Epidemiology of Traumatic Spinal Cord Injury in the Himalayan Range and Sub-Himalayan Region: A Retrospective Hospital Data-Based Study
Article information

Abstract
Objective
To compile epidemiological characteristics of traumatic spinal cord injury (TSCI) in the Northern Indian Himalayan regions and Sub-Himalayan planes.
Methods
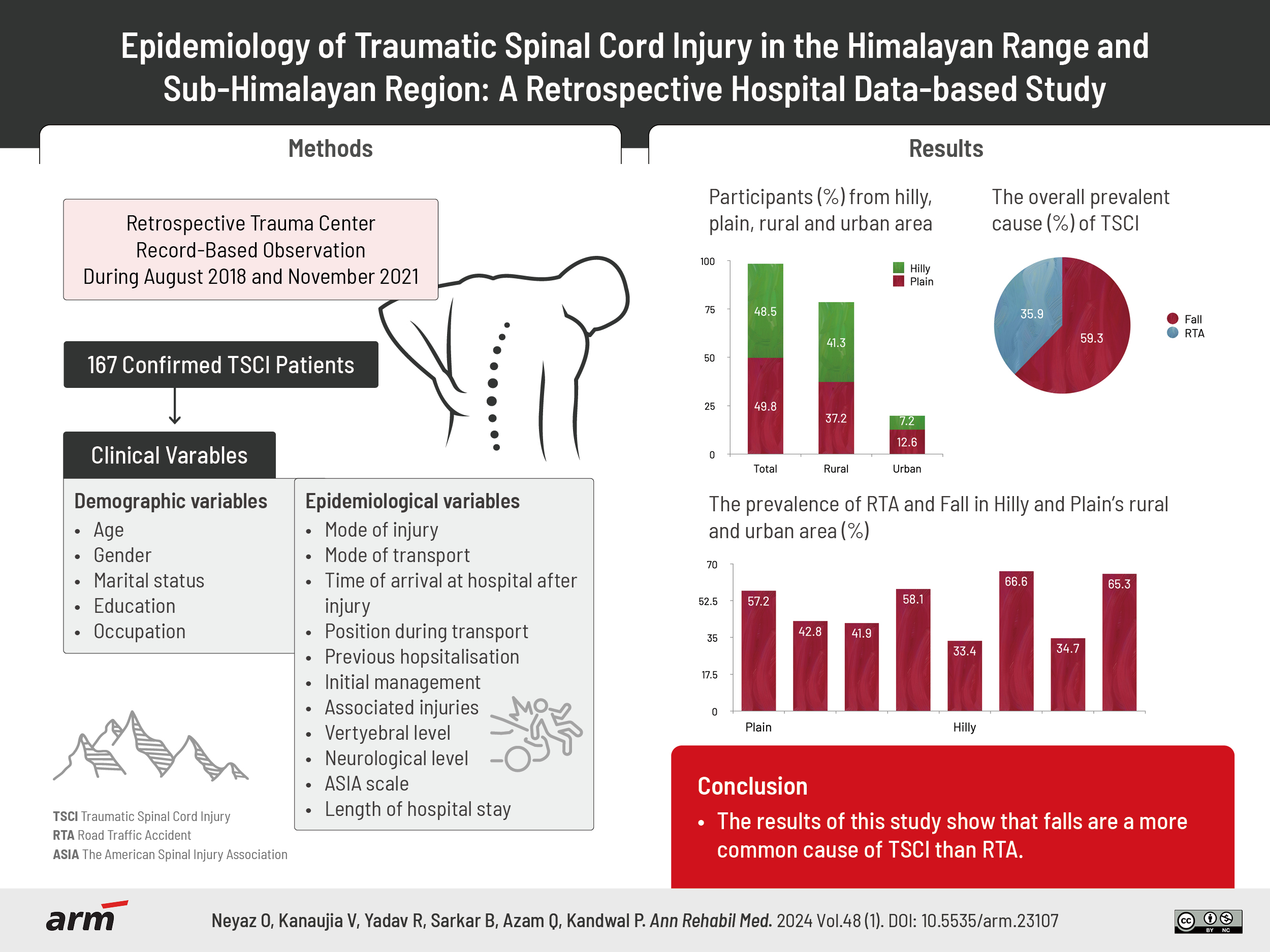
The present study is a retrospective, cross-sectional descriptive analysis based on hospital data conducted at the Department of Physical Medicine and Rehabilitation and Spine Unit of Trauma Centre in a tertiary care hospital in Uttarakhand, India. People hospitalized at the tertiary care center between August 2018 and November 2021 are included in the study sample. A prestructured proforma was employed for the evaluation, including demographic and epidemiological characteristics.
