Effectiveness of Community-Based Rehabilitation (CBR) Centers for Improving Physical Fitness for Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis
Article information

Abstract
To synthesise the best available evidence for the effectiveness of interventions delivered in community-based rehabilitation (CBR) centers on physical fitness, for community-dwelling older adults living in Asian countries. This study is a systematic review and meta-analysis. Seven English and two Chinese electronic databases were searched for randomised controlled trials (RCTs) and quasi-experimental studies that were conducted by centers providing CBR. Independent reviewers screened, quality-appraised and extracted data. The primary outcome was physical fitness measured by validated assessment tools, including the Timed Up and Go Test (TUG) gait speed, hand grip strength, Functional Reach Test (FRT), and one-leg standing test. Assessments of activity of daily living and quality of life using tools including the Barthel Index, Short Form (SF)-12, and SF-36 were secondary outcomes. After screening 5,272 studies, 29 studies were included (16 RCTs, 13 quasi-experimental studies) from four countries. Meta-analyses found that CBR programs significantly decreased TUG time (mean difference [MD], -1.89 seconds; 95% confidence interval [95% CI], -2.84 to -0.94; I2=0%; Z=3.90, p<0.0001), improved gait speed (MD, 0.10 m/s; 95% CI, 0.01–0.18; I2=0%; Z=2.26, p=0.02), and increased one-leg standing time (MD, 2.81 seconds; 95% CI, 0.41–5.22; I2=0%; Z=2.29, p=0.02). Handgrip strength and FRT showed no statistically significant improvement in the meta-analyses. CBR may improve aspects of physical fitness for older adults in Asian countries. However, variability in intervention components and measurement tools reduced the ability to pool individual studies. Further trials are required with robust designs including standardised measures of physical fitness.

INTRODUCTION
The global population is ageing, with the proportion of older adults (aged 60 years or over) increasing in nearly every country [1]. Managing this change has been identified as a major public health issue in many countries, especially in Asian countries [2]. The United Nations Economic and Social Commission for Asia and the Pacific estimates that the proportion of older adults in Asian countries will increase from 12.4% in 2018 to 25% (1.3 billion) in 2050 [3]. This social phenomenon in Asian countries creates significant challenges for health, economic and social services [4,5].
Taking modifiable (smoking, dietary, and exercise behaviors) and non-modifiable (ageing processes) risk factors together, the prevalence of chronic diseases increases with age [6]. The increasing incidence of chronic diseases, including cardiovascular, neurodegenerative, and metabolic diseases, is associated with a decline in functional ability of older adults [7-9]. Functional ability is defined as “having the capabilities that enable all people to be and do what they have reason to value” and includes basic activities of daily living (ADLs) such as dressing, toileting, and ambulating [10]. Physical fitness is considered an essential component of functional ability and refers to all movement including during leisure or work time [11]. Impaired physical fitness is associated with loss of independence, reduced ability to perform ADL, reduced quality of life and increased mortality [12,13]. Therefore, older adults should be encouraged to maintain and improve their physical fitness to avoid associated loss of functional ability and independence [14]. Rehabilitation interventions, including exercises, occupational therapy, education, and group training, effectively improve physical fitness and performance of ADL of community-dwelling older adults [15,16]. Concurrently, there is established level one evidence that exercise reduces fall rates, improves endurance, range of motion, muscle strength, balance, mental health, functional ability, and health-related quality of life (HRQoL) in older adult populations [17-23]. Hence, effective interventions implemented by health systems that maintaining the physical fitness, functional ability, and reduce rising pressure on health care costs of older adults are important in the context of the ageing population [4,24,25].
Rehabilitation is provided by general or rehabilitation hospitals throughout China for individuals with new or chronic disabilities. However, only approximately 1% of older adults have access to timely, comprehensive rehabilitation services in their community [26]. To adequately meet the need for rehabilitation services including services for older adults, World Health Organization (WHO) guidelines recommend community-based rehabilitation (CBR) [27,28]. This focus on CBR aims to improve HRQoL for individuals living with disabilities and prevent new disability. CBR utilizes local community resources to deliver a broad range of rehabilitation programs, which are provided by healthcare professionals [29,30]. Previous research has demonstrated that CBR has a positive impact on health and social outcomes in developed Asian countries [31]. However, limitations and barriers to implementing CBR in developing Asian countries have also been described, such as lack of guidelines, insufficient local medical resources, shortages of health care professionals and limited programs being delivered by multidisciplinary teams [32,33].
