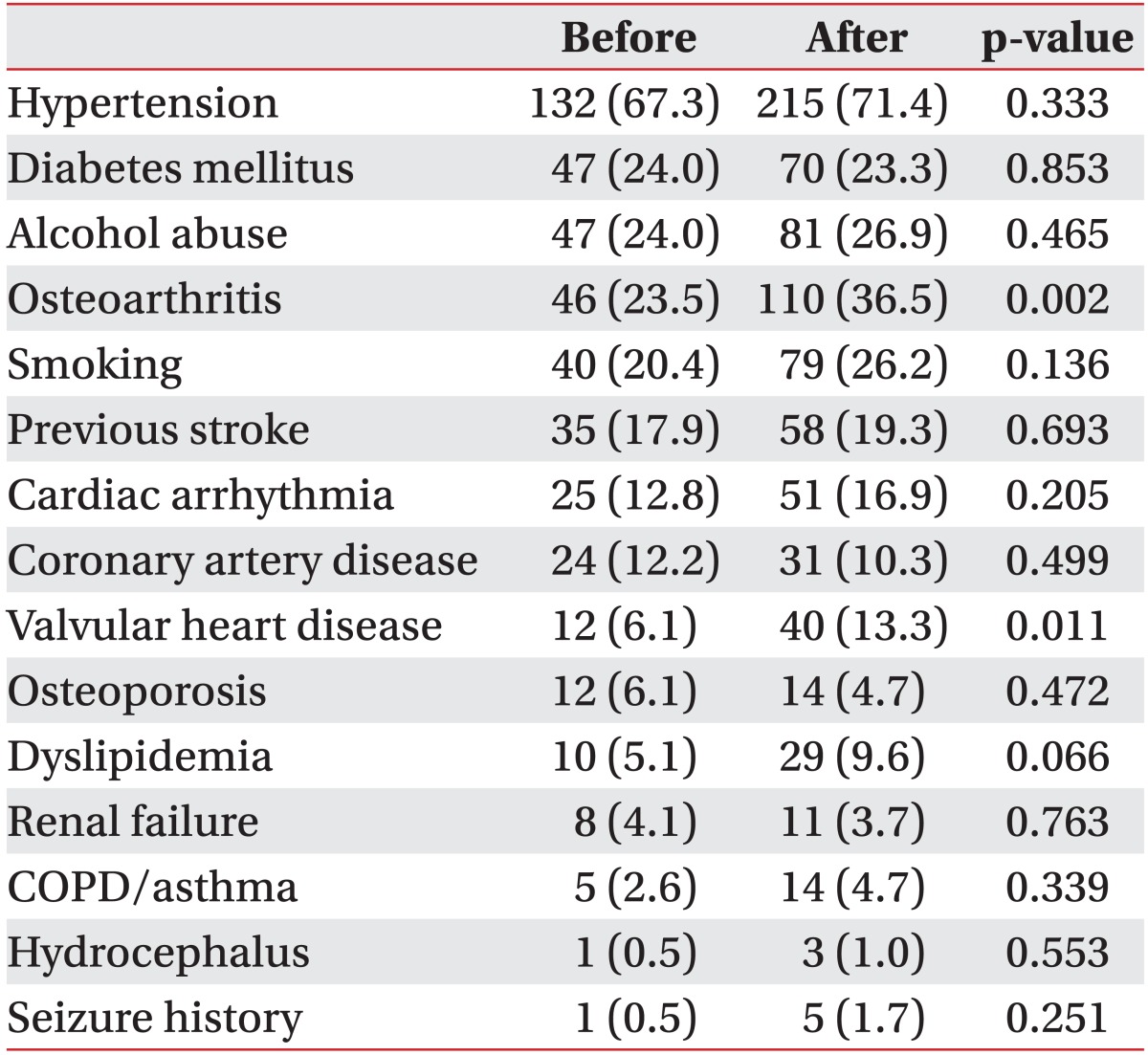
Comparison of pre-existing medical conditions of stroke patients before and after CP implementation
Complications
More than half the patients suffered from shoulder pain after a stroke (n=124, 63.3%) and dysphagia (n=121, 61.7%) prior to CP, followed by Foley catheter insertion (n=35, 17.9%), urinary tract infection (n=30, 15.3%), and pneumonia (n=28, 14.3%). After CP introduction, dysphagia comprised the majority of complications (n=153, 50.8%), followed by shoulder pain after a stroke (n=145, 48.2%), gastrointestinal symptoms (n=50, 16.6%), depression (n=49, 16.3%), and Foley catheter insertion (n=47, 15.6%). The decreases in the rate of shoulder pain after stroke and dysphagia was significant (p=0.001 and p=0.017, respectively), with the increase in gastrointestinal symptoms being significant (p=0.001). Among all stroke patients, 181 (92.3%) and 262 (87.3%) experienced complications before and after implementation of CP, respectively (Table 3).