Results
TSCI was found in 167 out of 3,120 trauma patients. The mean age of people with TSCI was 33.5±13.3, with a male-to-female ratio of 2.4:1. Eighty-three participants (49.7%) were from the plains, while the hilly region accounts for 50.3%. People from the plains had a 2.9:1 rural-to-urban ratio, whereas the hilly region had a 6:1 ratio. The overall most prevalent cause was Falls (59.3%), followed by road traffic accidents (RTAs) (35.9%). RTAs (57.2%) were the most common cause of TSCI in the plains’ urban regions, while Falls (58.1%) were more common in rural plains. In both urban (66.6%) and rural (65.3%) parts of the hilly region, falls were the most common cause.
Conclusion
TSCI is more common in young males, especially in rural hilly areas. Falls rather than RTAs are the major cause.
INTRODUCTION
Traumatic spinal cord injury (TSCI) is one of the most common causes of disability. Depending on the nature of the injury, damage to the skeletal, disco-ligamental, spinal cord, and nerve roots can result in varying degrees of disability, including complete paralysis, pain, sensory loss, and bladder-bowel involvement. TSCI has a substantial psychological and economic impact on individuals’ lives, families, and society [1]. Although timely and proper surgical decompression can improve the odds of neurological recovery, rehabilitation is still the most crucial factor in improving these individuals’ quality of life [2].
According to a systematic review by Kumar et al. [3], the global incidence of TSCI is 10.5 cases per 100,000 people. According to the World Health Organization, the incidence of TSI ranged from 3.4 per 100,000 in Europe to 13.7 per 100,000 in Southeast Asia and 54 cases per million in the United States of America. The most common mechanisms for TSCI worldwide were road traffic accidents (RTAs) followed by falls [3,4].
Regional and cultural factors and infrastructural disparities influence significant demographic and epidemiological data differences among countries. Most European research points to transportation-related accidents as the leading cause of TSCI, followed by falls and sports-related injuries. In contrast, the United States sees violence, specifically firearm injuries, as a major contributor after transportation and sports [4-7]. In Asia, patterns vary: China reports falls as the predominant cause, followed by motor vehicle collisions and striking injuries, while Iran emphasizes motor vehicle accidents and falls, including severe drops and related violence. In Nepal and Northern India, falls from significant heights, such as ladders, trees, and cliffs, are particularly prevalent, with RTAs also being a major concern [8-11].
Narrow valleys, steep cliffs and slopes overload India’s Himalayan and Sub-Himalayan regions, and this territory also experiences heavy rains during the monsoon season. The transport infrastructure is not in very good condition. The parapets on the roof of houses and side walls of stairs are either of low height or completely lacking, making them a source of injury. People residing in these areas depend on nearby forest areas for their livelihood.
These geographical factors play a crucial role in the incidence, prevalence, mortality, and morbidity of TSCI patients in this part of the country. Moreover, this part has limited access to tertiary-level healthcare facilities. Even though India is the world’s second-most populous country, demographic and epidemiological data are scarce for TSCI. The present study aimed to assemble demographic and epidemiological characteristics of TSCI in the Himalayan and Sub-Himalayan regions.