A systematic review reported that CBR can help to improve both mental and physical function for individuals living with disabilities and improve their HRQoL, however, this review did not use aged-based inclusion criteria [29]. The quality of randomised controlled trial (RCT) that have evaluated providing CBR for ageing populations are relatively low due to small sample sizes, and limited reporting on intervention duration [34-36]. A preliminary search of both the literature and PROSPERO identified no systematic reviews that have evaluated the effectiveness of CBR for improving physical fitness or ADL for community-dwelling older adults, or specifically for older adults in Asian countries [37]. Different countries and regions have different cultures and histories, which may influence the effectiveness of CBR in older adult populations and implementation of CBR may differ in developed regions compared to developing regions of the world. Therefore, the objective of this systematic review was to synthesize the best available evidence for the effectiveness of interventions performed in CBR centers on physical fitness, ADL and HRQoL for older adults living in Asian countries. Findings aimed to inform the ongoing development of CBR in Asia counties and may be useful for other developing countries.
METHODS
This review was undertaken according to a published protocol [38] and reported following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary Table S1) [39]. The review was prospectively registered on PROSPERO (CRD42021292088).
Search strategy
Advice on the search and data sources was provided by a senior health sciences librarian. A three-step search strategy was used that included electronic and manual searches to ensure all published and unpublished literature in English and Chinese was located for the reviews [40]. Preliminary web searches through PubMed, CINAHL and Google Scholar using MeSH terminology [41] aimed to identify similar systematic reviews and relevant keywords. Then, a full text search with identified keywords using seven English electronic databases (CINAHL, MEDLINE, Scopus, ProQuest, Embase and Cochrane Library, and Web of Science), two Chinese electronic databases (China National Knowledge Internet and Wanfang Database) and grey literature (OpenGrey) from inception dates to 1st January 2022 was completed. Searches were re-run on 1st March 2023 to identify any new articles that were eligible for inclusion in the review. Finally, a manual search of the reference lists of all identified publications, including any systematic reviews, was undertaken to identify any additional studies. An example of a search strategy performed on MEDLINE can be found in Supplementary Table S2.
Inclusion and exclusion criteria
Two independent reviewers (WX and JU for English studies, WX and DX for Chinese studies) screened the titles and abstracts of all identified studies. Studies were included if: participants were community-dwelling adults aged 60 years or over living in 48 Asian countries (including Central, Northern, South-Eastern, Western, and Far East) (https://www.ncbi.nlm.nih.gov/mesh/68001208); interventions were programs conducted by centers providing CBR (including physiotherapy, exercise training, exercise, occupational therapy, Chinese traditional therapy, education, and medical services). Studies that evaluated palliative care, rehabilitation in the home or interventions delivered by hospitals, individual community medical practitioners or home visiting nurses were excluded; comparators could be usual or standard care or another intervention such as providing the control group with educational material. Study designs included were RCT and quasi-experimental trials. Case control studies, observational cohort studies, protocols, conference abstracts, qualitative studies, and reviews were excluded. Quasi-experimental studies were included as a source of further evidence [42]. Healthcare interventions may often be evaluated using quasi-experimental studies and preliminary searches had indicated that there were limited numbers of RCT published that addressed the topic within the geographical region of interest. The Cochrane handbook suggests that, if including non-randomized studies, attention is paid to the study design and addressing risk of bias (ROB) [42]. Quasi-experimental studies were only included if the design included the use of a control group and the ROB of any included quasi-experimental studies was subsequently addressed by using an appraisal tool specific to quasi-experimental studies [43].
Data extraction and analysis
The primary outcome was physical fitness including Timed Up and Go Test (TUG) [44], gait speed [45], handgrip strength [46], Functional Reach Test (FRT) [47], and one-leg standing test [48]. The TUG measures an individual’s ability to balance, sit to stand and walk [44]. Gait speed (the speed at which an individual walks) can be influenced by a number of factors, both voluntary and involuntary, and marks a functional skill that underpins a majority of the tasks that are essential to a person’s ability to function on a daily basis [45]. Grip strength is a measure of muscular strength or the maximum force/tension generated by one’s forearm muscles which is a screening tool for the measurement of upper body strength and overall strength [46]. FRT aims to measure dynamic balance using one simple task of reaching forward in a standing position [47]. The one-leg standing test is used to assess static postural and balance control [48].
The secondary outcomes were performance of ADL and HRQoL [49,50]. Studies were only included if they measured physical fitness outcomes using validated assessment tools, that included the Barthel Index (BI) [51] and the Short Form (SF)-12 [52] and SF-36 [53].
Joanna Briggs Institute (JBI) critical appraisal tools for RCT and quasi-experimental trials [40] were utilized for assessing the methodological quality of all included studies by two independent reviewers (DX and WX for Chinese articles and AMH and WX for English articles). Any disagreement between the two reviewers was resolved through discussion by all three researchers to reach a consensus.