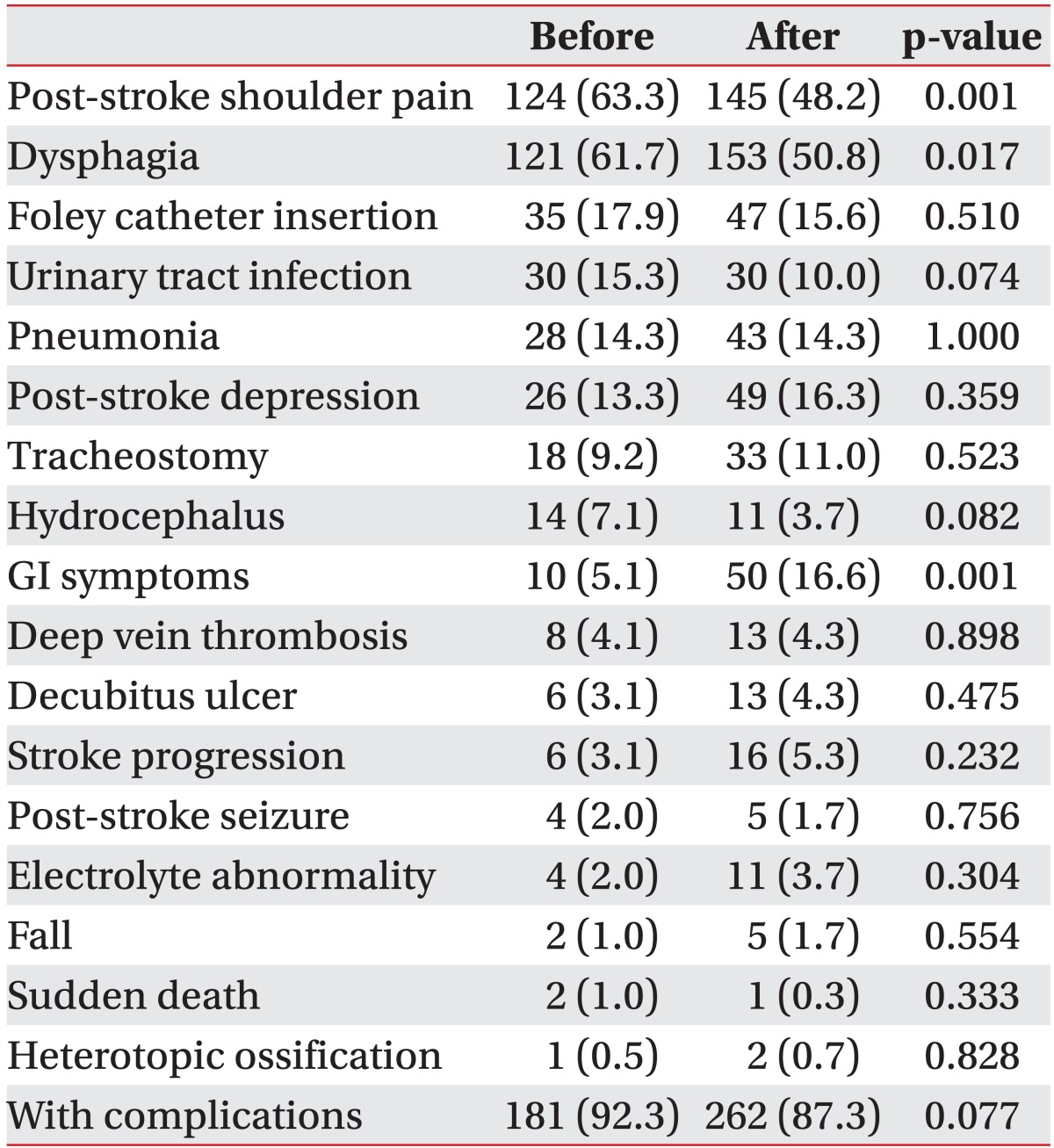
Comparison of the number of stroke patients with medical complications before and after CP implementation
Functional evaluation
After transfer, mRS score was 4.4±0.9 and 4.2±0.8 prior to and after CP introduction, respectively (p=0.003). Upper limb proximal, upper limb distal, and lower limb Brunnstrom stage was 3.2±1.3, 3.2±1.5, and 3.2±1.1, respectively, prior to the introduction of CP and 3.5±1.3, 3.4±1.4, and 3.6±1.2, respectively, after CP introduction. The increase in upper limb proximal and lower limb Brunnstrom stage was significant (p=0.008 and p=0.001, respectively). mRS of ischemic stroke patients was 4.4±1.0 and 4.1±0.8 prior to and following CP introduction (p=0.005). Brunnstrom stage increased significantly in upper limb proximal, upper limb distal, and lower limb (p=0.001, p=0.017, and p=0.01, respectively). On the contrary, changes in mRS and Brunnstrom stage in all the three locales of hemorrhagic stroke patients were not significant. For all stroke patients, K-MBI significantly decreased when they were transferred and discharged after the introduction of CP (p=0.004 and p=0.016, respectively). However, functional acquisition and rehabilitation treatment efficiency in K-MBI was not statistically different (Table 4).
