Effects of Home-Based Boxing Training on Trunk Performance, Balance, and Enjoyment of Patients With Chronic Stroke
Article information

Abstract
Objective
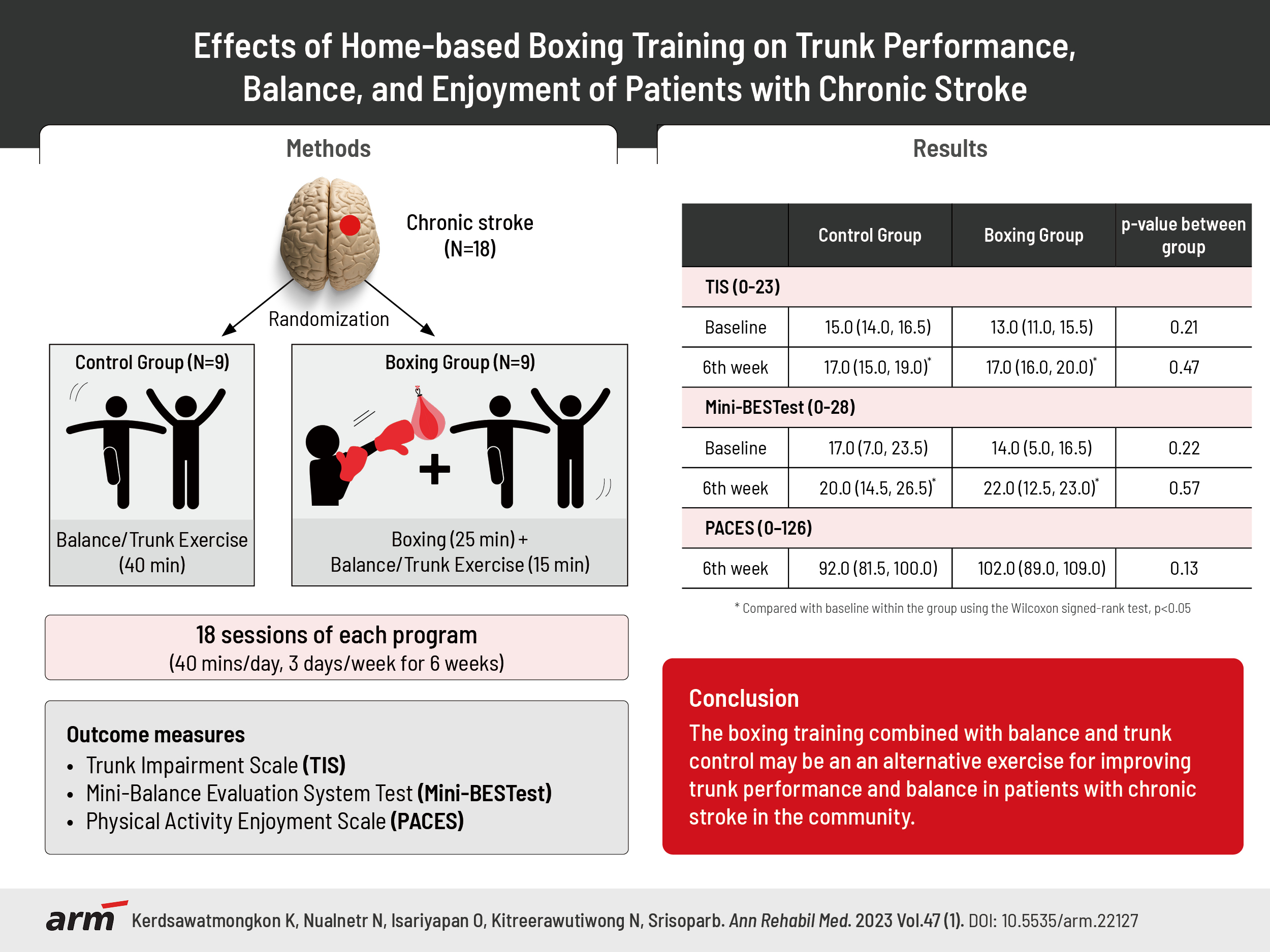
To investigate the effect of 6 weeks of home-based boxing training on trunk performance, balance, fear of falling, and level of therapy enjoyment in individuals with chronic stroke.