The standardized data extraction tool from the JBI reviewer’s manual was utilized for quantitative data extraction, including publication date, country, participants’ baseline characteristics, study setting, methods, type, intensity, and duration of the CBR intervention and data measuring outcomes relevant to physical fitness, ADL and HRQoL [40]. Data extraction was conducted by two independent reviewers (WX and JU) to ensure the accuracy of all the extracted data.
Statistical analysis and data synthesis
All data were subjected to double data entry. The mean and standard deviation of post-intervention quantitative outcome data of the included studies was used for performing meta-analyses [42]. However, studies with baseline differences between the control group and intervention group were omitted from these analyses. Data were entered into Review Manager 5 statistical software and described graphically using forest plots [54]. Study data reported in non-parametric format (median, range or inter-quartile range) or as standard errors were converted to means and standard deviations [55]. I2-statistics and visual inspection of forest plots were used to assess heterogeneity which was rated as low (25%), moderate (50%) or high (75%) [56]. Sensitivity analyses were performed when high heterogeneity (>75%) occurred. Random effects models were used to calculate effect sizes if there was substantial heterogeneity (I2>50%); otherwise, a fixed-effects model was used [56]. Treatment effect results were presented as mean difference (MD) with 95% confidence interval (95% CI). Studies unable to be pooled into meta-analysis were reported narratively using tables [57].
We used the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) system, recommended by Cochrane, to determine the certainty of evidence for the primary outcome of physical fitness, and presented results in a summary of findings table. The GRADE system categorizes the certainty of the evidence as very low, low, moderate, or high by rating the evidence through consideration of five domains: ROB, inconsistency of results, indirectness, imprecision, and publication bias [58]. The within-study ROB was downgraded by one level if 25% or more of the participants in the comparisons were from included studies with high ROB. The inconsistency of results was assessed by considering heterogeneity of point estimates, 95% CIs, and statistical measures, and was downgraded by one level if there was a wide variation of effect estimates or the I2 statistic was greater than 50%. In terms of indirectness, the quality of evidence was downgraded by one level if more than 50% of participants differed to the target population. We downgraded the quality of evidence by one level for imprecision if the sample size was less than 400 participants and downgraded two levels if the sample size was less than 200 participants. Due to the small sample sizes and limited numbers of studies we downgraded one level for suspicion of publication bias.
RESULTS
Literature search and study selection
The screening and selection of studies included in the review is presented in Supplementary Fig. S1. A total of 5,272 studies were identified through database searches and after final screening, 29 studies met the inclusion criteria. Studies excluded after full text review are summarized in Supplementary Table S3 with reasons for exclusion. Eight English studies [31,59-65] were included in meta-analyses. Twenty-one studies (14 English studies [62,66-78] and seven Chinese studies [34-36,79-82]) were narratively synthesized due to unique outcomes evaluated, or active interventions being delivered to the control groups. The seven Chinese studies [34-36,79-82] included in the narrative synthesis were of very low quality and the outcomes data were unable to be extracted due to absence of information about the mode, frequency and intensity of interventions that were evaluated.
Study characteristics
The characteristics of the included studies are presented in Table 1. One study was conducted in Israel [67], four in Korea [60,62,70,78], four in Japan [31,61,66,69], and 20 in China [34-36,59,63-65,68,72,73,75-77,79-81,83-86]. There were 16 RCTs [34-36,62,67-70,74,76-81,86], and 13 quasi-experimental studies [31,59-61,63-66,72,73,75,82,83]. The mean sample size of all included studies was n=198 and the mean age of all participants was 71.65±6.34 years. Nine studies [34-36,67,68,70,73,81,82] recruited older adults with stroke, three studies [65,79,80] recruited older adults with pulmonary dysfunction, four studies [62,63,66,71] older adults with knee pain, and 13 studies [31,59-61,64,69,72,74,75-78,83] included participants with other health conditions, including frailty, functional disability, and heart disease. Of the CBR interventions provided, all 29 studies delivered exercises, 13 studies provided education [34-36,63,65,67,68,77,79-81,83,85], and four studies provided counselling [34,63,68,84]. Eighteen studies [31,34-36,59-61,63,67-69,71,72,75,78-80,85] compared CBR with usual care, five studies [62,66,73,74,83] compared a new CBR intervention with standard CBR medical care or placebo intervention, five studies [64,65,70,76,86] compared CBR with home-based rehabilitation, and two studies [77,81] compared CBR with health education.