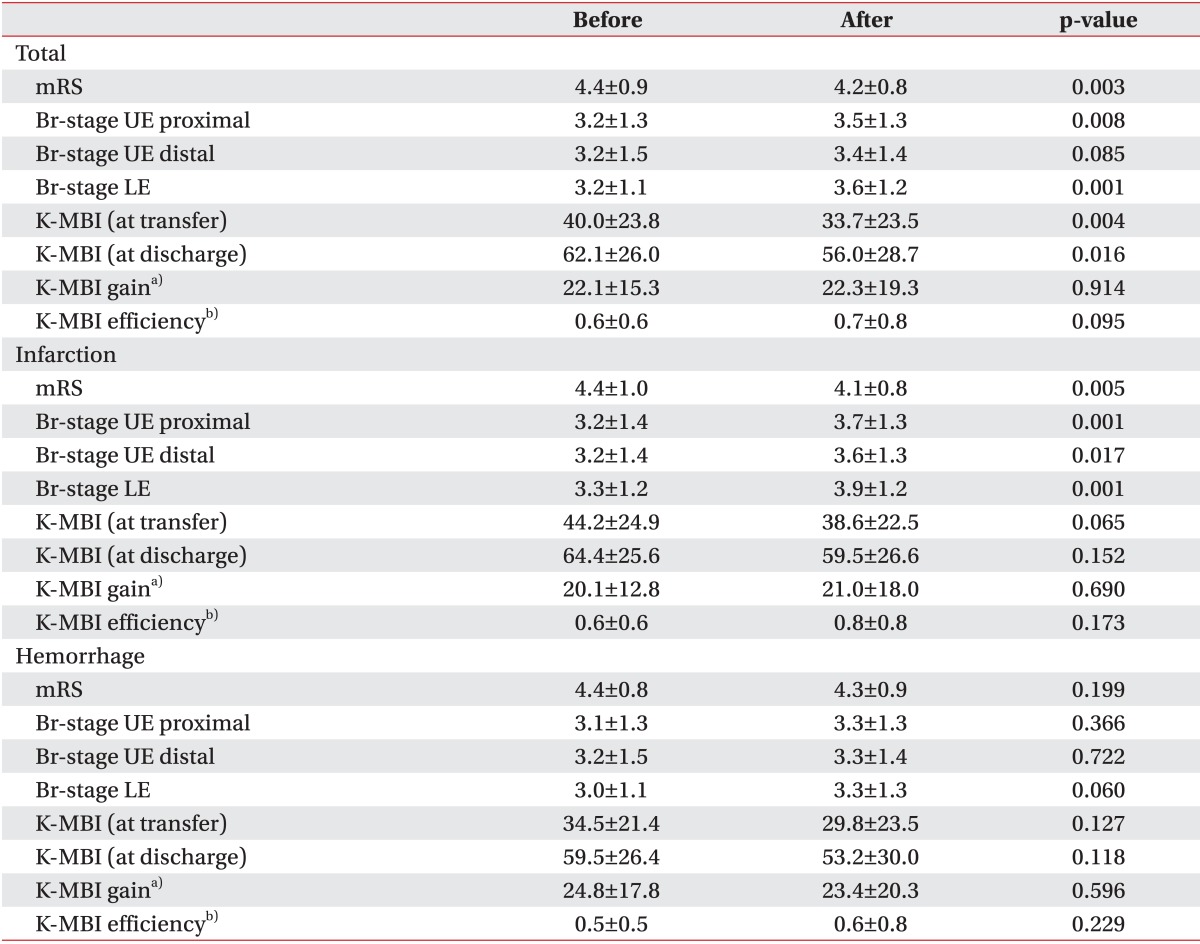
Comparison of functional states at transfer to rehabilitation center and discharge before and after CP implementation
Length of stay
LOS after CP introduction until transfer to the Department of Rehabilitation, LOS in the Department of Rehabilitation, and the total LOS significantly decreased in all stroke patients and the ischemic and hemorrhagic stroke patient groups (Table 5).
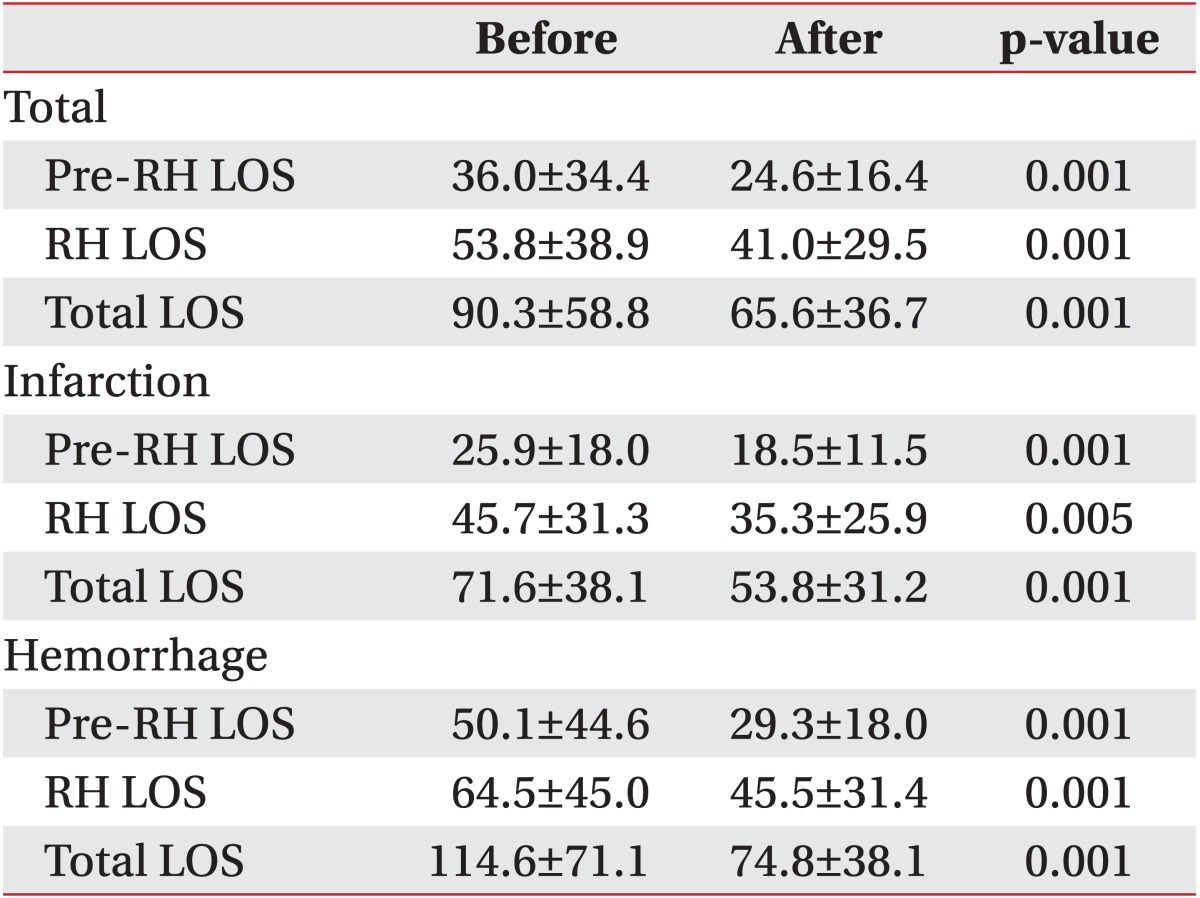
Comparison of length of stay (LOS) before and after CP implementation
DISCUSSION
CP can prevent unnecessary treatment delay and can shortened hospital stay [9,10,11]. Attention to the introduction of stroke CP and the resulting effects is increasing. However, its effects have not been systematically established and only small scale studies have been done. The present study was undertaken to reveal differences in the incidence of complications, functional recovery, and LOS of stroke patients prior to and after CP introduction, with differences among stroke patients classified according to the cause of stroke, with stroke patients in a single hospital as subjects.
The rates of hypertension, osteoarthritis, alcohol abuse, smoking, and DM were high prior to and after the introduction of CP. This agrees with the findings of a prior study, in which