Methods
Eighteen participants with chronic stroke were randomly divided into boxing and control groups (9 patients per group). The boxing group received home-based boxing training for 25 minutes plus balance and trunk exercise training for 15 minutes, while the control group received only home-based balance and trunk exercise training for 40 minutes, three days a week for 6 weeks. The Trunk Impairment Scale (TIS), Mini-Balance Evaluation Systems Test (Mini-BESTest), Activities-specific Balance Confidence (ABC) scale, and Physical Activity Enjoyment Scale (PACES) were assessed at baseline, and at 2, 4, and 6 weeks post-training. The Wilcoxon signed rank test and Mann–Whitney U-test were used to determine differences between pre- and post-training within and between groups. Statistical significance was set at p<0.05.
Results
The TIS scores significantly increased from 13 to 17 points in the boxing group (p<0.05) compared to an increase from 15 to 17 points in the control group (p<0.05). The Mini-BESTest scores significantly increased from 14 to 22 points in the boxing group (p<0.05) compared to an increase from 17 to 20 points in the control group (p<0.05). There were no differences in the TIS, Mini-BESTest, ABC, and PACES scores between the two groups.
Conclusion
Home-based boxing training with balance and trunk exercise training had a similar training effect compared to home-based balance and trunk exercise training.
INTRODUCTION
Stroke not only leads to muscle weakness of the upper and lower limbs, but also of the trunk muscles [1]. Deterioration of trunk muscle function after stroke results in poor movement of the upper and lower limbs and reduced functions in activities of daily living. Survivors of chronic stroke with reduced trunk stability are likely to experience decreased upper limb function in daily activities [2], impaired walking ability [3,4], and an increased risk of falls [5]. Consequently, their social participation may decrease. Several methods improve trunk performance and balance in stroke patients, including core stability training [6], as well as alternative exercise programs such as yoga [4] or tai chi [3], which activate trunk muscle control and improve balance during changes in position.
Recently, boxing training was employed on neurology patients, resulting in improved balance, mobility, and quality of life. Boxing training involves whole-body movements, while the upper limbs are used to punch. A speedy repetitive punching movement of the arms, together with weight-bearing and anticipatory postural adjustments [5], seem to improve trunk performance and balance. Similarly, a group kickboxing program improved balance and functional mobility in patients with multiple sclerosis [7,8]. In addition, boxing training was noted to improve the balance, mobility, and quality of life of patients with Parkinson’s disease [9,10]. Boxing training was also applied to patients with acute stroke, and it increased the patients’ upper limb function, balance, gait, and quality of life [11]. However, no published study has investigated the effects of boxing training on trunk performance and balance in people with chronic stroke. Therefore, this study aimed to investigate the effects of home-based boxing programs on trunk performance and balance in individuals with chronic stroke.
MATERIALS AND METHODS
This study was a matched-pair, single-blind study approved by the Institutional Review Board (IRB) of Naresuan University (IRB No. 0500/61). Each participant signed the IRB-approved informed consent form for publication, and participants’ rights were protected following the ethical principles of the Helsinki Declaration.