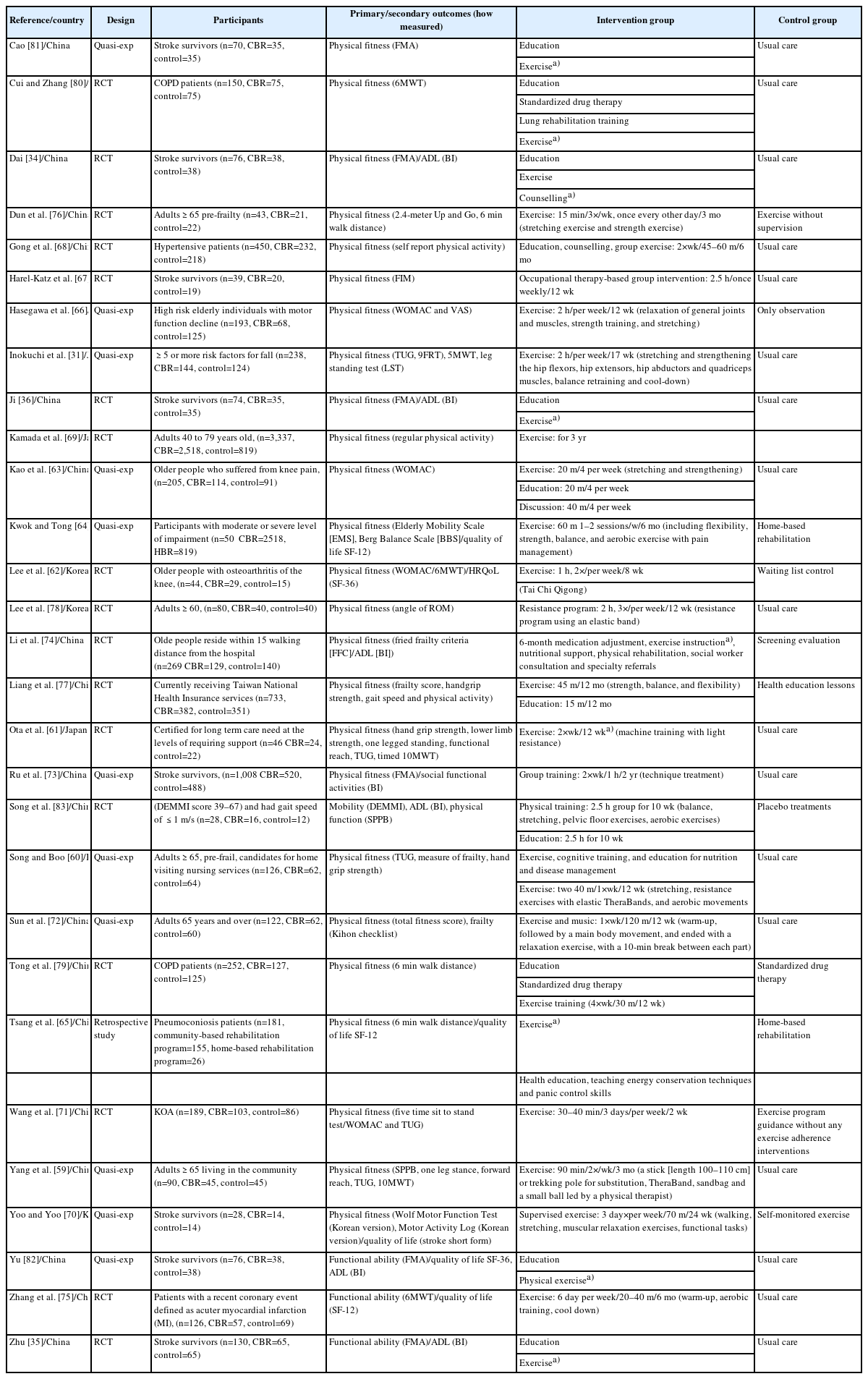
Characteristics of included studies
Methodological quality appraisal
The methodological quality rating of the included studies (both RCT and quasi-experimental studies) is presented in Supplementary Tables S4, S5 and summarized in Supplementary Figs. S2-S5. Overall, the ROB for items including random sequence generation and reporting bias was considered low for the included RCT. The ROB due to participants not being blinded to the intervention was rated as high for 14 studies. Six quasi-experimental studies were judged to be of low quality due to inappropriate statistical analyses. The certainty of evidence for the primary outcome of physical fitness measured by GRADE system is presented in Table 2.

Summary of findings of GRADE: the effectiveness of CBR on physical fitness
Effectiveness of interventions
Primary outcome – physical fitness
Physical fitness was measured by 31 different assessment tools. Seventeen assessments tools were used by more than two studies, and five of these assessment tools: TUG [31,59-61,66,76], gait speed [31,59,61,62], handgrip strength [31,60,61,87], FRT [31,59,61], and one-leg standing time [31,59,61] were pooled in meta-analysis. Findings from five studies that assessed motor function of older adults with stroke, using the Fugl-Meyer motor function assessment [34-36,81,82] were presented as an un-pooled forest plot. Findings from the remaining studies were narratively synthesized in Supplementary Table S6.