hypertension, DM, smoking, and previous cardiovascular disease were the most common risk factors for stroke [12]. Presently, osteoarthritis and valvular heart disease significantly increased in stroke patients after CP introduction, compared to before CP introduction. A previous study reported that the diagnosis frequency of diseases significantly differed according to the treatment environment of a stroke [13]. The present study was retrospective and the results depended on medical records, so the results may have varied according to the integrity of preparation of medical records. Also, the results may reflect the increasing use of radiologic examination for active diagnosis of stroke, and increasing use of cardiac sonography among stroke patients.
Gain and efficiency in Functional Independence Measure scale and MBI are significantly low when a stroke is accompanied by osteoarthritis, myocardial infarction, and atrial fibrillation [14]. Such past medical histories can impede recovery during hospitalization (including rehabilitation) of stroke patients. The treatment plan should consider such factors.
The rate of complications in stroke patients did not differ between the two groups, but tended to decline after the introduction of CP. The most frequent complications of post-stroke dysphagia and shoulder pain significantly decreased. Dysphagia is diagnosed by performing esophagography or a videofluoroscopic swallowing study on patients suspected of difficulty in swallowing using a bedside screening test. According to the treatment plan, they are trained to swallow and a follow-up examination is done to check improvement. Early evaluation and treatment of dysphagia after CP introduction aids in the treatment of dysphagia and can help prevent complications. Shoulder pain after a stroke includes all musculoskeletal pains together with complex regional pain syndrome. After CP introduction, collaborative diagnosis with the Department of Rehabilitation was made early after the onset of a stroke. Also, before transfer to the Department of Rehabilitation, shoulder joint exercise was performed with bed posture and arm sling to prevent subluxation of the shoulder joints. This may have led to a reduction in the incidence of shoulder pain. Brunnstrom stage also significantly improved in proximal upper limb at the time of transfer, thereby preventing shoulder pain. This is consistent with a finding of a previous meta-analysis, in which early rehabilitation treatment was more effective in helping to obtain functional independence and decreasing complications than conventional rehabilitation treatment [15,16].