METHODS
The current study is a cross-sectional descriptive analysis of people with TSCI based on hospital data. It was carried out with prior approval from the Institute Ethics Committee, All India Institute of Medical Sciences, Rishikesh (approval number: AIIMS/IEC/21/12) in the Department of Physical Medicine and Rehabilitation and the Spine Unit of the Trauma Centre of a tertiary care hospital in Uttarakhand, India. The requirement of informed consent in this study was waived because the study was a retrospective study. All personal details of the participants were kept confidential throughout the study. The study sample comprises individuals with TSCI admitted to the tertiary care center between August 2018 and November 2021. A prestructured proforma was used for evaluation, including demographic parameters such as age, sex, marital status, address, educational status, and occupation. The epidemiological variables included mode of injury, time of arrival in the Institute after injury, mode of transport used during transfer, body position during transfer, any previous hospitalisation, type of care provided during initial admission at another healthcare facility, vertebral level of injury, neurological level of injury (NLI), the severity of injury based on American Spinal Injury Association Impairment Scale (AIS) [12], and associated injuries. People who died before arriving at the hospital were excluded from the study.
Operational definition
TSCI results from a sudden, traumatic impact on the spine that fractures or dislocates vertebrae, where displaced bone fragments, disc materials, or ligaments bruise or tear into the spinal cord tissue [13].
Himalayan region: The Indian Himalayan region in Northern India is denoted as the hilly region in the study, further divided into hilly-urban and hilly-rural areas.
Sub-Himalayan region: The planes after the foothills of the Himalayas in Northern India are denoted as the plains in the study, which are further divided into plains-urban (PU) and plains-rural (PR) areas.
Statistical analysis
IBM SPSS 27.0 (IBM Corp.) and Microsoft Excel 2016 Professional Plus (Microsoft Corp.) software were used for data management and analysis. In the statistical analysis, categorical variables were presented in number (%), and continuous variables were presented as mean±standard deviation. For multigroup comparisons of categorical variables like sex and marital status, a chi-square test was used. A one-factor ANOVA test for independent measures was used for continuous variables like age. The p-value was significant at <0.05.
RESULTS
A total of 3,120 trauma patients were admitted during the study period, with 167 having TSCI. The mean age of the people with TSCI was 33.5±13.3, ranging from 4 to 72 years. The age difference was not statistically significant between rural and urban areas of hills and plains. Males were significantly affected in this study, with a male-to-female ratio of 2.4:1. Most participants, 108 (64.7%), were married at the time of the injury, although the difference is insignificant. Roughly 74 (44.3%) individuals had a high school education or less, while 23 (13.7%) were uneducated (without formal education in any institute). In this study, the majority of patients were from the state of Uttarakhand 112 (67.1%), followed by Western Uttar Pradesh districts 52 (31.1), and a few from neighbouring Himachal Pradesh 3 (1.8%). A total of 83 participants (49.7%) are from the plains, while 84 (50.3%) are from the hilly region. Individuals from the plains had a rural-to-urban ratio of 2.9:1, compared to 6:1 in the hilly region. The study included a wide range of occupations, but homemakers 30 (17.9%), students 44 (26.4%), farmers 27 (16.2%), and labourers 21 (12.6%) were the most common (Table 1).

Demographic profile of the patients
In this study, the most common cause of TSCI was Falls 99 (59.3%), followed by RTAs 60 (35.9%), other causes were 8 (4.8%), which involved assault 2 (1.2%), bullet injury 2 (1.2%), a heavy object falls on back 3 (1.8%), Ankylosing spondylitis 1 (0.6%). Falls were the most common cause in urban 8 (66.6%) and rural 47 (65.3%) areas of the hilly region. RTAs were the most common 12 (57.2%) in the PU areas, while Falls were more common in the PR area 36 (58.1%). Falls were more common in both males and females than RTAs, but females had a much higher proportion of Falls 41 (82.0%) than males 58 (49.6%).
The time taken to get to the health center after an injury varies greatly. A total of 35 (20.9%) participants were reached within 24 hours of injury, and 45 (26.9%) were brought between 24 and 48 hours. After an injury, the most common transfer mode was an ambulance 128 (76.1%), but cars 38 (22.8%), and bikes 1 (0.6%) were also used. Most cases were transferred supine during the transfer 165 (98.8%). A total of 143 (85.6%) participants were previously hospitalized at a nearby primary health care facility and referred to the tertiary center; only 24 (14.4%) participants reported directly. A total of 55 (32.9%) participants were managed conservatively, while 112 (67.1%) were managed surgically. Out of 112 participants, 83 were operated on inside the Institute, while 29 were outside.