TUG
Six studies [31,59-61,66,76] evaluated the effectiveness of a CBR program (exercise, including both strength and balance training) on physical fitness using the TUG. Four studies were included in the meta-analysis (493 participants) [31,59-61]. Results demonstrated that older adults receiving CBR exercise programs made significant improvement in the TUG compared to usual care (MD, -1.89 seconds; 95% CI, -2.84 to -0.94; I2=0%; Z=3.90, p <0.0001), with no statistical heterogeneity found (Fig. 1).
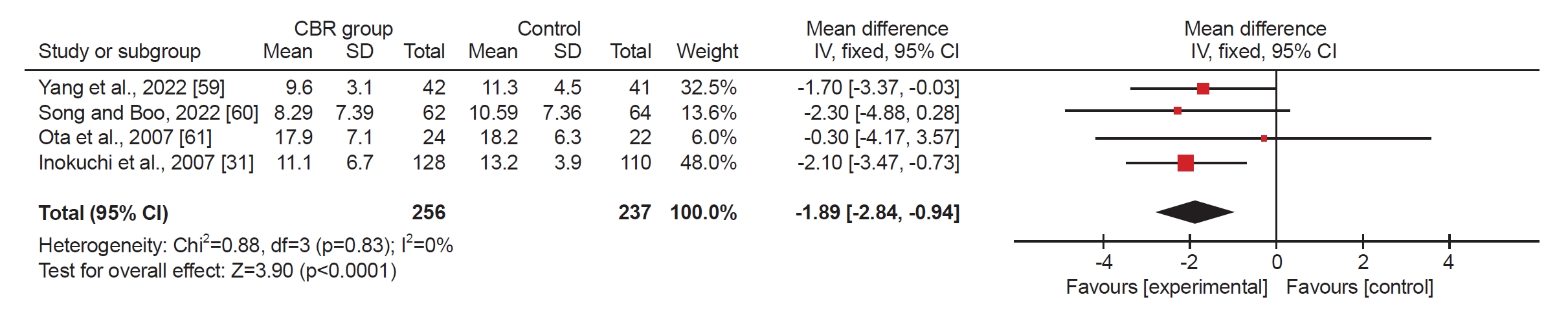
Effects of CBR program on TUG. Values are in second. CBR, community-based rehabilitation; TUG, Timed Up and Go Test; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Gait speed
Six studies [31,59,61,62,66,77] evaluated the effectiveness of a CBR program (exercise) on gait speed and four studies [31,59,61,62] were pooled in meta-analysis (n=397 participants), and no statistical heterogeneity was found. A statistically significant difference was found between the two groups (MD, 0.10 m/s; 95% CI, 0.01–0.18; I2=0%; Z=2.26, p=0.02; Fig. 2).
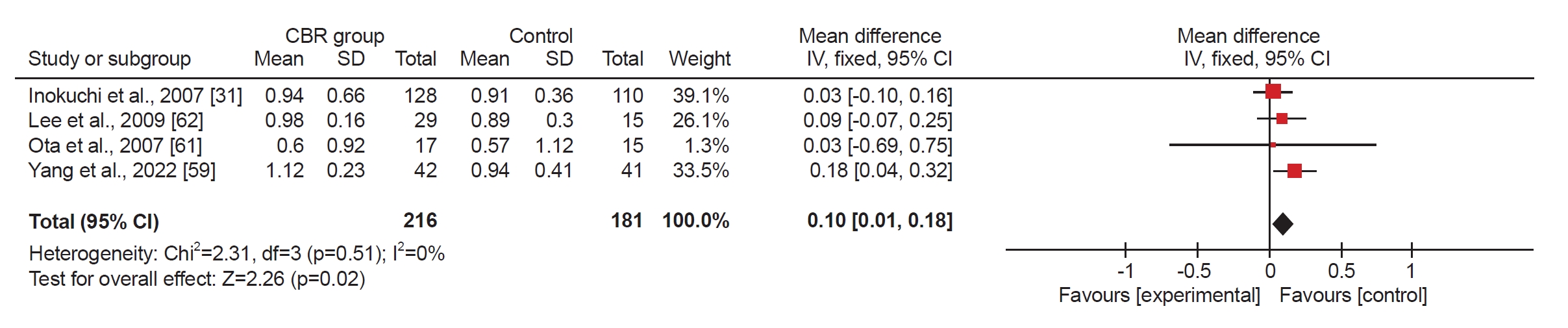
Forest plot of the effects of CBR on gait speed Values are in meter per second (m/s). CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Handgrip strength
Five studies measured handgrip strength [31,60,61,66,77] and three of these studies [31,60,61] were pooled in meta-analysis. In 2007, Inokuchi et al. [31] investigated the effect of CBR (exercise) on handgrip strength on both participants’ left and right sides but only the right side was pooled in meta-analysis. The heterogeneity was moderate and there was no statistically significant difference between the two groups (MD, 1.39 kg; 95% CI, -0.89 to 3.66; I2=73%; Z=1.20, p=0.23; Fig. 3).