Gastrointestinal symptoms rapidly increased after CP introduction. Such patients were endoscopically diagnosed with the symptoms among those suspected of gastritis, gastric ulcer, and gastrorrhagia during hospitalization. Endoscopy has become a more commonly used procedure according to gastrointestinal complaints. When the NIHSS is high, gastrointestinal bleeding increases [17]. In the present study as well, after CP introduction the NIHSS measured when patients visited the emergency room became higher.
Functional evaluation following transfer to the Department of Rehabilitation and CP introduction revealed significantly lower mRS in ischemic stroke patients than hemorrhagic stroke patients. This result may reflect improved diagnosis and treatment of acute stroke patients because of CP, and because collaborative diagnosis with the Department of Rehabilitation enabled early comprehensive rehabilitation treatment even before transfer. Brunnstrom stage of ischemic stroke patients significantly increased when they were transferred and Brunnstrom stage of the upper limb proximal and the lower limb was significantly high in all stroke patients, which is the result of early rehabilitation treatment. Nonetheless, there were no significant differences in mRS and Brunnstrom stage of hemorrhagic stroke patients probably because they did not receive active rehabilitation treatment and had limited access to comprehensive rehabilitation due to postoperative treatment in the intensive care unit. Nevertheless, the mRS score of hemorrhagic stroke patients tended to be low and their Brunnstrom stage tended to be higher after CP introduction. It is likely that there will be positive effect of early rehabilitation treatment in hemorrhagic stroke patients after the CP introduction.
K-MBI of all stroke patients was significantly low compared to prior to the CP introduction, but other changes were not significant. On the other hand, LOS after CP introduction was significantly decreased in ischemic and hemorrhagic stroke patients, and all stroke patients. This indicates that functional acquisition and efficiency during comprehensive rehabilitation may be affected by differences in the total amount of treatment; significant reduction in LOS in the Department of Rehabilitation may influence the functional outcome of patients when they are discharged. This result is consistent with the outcome in which the hospitalization period decreased and the degree of independence was low in patients to which the CP was applied in previous meta-analyses [7,10,18]. In addition, after CP introduction, LOS significantly decreased in all total stroke patients. But, the fact that the efficiency of rehabilitation treatment was high and statistically significant in functional acquisition may indicate that the result of patient treatment did not differ appreciably among individuals.
This study concerned stroke patients hospitalized in a single hospital during the most recent 5 years, and included recurrent stroke patients as well as those who experienced a stroke for the first time. It was a large-scale study of all stroke patients in a single hospital and its advantage is that it examined complications, functional acquisition, and hospitalization period prior to and after CP introduction. However, this study was retrospective, involved one site, and depended on medical records and, therefore, the integrity of the preparation of these records, the stroke treatment environment at the time of data acquisition, and universalization of tests on relevant diseases that may have led to different results. In addition, there may be variation between hospitals concerning considering comprehensive rehabilitation treatment and patient transfer to the Department of Rehabilitation and their total hospital stay. The scope of available data from different hospitals applying the CP and from our hospital may differ, limiting generalization of the findings. Thus, multi-institutional research is necessary using data from hospitals that currently apply the stroke CP.
In conclusion, due to the introduction of the CP, the rate of complications among stroke patients tended to decline. Overall functional acquisition and efficiency did not differ between the periods before and after CP implementation. However, CP introduction reduced the hospitalization period before transfer to the Department of Rehabilitation, post-transfer LOS, and total LOS.
Notes
No potential conflict of interest relevant to this article was reported.