Participants
Patients with chronic stroke living in the Bangrakam district in Phitsanulok Province, Thailand, were recruited. The inclusion criteria were as follows: 1) diagnosis of the first stroke more than 6 months previously; 2) stable medical status; 3) age 50–80 years; 4) no cognitive impairment as screened through the 2002 Thai Mini-mental State Examination; 5) no severe cardiorespiratory, musculoskeletal, or neurological conditions affecting sitting ability; and 6) able to stand independently. The exclusion criteria were as follows: 1) Modified Ashworth Scale score greater than 2 for shoulder adductors, elbow flexors, wrist flexors, hip adductors, knee extensors, and ankle plantar flexor muscles; 2) patients with contraversive pushing or bilateral hemiplegia; and 3) other safety contraindications to exercise. A sample of 9 patients per group was necessary to achieve 80% power at a 5% significance level, with a 15% dropout rate, based on a study by Jeon et al. [12]. Concealed allocation was performed using a computerized program for either the boxing or control group to reduce selection bias. The randomization was stratified by age, sex, time post-stroke, and Mini-Balance Evaluation Systems Test (Mini-BESTest) scores of the patients to provide equal distribution. Participants and physiotherapists who trained the patients in each group were not blinded due to the nature of the study.
Home-based boxing and balance and trunk exercise training program
All participants were provided with a 60-minute session, 3 times per week for 6 weeks in their homes by two different physiotherapists with a three-year average of working experience in the field of neurorehabilitation. The physiotherapist supervising the boxing group had received boxing training from a Muay Thai boxing instructor and had more than 10 years of experience before conducting this study. The physiotherapists visited the participants’ homes three days per week during the initial 2 weeks for training, instructing according to the program, and correcting movements until the participants and their caregivers followed the program correctly. Subsequently, the physiotherapists decreased their visits from 2 days weekly on weeks 3 and 4 to 1-day weekly on weeks 5 and 6. The participants and their caregivers continued and recorded their training in the logbook on the days there were no visits from the physiotherapist. Table 1 shows the intervention for the boxing and control groups.

Interventions for the boxing and control groups
All training programs started in the sitting position, and then progressed to altering the base of support to standing and marching within 2 weeks. Fig. 1 demonstrates boxing in the sitting and standing positions.
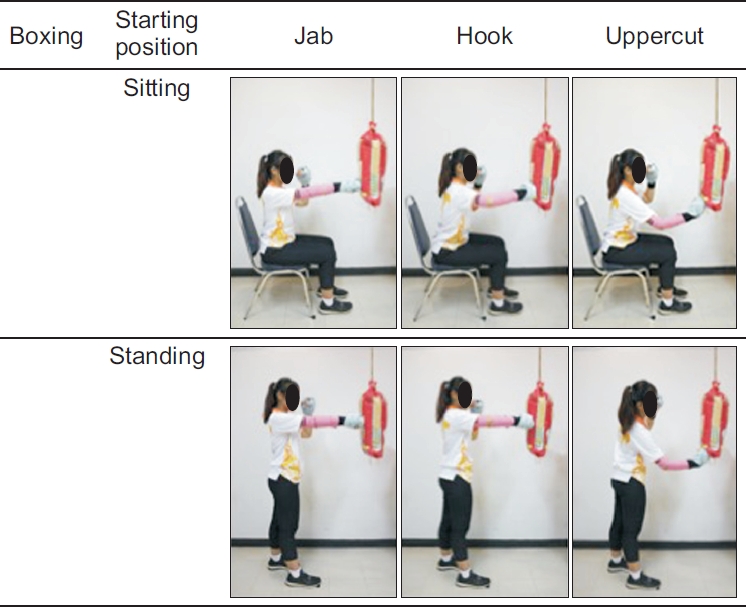
Photographic illustrations of boxing in the sitting and standing positions (with simulated right hemiparesis).