Forest plot of the effects of CBR on handgrip strength. Values are in kilogram. CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
One-leg standing time
Four studies [31,59,61,76] evaluated the effect of a CBR program (exercise) on one-leg standing time; three studies (n=353 participants) [31,59,61] were pooled in meta-analysis. The results were homogenous and a significant difference in one-leg standing time was found between the groups (MD, 2.81 seconds; 95% CI, 0.41–5.22; I2=0%; Z=2.29, p=0.02; Fig. 4).

Forest plot of the effects of CBR on one-leg standing time. Values are in second. CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
FRT
Three studies [31,59,61] (360 participants) evaluated physical fitness using the FRT and were pooled in meta-analysis. Pooled results (moderate heterogeneity) showed no significant changes in FRT distance between the CBR (exercise) groups and usual care groups (standard MD, 0.42 cm; 95% CI, 0.00–0.83; I2=64%; Z=1.96, p=0.05) after the intervention (Fig. 5).

Forest plot of the effects of CBR on Functional Reach Test Values are given centimeter. CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Fugl-Meyer Assessment
Changes in motor function in older adults who received CBR (stroke exercise and health-related education) after stroke (measured using the Fugl-Meyer Assessment, FMA) compared to a control group who received usual care alone were evaluated in five studies [36,80-82,88]. All five studies reported a significant improvement in the FMA in the CBR group compared to the control group after the intervention [34-36,81,82]. Results were presented using an un-pooled forest plot, because the intervention durations were not reported in these studies and the quality of the evidence for findings for physical fitness outcomes was rated as very low (Fig. 6).

Forest plot (un-pooled) of the effects of CBR on physical fitness Fugl-Meyer Assessment on older adults with stroke Values are given point. CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Secondary outcomes-performance of ADLs
Six studies evaluated the effectiveness of CBR (exercise and health education) on older adults’ performance of ADL (using the BI) compared to usual care alone. Results were presented using an un-pooled forest plot (Fig. 7). Studies could not be pooled due to methodological problems, including that some studies did not provide information about the intervention duration, the method of randomization or whether data were examined for normality [89].

Forest plot (un-pooled) of the effects of CBR measured using the Barthel Index. Values are given point. CBR, community-based rehabilitation; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Secondary outcomes-HRQoL
Six studies evaluated the effectiveness of CBR on HRQoL [62-65,70,81]. Three assessment tools were used for evaluating HRQoL, and two of these tools (SF-36 and SF-12) were used by more than two studies.
Two studies evaluated the effectiveness of CBR (exercise) on HRQoL (using the SF-36) [62,63] for older adults with knee osteoarthritis and the pooled analysis of these two studies found homogenous effects (non-significant) favoring the CBR intervention group (MD, 8.74; 95% CI, -2.71 to 20.18; I2=0%; Z=1.50, p=0.13; Fig. 8).

Forest plot of the effects of CBR on health-related quality of life (SF-36) on older adults Values are given point. CBR, community-based rehabilitation; SF, Short Form; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Two studies [64,65] evaluated the effect of CBR (exercise, education, and occupational therapy) on HRQoL (measured using SF-12) between two groups compared to a group receiving home-based rehabilitation. Pooled results demonstrated no significant differences between the groups (MD, 2.32; 95% CI, -1.99 to 6.64; I2=66%; Z=1.06, p=0.29; Fig. 9).

Forest plot of the effects of CBR on health -related quality of life (SF-12) on older adults Values are given point. CBR, community-based rehabilitation; SF, Short Form; SD, standard deviation; IV, inverse variance; 95% CI, 95% confidence interval; df, degrees of freedom.
Other outcomes-narrative synthesis
Findings from 17 studies reporting physical fitness assessments [31,61,64-70,72-77,83,86] and four studies [67,70,73,75] reporting secondary outcomes of HRQoL and ADL were not able to be pooled in meta-analysis. These studies were synthesized narratively (Supplementary Table S6).