A total of 38 of the participants (22.7%) suffered various associated injuries. In total, musculoskeletal injuries (single/multiple bone fractures or dislocations at different sites) are more common (9.0%), followed by chest injuries (6.5%) (rib fracture, pneumothorax, and haemothorax). A total of 19 participants (11.4%) had multiple vertebrae fractures, while the rest (89.2%) had single vertebrae fractures. Cervical (C1–C7), thoracic (T1–T10), thoracolumbar (T11–L1), and lumbar (below L1) regions accounted for 28.2%, 24.5%, 32.3%, and 3.5% of vertebral injuries, respectively, in single vertebrae. Thoracic vertebrae (41.3%) were the most commonly affected in this study, followed by cervical vertebrae (30.5%).
In this study, NLI distribution was like upper cervical (C1–C4) (10.8%), lower cervical (C5–C7) (21.0%), upper thoracic (T1–T6) (11.3%), lower thoracic (T7–T12) (40.1%) and lumbar (L1–L5) (19.1%). Complete paralysis (AIS-A) was found in 85 individuals (50.9%), incomplete sensory (AIS-B) in 22 individuals (13.2%), and incomplete motor (AIS-C) in 36 (21.5%). The average length of stay in the hospital was 14.6±14.6 days, with stays ranging from 1 day to 125 days. In the first week of admission, 47 individuals (28.1%) were discharged, while 67 people (40.1%) were discharged in the second week. Length of stay was more for higher levels (above T6 level) (16.2±18.6 days) in comparison to the lower level (below T6 level) (13.3±9.7 days). A total of 6 people with TSCI (3.5%) reported death, all belonging above the T6 level (Table 2).

Epidemiological variables
DISCUSSION
TSCI is one of the most debilitating disabilities that affect people with TSCI and their families and is a social and economic burden on society. Families in developing countries must face hospitalisation costs and continued treatment due to a lack of socialized medicine and structured medical insurance policies. As a result, determining modifiable factors using precise epidemiological features will undoubtedly aid in formulating prevention initiatives.
In our study, the average age of the afflicted was 33.5±13.3 years, aligning with the mean age observed in various South Asian and Middle Eastern countries: India (34.4 years), Pakistan (33.3 years), Nepal (21–30 years), Saudi Arabia (29.5 years), and Iran (29.1 years) [9,14-16]. In contrast, Western studies show a trend of increasing age over time. For instance, the United State saw the average age at injury rise from 29 years in the 1970s to 43 years post-2015. Similarly, New Zealand’s median age of injury increased from 43 to 48 years, and Denmark’s shifted from 29.0 to 47.5 years. Notably, Italy and Iceland present average ages of 59.2 and 39 years, respectively [5-7,17,18].
The male-to-female ratio in this study was 2.4:1, which was quite similar to the distribution in other countries like Spain and Austria [19,20] but lower than the worldwide (3.8:1) [21] and other Indian studies [11,22]. This finding suggests that young males are more prone to TSCI than females. A possible explanation is that in most families, males are the primary earning members of the family and hence get exposed to greater risk for falls and RTAs. On the other hand, women were primarily involved in low-risk home jobs and outdoor areas [23].
Most participants in our study were married at the time of injury, compared to individuals in studies from the United States (30.6%) [24]. This could be because Indians marry at a younger age. Most of the participants in this study fall into the category of low education and working as manual labour in farming and other dangerous vocations, making them more vulnerable to TSCI. Those with a higher level of education were less likely to be involved in TSCI accidents.
In Hilly-rural areas, housewives, students, and unemployed people are more frequently involved in TSCI. It is possible because they mostly engage in domestic work like fetching household goods and water, collecting wood from forests, and climbing trees, and hilly geography makes them prone to incidents like falling from height.
Our study’s overall rural versus urban background ratio was approximately 4:1 against the proportion of 3:1 for the Indian population [25]. It might be due to the hospital’s location in the foothills of the Himalayas in Northern India. The center primarily serves the rural population as it is the only specialized referral center in this region. This tertiary center caters to a large population, including people from Uttarakhand, Western Uttar Pradesh districts, and neighbouring Himachal Pradesh. In the present study, 31.1% of participants were employed at the time of injury compared to the Indian population (48.24%) [26]. It is possible that folks with a lower socioeconomic position would have travelled long distances to get treatment at our Institute.