The participants’ blood pressure and heart rates were monitored before, during, and after training. The participants in the boxing program were instructed to perform boxing training at level 3 below the modified Borg scale. The boxing training was developed from previous literature with the aim of improving trunk control and balance in patients with stroke. Boxing equipment included mitts adapted from towels and 10 kg sandbags that contained sand and cloth. The boxing training included maneuver such as the jab, hook, and uppercut, repeated 30 times per set with 2-minute rest intervals. The progression of boxing training included increasing the repetitions and angle of boxing. The participants in the control group underwent balance and trunk exercise training. Trunk exercise training comprised trunk flexion/extension, rotation, and lateral flexion by focusing on the core muscles. Balance training included leaning forward, sideways, upward, and downward while keeping the arms straight. Balance and trunk exercises were performed 30 times per set with 2-minute rest intervals, starting in the sitting position before progressing to altering the base of support to standing and marching for 2 weeks, similar to boxing training. Warm-up and cool-down involved stretching the trunk and upper and lower limb muscles and active assisted movement of all joints.
Outcome measures
The participants in the boxing and control groups were blinded to their style allocation, and the physiotherapists for each condition did not know the existence of the other condition. Moreover, the assessor who collected the data was blinded to the treatment allocations. Outcomes were measured at the following time points: at the start of the program, on the second, fourth, and sixth weeks following the interventions, and at the end of the program. The primary outcome measure used to evaluate trunk performance was the Trunk Impairment Scale (TIS). The TIS was developed to measure trunk performance in people with stroke [13]. There are 17 items in each of the three subscales of TIS: static sitting balance, dynamic sitting balance, and coordination. Static sitting balance was assessed when the participants’ feet were supported, with the legs positioned passively and actively across each other. The dynamic sitting balance subscale was assessed when the participants performed trunk lateral flexion and unilateral lifting of the hip. The participants were then asked to rotate the upper or lower part of the trunk to assess the coordination subscale. The scores obtained ranged from 0 to 23; a higher score represented higher trunk performance [14].
Secondary outcome measures included balance, balance confidence, and the enjoyment of being involved in the program as assessed by the Mini-BESTest, Activities-specific Balance Confidence (ABC) scale, and Physical Activity Enjoyment Scale (PACES), respectively. The Mini-BESTest, the short version of the BESTest, was used to address anticipatory postural adjustment (sit to stand, rise to toes, stand on one leg), reactive postural control (compensatory stepping correction forward, backward, and lateral), sensory orientation (stance with feet together on a firm surface, with eyes open or closed and stance on inclined surface with eyes closed), and dynamic gait balance (change in gait speed, walk with head turns, walk with pivot turns, step over obstacles, and timed up and go with a dual task). The total score ranges from 0 for a minimal performance to 28 for a perfect performance [15]. The ABC scale, a 16-item structured questionnaire, was used to measure participants’ confidence in performing various activities without falling or feeling unsteady. The ABC score ranges from 0 (no confidence) to 100 (full confidence) [16]. PACES is an 18-item scale that assesses the participants’ enjoyment of the intervention they received. The participants were asked to rate how they felt about the boxing or balance training program using a 7-point Likert scale from 1 (I enjoy it) to 7 (I hate it). PACES has 11 negatively worded items and 7 positively worded items. The scores range from 18 to 126, with a higher score indicating higher enjoyment [17].
Statistical analysis
Statistical software (IBM SPSS 24.0; IBM Corp., Armonk, NY, USA) was used for the data analysis. The normality of the outcome measures was tested using the Shapiro–Wilk test, which demonstrated a non-normal distribution. Descriptive statistics were presented as means±standard deviation for normally distributed variables and medians (interquartile range) for non-normally distributed variables. Friedman’s two-way analysis of variance was used to compare the effects of boxing training and conventional physiotherapy in improving trunk performance, balance, and balance confidence. The Wilcoxon signed-rank test and Mann–Whitney U-test were used to compare all variables within and between groups, respectively. The significance level was set at p<0.05.
RESULTS
Initially, 79 patients were screened for eligibility. Fifty-three patients were excluded due to physical limitations such as inability to walk, shoulder stiffness, back pain, and inability to communicate effectively. Eight patients were excluded as their mental limitations (4 patients) and poor communication (4 patients). Eighteen participants were matched and randomly assigned to either the boxing or control group. Four of the 9 participants in the boxing group completed training and complained about strains in the fingers, wrist, and shoulder joints, while 1 of the 9 participants in the control group reported knee pain on day one. These symptoms were absent one day after the training. All 18 participants completed the study, and their data were available for analysis. A flowchart of the research participants and their participation is shown in Fig. 2.