DISCUSSION
This systematic review synthesized the best available evidence for the effectiveness of CBR for improving physical fitness in community-dwelling older adults living in Asian countries. Results indicated that CBR significantly improves aspects of older adults’ physical fitness, including functional ability (TUG), gait speed, and balance function (one-leg standing test) but there was no significant improvement in strength (handgrip strength).
The pooled results showed that compared with usual care, CBR (multi-component exercise programs) can significantly improve the functional ability (TUG time) of community-dwelling older adults. The improvement in the TUG outcome (-1.89 seconds) reached clinical significance (the minimal clinically important difference [MCID] reported for the TUGt is 1.2 seconds) [90]. This positive result is possibly due to the pooled studies were all being conducted in Eastern Asia (Japan, Korea, and China), and having intervention duration of (12–17 weeks) [31,59-61]. These studies delivered similar intervention components, including strength training as part of the supervised-group exercise intervention. These findings concur with Dun et al. (2022) [76], which utilized 2.4-meter Up and Go test and showed a CBR program (supervised exercise) significantly improved 2.4 m TUG compared with un-supervised exercise (p<0.05). Another un-pooled study, Hasegawa et al. (2013) [66], compared TUG time between genders only in the CBR (strength and balance exercise) group. Findings demonstrated significantly improved TUG time in female participants (p=0.01), but not in males (p=0.82). These differing results may be due to the unequal and small sample size of each between genders (n=60 in female, n=8 in male). Moreover, Hasegawa et al. (2013) [66] failed to compare the TUG time between the CBR intervention group and the un-supervised exercise group.
Walking is an important activity for maintaining and improving physical fitness and an essential component of older adults’ functional ability [91]. Normative age-related values for gait speed indicate an older adult have effective functional ability to engage in their community and slow gait speed is predictive of negative health outcomes like incident health events, increased l length of stay when hospitalized, postoperative morbidity, and death [91,92]. The pooled MD for gait speed was 0.10 m/s which was a clinically significant improvement (MCID for gait speed is 0.10–0.17 m/s) [91]. This pooled result was supported by Liang et al. (2021) [77] who found participants in the “normal cohort” who received the CBR intervention (multidomain intervention including physical and cognitive training, nutritional advice, and health education) showed significant improvement compared with health education only.
Handgrip strength is also an important indicator of frailty and functional decline, and is associated with overall strength in ageing adults. [93,94] Previous systematic reviews reported the MCID of handgrip strength as ranging from 5.0 to 6.5 kg and 2.44 to 2.6 kg. [92,95] However, these two systematic reviews did not provide information specifically for older adults. Our pooled results demonstrated that undertaking CBR programs resulted in no statistically or clinically significant improvement in handgrip strength. This negative finding possibly due to the small number of studies included. Two un-pooled study reported significant improvement on handgrip strength. Hasegawa et al. (2013) [66] found a CBR program significantly improves handgrip strength in female participants. Liang et al. (2021) [77] reported that physical and cognitively declined older adults who completed a CBR program showed significant improvement in handgrip strength compared to the control group after the intervention. However, due to the low quality of study designs and different inclusion criteria these two studies were not able to be pooled in meta-analysis.
Impaired balance is a strong predictor of falls in older adults [96]. Pooled results for assessment of balance using one-leg standing time found statistically and clinically significant improvement in the CBR (exercise) group compared to the usual care group (MCID for one leg standing time is 2.0 seconds) [97]. Although the meta-analysis did not demonstrate a significant difference in balance between the CBR group and the control group (as measured by FRT) the pooled result showed that after the intervention, the FRT result in the CBR group was improved compared to baseline measurements. Balance improvements were also reported by two Chinese studies that compared CBR (exercise) with home-based rehabilitation (exercise) [64,83]. These two studies found significant improvements in balance in the CBR group (measured using the Berg Balance Scale and the Short Physical Performance Battery) [64,83]. However, these two studies could be pooled in meta-analysis due to the different outcome measurements and use of interventions in the control group.
Overall, the modest clinically significant improvement observed in pooled analyses of physical fitness may indicate that the CBR programs provided were not sufficiently intensive for older adults. Healthcare professionals who deliver CBR should design and deliver programs for older adults that are informed by relevant guidelines, such as the WHO guidelines for physical activity for older adults [27]. Some interventions with comprehensive programs included weekly group exercise classes, containing integrated strength and balance exercises, and supervised by professional healthcare staff [31,61,66,77]. Previous systematic reviews have found that community-based group exercise programs provided by healthcare professionals have better adherence compared with individual physical activities, since group exercise programs provide regular, structured, and supervised exercise opportunities which can improve exercise motivation, and provide peer support [98,99].