Falls were a more common cause of TSCI than RTAs in this study. In contrast to affluent countries where RTAs were the most common cause, Falls were the most common mode of injury in most Indians [22,27,28] and southern Asian research [29,30]. More specifically, Falls were widespread in urban and rural parts of the hilly region. This finding correlates with a study in the hilly areas of the North-East part of India and Nepal [10,31]. Urban areas have more RTAs in the plains, while falls are common in rural areas. It suggests that because of better road conditions and highways, metropolitan areas are more involved in RTAs. Poor road infrastructure and poor driving conditions in rural areas, on the other hand, limit the RTAs.
Post-injury duration of arrival at a tertiary care facility is crucial. Clinical evidence favours a 24-hour threshold in defining early surgical decompression. A significantly greater proportion of patients who underwent early surgery (19.8%) demonstrated a 2-or-more grade improvement in AIS at six months compared with those who underwent late surgical intervention (8.8%) [32]. About 52% of participants in our study were admitted after 48 hours of injury. Most of them were initially managed at the primary care center and then referred to a higher center. The reason could be a lack of transport logistics from the field, access to a tertiary care center, or polytrauma.
Most of the individuals were transported in the supine position after the injury. For suspected TSCI cases, immobilisation during hospital transit is a significant concern. To minimise subsequent neurological injuries during transportation, supine placement, a board, a collar, and head immobilisation with towels or foam wedges have been proposed [23,33,34]. Primary healthcare providers in hilly locations should be trained in the initial management of SCI and the early and safe transfer of affected persons to a specialized center.
The thoracic spine is injured in most of the participants in the present study, while combined T12 and L1 have the highest proportion. In a systematic review by Golestani et al. [35], out of 37 studies, in 22 studies, most injuries occurred at the cervical level, while in 12 studies, the thoracic level was the most prevalent level of injury, and only in 3 studies, the lumbosacral level had the highest injury frequency. Because of anatomical considerations, the thoracolumbar junction is the most usual location. The rib cage, the most movable part of the spine, makes the dorsal spine less mobile than the lumbar spine. The thoracolumbar area is vulnerable to injury as it transitions from a fixed to a mobile component [27].
Prevention is the key to reducing the burden of TSCI. Some preventive strategies are building adequate height bannisters on the roof, railing with hand support near stairs, preventing unnecessary tree climbing, utilising rough tiles for bathroom floors, building good road infrastructure with proper barricading, enforcing speed limits on city roads, and raising awareness of traffic rules. Integrating specialized rehabilitation services for people with TSCI can aid their recovery, improve their quality of life, and increase their contribution to society.
There are some limitations in the generalizability of the findings to the broader Indian TSCI population because our sampling method was only based on one hospital record from Northern India. Also, excluding 6 individuals who passed away before reaching the hospital might lead to underestimating the severity in some instances.
In conclusion, to summarise, the demographic and epidemiological data of TSCI in India differ from those in developed countries, with Falls rather than RTAs being the leading cause. Most people belong to younger age groups and have a complete injury, with the thoracolumbar spine being the most affected. In terms of future research, a multicentric longitudinal study with a larger number of TSCI patients is required to evaluate the long-term impact of the injury on functional status, community integration, and quality of life indicators. Other information, such as the financial impact of the injury and caregiver stress, may also be provided. With the number of TSCI patients expected to rise in the years ahead, establishing a national database would be beneficial for developing preventive and rehabilitative measures.
Notes
CONFLICTS OF INTEREST
No potential conflict of interest relevant to this article was reported.
FUNDING INFORMATION
None.
AUTHOR CONTRIBUTION
Conceptualization: Neyaz O. Methodology: Neyaz O. Formal analysis: Neyaz O, Kanaujia V, Yadav RK. Project administration: Azam MQ, Kandwal P. Visualization: Neyaz O, Kanaujia V, Writing – original draft: Neyaz O, Kanaujia V, Sarkar B. Writing – review and editing: Neyaz O, Kanaujia V, Yadav RK. Approval of final manuscript: all authors.