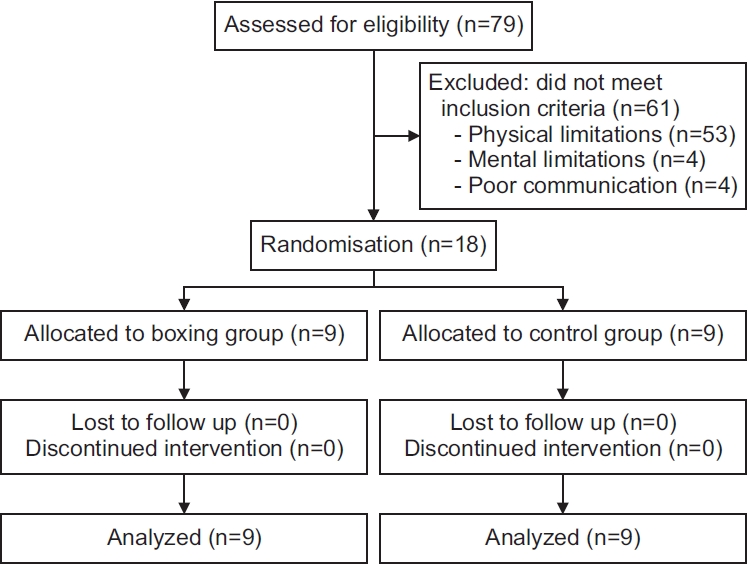
Flowchart depicting the participant selection.
There were no significant differences in the demographic and clinical characteristics of the participants between the two groups at baseline (Table 1). There were also no significant differences in trunk performance, balance, and balance confidence between the groups (Table 2).
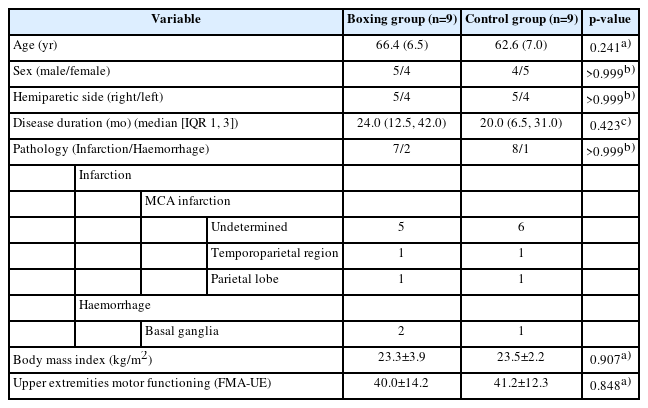
Participant demographics
Table 3 shows the outcome scores of the 18 participants. Within-group differences in scores across the four assessment occasions (p<0.05) were found regarding the TIS, Mini-BESTest, and ABC scales in both groups. However, only the boxing group showed a significance difference between baseline and the sixth-week assessment on the TIS dynamic sitting balance and the Mini-BESTest anticipatory and reactive postural control. Significant between-group differences were found in PACES during the second-week assessment (p=0.02). After 6 weeks of intervention, the median TIS score of the boxing group was 17.0 (16.0, 20.0) and the median Mini-BESTest score of the boxing group was 22.0 (12.5, 23.0).