Un-pooled analysis of studies evaluating ADL showed improvements in the BI of between 4 and 22 points. The MCID of the BI in older patients with femur fracture has been estimated to be 9.8 points [100], therefore this was a clinically important improvement in some studies [34-36,82,83]. This evidence was of low quality as some studies could not be pooled due to insufficient data regarding intervention duration and randomization methods, which ultimately increases the uncertainty of the results.
Appraisal of the certainty of evidence according to GRADE indicated very low-quality results for each outcome and should be interpreted cautiously. There was moderate ROB found in six studies, and indirectness, imprecision and inconsistency were rated as serious for all outcomes because the pooled studies used different intervention durations, had small sample sizes and participants had mixed diagnoses. CBR could adopt older adults’ exercise guidelines and standardized delivery and assessment tools could be utilized by researchers, to facilitate robust evaluation of the effectiveness of CBR for improving older adults’ physical fitness. Interventions should also be designed using evidence-based guidelines that are relevant for older adults’ physical fitness, including physical activity, fall prevention and frailty guidelines [101,102], to be sure they are of sufficiently intensity.
Limitations of the review
Firstly, the relatively small number of studies included in the review suggest that there is a gap in the published evidence for the effectiveness of CBR programs for older adults in Asian countries. Only four countries, including China, Japan, Korea, and Israel, were represented in the review. Findings may not be generalizable for all developing countries in Asia, because differing government policies, available CBR services and cultural context may influence the effectiveness of CBR programs.
Secondly, since GRADE approach was used to rate the certainty of the evidence, this identified that study heterogeneity caused by differing designs reduced the certainty of the findings and limited recommendations that could be made.
Therefore,future studies should use larger sample sizes and robust designs to evaluate the efficacy of CBR programs for improving physical fitness, as well as ADL and HRQoL. Further research comparing the effectiveness of CBR with inpatient rehabilitation or home-based programs on physical fitness would also assist to determine how to effectively increase delivery of evidence-based physical fitness programs for older adults in Asian countries.
CONCLUSION
Chronic diseases in the increasing ageing populations in Asia are associated with a decline in functional ability that results in loss of independence and increasing use of health care services. Programs for older adults that focus on maintaining or improving physical fitness and functional ability and are accessible to older adults in their local community are required to be scaled up. Older community-dwelling adults who completed CBR programs made improvements in some aspects of physical fitness, including functional ability. However, few CBR programs comprehensively addressed physical fitness, such as including elements of strength, balance, and aerobic activity of sufficient intensity, alongside ADL training where required and relevant behavior change support. Research recommendations include using rigorous study designs that include larger sample sizes, validated assessment tools for older adults, interventions of sufficient intensity and describing the intervention components clearly. Further research to design and evaluate CBR programs for community-dwelling older adults in Asian countries is required.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING INFORMATION
This study is funded by the National Key Research&Development Program of China (Grant No. 2020YFC2004205).
AUTHOR CONTRIBUTION
Conceptualization: Xin W. Methodology: Hill AM, Xu D, Xin W, Dou Z. Formal analysis: Xin W, Jacques A, Umbella J. Funding acquisition: Hill AM, Xin W, Dou Z. Project administration: Hill AM, Xu D, Xin W, Dou Z. Visualization: Hill AM, Xu D, Xin W, Dou Z. Writing – original draft: Xin W. Writing – review and editing: Hill AM, Xu D, Dou Z. Approval of final manuscript: all authors.
AVAILABILITY OF DATA AND MATERIALS
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
Anne-Marie Hill is supported by a National Health and Medical Research Council (Australia) Investigator (EL2) Award and the Royal Perth Hospital research foundation. Wei Xin is supported by a Curtin University Fee Offset Scholarship for her PhD.
SUPPLEMENTARY MATERIALS
Supplementary materials can be found via https://doi.org/10.5535/arm.23148.
Supplementary Table S1.
PRISMA 2020 Checklist
Supplementary Table S2.
Search strategy performed on MEDLINE
Supplementary Table S3.
Studies excluded based on full text review
Supplementary Table S4.
JBI critical appraisal tool for quasi-experimental studies
Supplementary Table S5.
JBI critical appraisal tool for randomised controlled trials
Supplementary Table S6.
Studies reporting other physical fitness, ADL and QoL outcomes
Supplementary Fig. S1.
OOOOOO
Supplementary Fig. S2.
Risk of bias graph for randomised controlled trials
Supplementary Fig. S3.
Risk of bias summary for randomised controlled trials
Supplementary Fig. S4.
Risk of bias graph for quasi-experimental studies
Supplementary Fig. S5.
Risk of bias summary for quasi-experimental studies