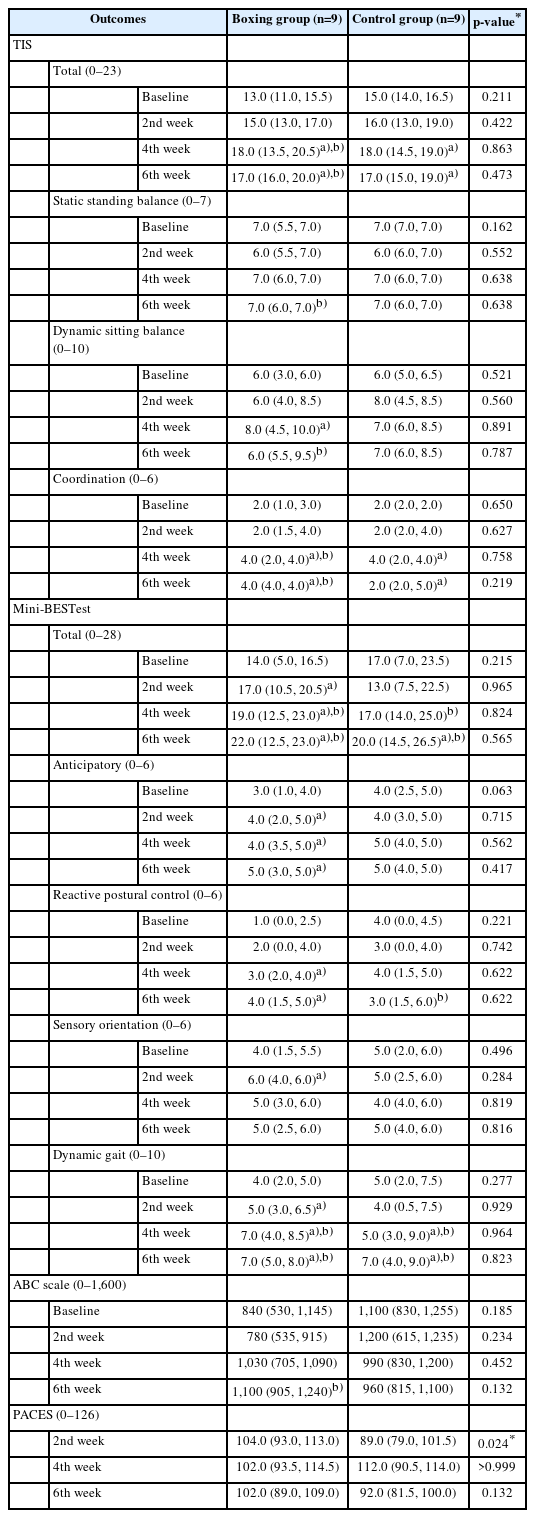
Outcome scores during the four assessment occasions
DISCUSSION
The results of this study demonstrated that boxing, balance, and trunk exercise training improved trunk performance, balance, and balance confidence in patients with chronic stroke. However, boxing training seemed to improve dynamic sitting balance and anticipatory and reactive postural control faster than balance and trunk exercise training (control group). Furthermore, patients with chronic stroke enjoyed the boxing program more than the conventional balance and trunk training program.
One probable reason why the boxing program did not have significantly better results on trunk performance and balance than the control group might be due to both programs incorporating activities that require participants to shift their weight from midline to different directions, which is beneficial for improving trunk control and proprioception in patients with chronic stroke [18]. Although the boxing program stipulated that the participant had to punch the sandbag at a specified distance, some participants with stroke were limited in moving their hemiparetic arm to reach the target. Therefore, proprioceptive inputs may have been inadequate in providing accurate feedback on their movements. Consequently, they had poor coordination to punch and control their upper limb movements [19]. If the participant’s upper limb could not reach the target (the sandbag), their trunk muscles may not have been adequately activated [20,21]. It was observed that TIS scores in the boxing group increased by 4 points, while TIS scores in the control group increased by two points. This may be due to the fast and repeated upper limb movements required during punching, which could activate trunk muscles [22] better than the balance and trunk exercises of the control group. Boxing training could have changed the patient’s balance significantly over 6 weeks because the 6-point change in the Mini-BESTest score exceeded the minimal clinically important difference of 4 points [23]. This finding demonstrates that boxing training 3 times per week for 2 weeks can improve balance in patients with chronic stroke, especially with regard to anticipatory and reactive postural control. After 6 weeks of boxing training, more than 80% of the participants in the boxing group showed a Mini-BESTest score higher than 17.5, which is the cut-off score of the Mini-BESTest [15]. Therefore, these participants had a decreased risk of falling.
The findings of this study contrast with those of previous studies that found that boxing improved balance more than conventional physiotherapy. This may be due to their participant pool consisting of subacute patients with stroke, who may have better recovery trajectories than chronic stroke patients [11]. The boxing program also showed positive results in other neurology patients, including those with multiple sclerosis [8] and Parkinson’s disease [9]. This may be because most patients with multiple sclerosis and Parkinson’s disease can control the movement of their upper limbs more accurately than patients with stroke and hemiparetic upper limbs. Although, patients with pontine and cerebellar stroke, which produce symptoms such as truncal and limb ataxia [24,25], were not recruited into this study, the majority of participants in this study were stroke patients with middle cerebral artery infarction who presented with muscle weakness and poor muscle control [26].
To our knowledge, this is the first study to investigate the effects of a home-based boxing program on trunk performance, balance, fear of falling, and level of therapy enjoyment in individuals with chronic stroke. The physiotherapist visited patients to monitor their training and empower patients and their caregivers to continue with the boxing programs on their own. The patients were able to complete the training program independently over 6 weeks. Therefore, a boxing training program seems feasible and sustainable. The patients appeared to enjoy the boxing program more than the control program that involved balance and trunk exercise training during the physiotherapist’s visits in the first 2 weeks. This might be due to the perceived impression that boxing training was a novel therapeutic training for them, and thus, more appealing. In addition, they received personalised attention and positive encouragement from the physiotherapist. In the boxing group, hemiparetic shoulder and wrist injuries occurred during uppercut punches, a technique that is more difficult than other punching techniques. Consequently, the punching style for patients with stroke should be reviewed and customized to select the most appropriate for patient use. Moreover, the sandbag that we used should be softer and the boxing mitt should be thickened, especially over the fingertips, to prevent injuries.
This study has some limitations. The matched randomized trial might have introduced biases in the selection of participants. Furthermore, boxing training could be risky if the patients do not or cannot move correctly, predisposing the patient to a loss of balance or straining of the upper limbs during boxing. Stroke participants who were able to follow the program required a higher level of functioning. Therefore, we excluded many patients who did not meet this criterion. Consequently, the results of the boxing program in this study can only be generalized to chronic patients with stroke using the study’s inclusion and exclusion criteria. Additionally, the results of this study should be interpreted with caution as it had a small sample size. Further studies should investigate the results of boxing training at different performance levels in individuals with stroke using larger sample sizes.
In conclusion, the 6-week boxing training program combined with balance and trunk control training had positive effects on trunk performance, balance, and fear of falling among patients with hemiplegia from chronic stroke. Although no statistically significant differences were observed between the boxing and control groups in terms of trunk performance and balance, participants in the boxing program had slightly greater satisfaction with the training program. Therefore, boxing training combined with balance and trunk control may be an alternative exercise for improving trunk performance and balance in patients with chronic stroke in the community.
Notes
No potential conflict of interest relevant to this article was reported.
Conceptualization: Kerdsawatmongkon J, Srisoparb W. Formal analysis: Kerdsawatmongkon J, Srisoparb W, Isariyapan O. Funding acquisition: Srisoparb W. Methodology: Kerdsawatmongkon J, Srisoparb W, Isariyapan O. Visualization: Srisoparb W, Nualnetr N, Kitreerawutiwong N. Writing – original draft: Kerdsawatmongkon J, Srisoparb W. Writing – review and editing: Srisoparb W. Approval of final manuscript: all authors.
Acknowledgements
This work was funded by the National Research Council of Thailand (No. 910244).