Predictors of Aspiration Pneumonia in the Elderly With Swallowing Dysfunction: Videofluoroscopic Swallowing Study
Article information

Abstract
Objective
To identify the variables of videofluoroscopic swallowing study (VFSS) that are useful for predicting the risk of aspiration pneumonia in elderly patients with dysphagia.
Methods
A total of 251 patients (aged 65 years or more) were included and divided into a pneumonia group (n=133) and a non-pneumonia group (n=118). The pneumonia group included patients who had been diagnosed with aspiration pneumonia, and individuals in the non-pneumonia group did not have pneumonia but were referred for VFSS. The medical records and results of VFSS were reviewed and compared between the groups retrospectively.
Results
The pneumonia group exhibited a male preponderance and a higher 8-point Penetration-Aspiration Scale (8PPAS) score. The mean values of 8PPAS score for swallowing thick liquid and rice porridge was significantly higher in the pneumonia group. The pharyngeal delay time (PDT) and pharyngeal transit time (PTT) were significantly longer in the pneumonia group. The amounts of vallecular and pyriform sinus residue were increased in the pneumonia group. The delay in swallowing reflex and the decrease in laryngeal elevation were more frequently observed in the pneumonia group. Among those variables, PDT and PTT were identified as significant predictors of aspiration pneumonia based on logistic regression analysis.
Conclusion
The present study delineated the findings of VFSS, suggesting an increased risk of aspiration pneumonia in elderly patients with dysphagia. The results demonstrate that prolonged PDT and PTT are significant predictors of aspiration pneumonia.
INTRODUCTION
Aspiration pneumonia is a type of lung infection that develops after the inhalation of a relatively large amount of bolus consisting of colonized oropharyngeal or upper gastrointestinal contents that exceed the immune system of the respiratory system [1]. Aspiration pneumonia is generally considered a part of community- and hospital-acquired pneumonias rather than a distinct disease entity [2]. The prevalence of aspiration pneumonia accounts for approximately 5% to 15% of cases of community-acquired pneumonia, but its proportion of hospital-acquired pneumonia is unknown [3,4]. Aspiration pneumonia increases the possibility of mechanical ventilation, the duration of stay in the intensive care unit (ICU), the length of hospital stay, and the mortality rate compared with non-aspiration pneumonia [5]. It has been reported that older age, male gender, lung disease, diabetes mellitus, severe dementia, and poor oral health are risk factors for aspiration pneumonia [6]. In the study of national trends in admission for aspiration pneumonia in the United States in 2002–2012, approximately 80% of patients with aspiration pneumonia were aged 65 years or older [7]. Furthermore, the length of hospital stay was longer, the overall total charge was higher and the mortality was increased in patients with aspiration pneumonia aged 65 years or older [7].
Dysphagia, which is a common disorder in the elderly [8], is also considered a risk factor for aspiration pneumonia [6,9,10]. It has been reported that approximately 15%–40% of the elderly population over 65 years is affected by dysphagia [11,12], and 55% of elderly adults 70 years and older diagnosed with pneumonia presented with clinical signs of oropharyngeal dysphagia [13]. Only 20% of older patients with aspiration symptoms exhibit normal swallowing function in a videofluoroscopic swallowing study (VFSS), and laryngeal penetration is identified in approximately 40% and aspiration in 20% [8]. A previous study reported that oropharyngeal dysphagia is closely related to community-acquired pneumonia in elderly subjects regardless of functional status and comorbidities [9]. According to a report by the Agency for Healthcare Research and Quality (AHRQ), it is estimated that approximately one-third of patients with dysphagia develop pneumonia [14]. Therefore, appropriate evaluation of swallowing function, including VFSS, should be provided to all elderly patients with clinical features related to dysphagia and pneumonia [10].
However, variables of VFSS that are valuable in estimating the risk of aspiration pneumonia in the elderly with dysphagia are unknown. Only one study investigated the findings of VFSS in patients older than 65 years with aspiration pneumonia, but specific parameters were not analyzed or compared with elderly individuals without aspiration pneumonia [15]. The present study aims to identify the variables of VFSS that are useful for predicting the risk of aspiration pneumonia in elderly patients with dysphagia.
MATERIALS AND METHODS
Subjects
The medical records and results of VFSS of a total of 251 elderly patients (aged 65 years or older) who were referred for VFSS due to symptoms suggestive of dysphagia in the period between July 2013 and April 2020 were reviewed retrospectively. The patients were excluded if they had (1) acute or subacute brain injury or stroke within 1 year; (2) cranial neuropathy or other acute neurological disorders that could affect swallowing function; (3) prior surgery in the pharyngo-laryngeal area; or (4) anatomical or structural abnormalities in the head and neck. Among the subjects, 133 patients were diagnosed with aspiration pneumonia (pneumonia group), and 118 patients did not exhibit any evidence of pneumonia (non-pneumonia group). The diagnosis of aspiration pneumonia was based on a clinical presentation consistent with pneumonia associated with a history of witnessed aspiration or risk factors for aspiration, which include impaired consciousness, history of seizure, age, antipsychotic medications, enteral feeding when associated with gastric dysmotility, poor cough, altered mental status, gastroesophageal reflux, poor oral care, and chronic obstructive pulmonary disease [2,3]. The clinical presentation of pneumonia was defined as two or more of the following symptoms or signs: fever (temperature, >38°C), cough, sputum production, shortness of breath, pleuritic chest pain, crackles, or consolidation on examination of the chest together with an acute pulmonary infiltrate evident on chest radiographs compatible with pneumonia [5].
VFSS
The VFSS was performed following the protocol described by Logemann [16] with minor modifications. The video images were recorded with lateral projection and stored digitally at a speed of 30 frames per second while the patients swallowed 3-mL boluses of various consistencies mixed with contrast medium in the seated position. In the authors’ dysphagia clinic, the order of the consistencies swallowed was three times swallowing of thick liquid (water-soluble barium sulfate diluted to 70%), two times swallowing of rice porridge, two times swallowing of curd-type yogurt, and three times swallowing of thin liquid (water-soluble barium sulfate diluted to 35%) followed by two times swallowing of drinking 5 mL of thin liquid from a cup. The VFSS was not performed if the patients could not cooperate or the medical condition of the patients was not stable enough for performing VFSS.
Analyses of VFSS
Video files of VFSS were reviewed and analyzed by a physiatrist who was experienced in VFSS reading without exposure to any clinical information. VFSS parameters associated with the swallowing process in the oral and pharyngeal phases, including the presence of penetration and aspiration, were analyzed. All the parameters of VFSS were defined according to Logemann’s protocol as described in Table 1 [17-20]. The severity of airway invasion was measured by the final version of the 8-point Penetration-Aspiration Scale (8PPAS) [20]. Residues in valleculae and pyriform sinuses were defined as clearly visualized barium lining in the pharynx after swallowing and graded into 4 levels—level 1 (none); level 2 (minimal), <10% of bolus; level 3 (moderate), from 10% to 50% of bolus; and level 4 (maximal), 50% of bolus [18]. Oral transit time (OTT) was measured as the time elapsed from the backward movement of the bolus until the bolus head reached the lower edge of the mandible [16]. Pharyngeal delay time (PDT) was measured as the time from the arrival of the bolus at the lower edge of the mandible until pharyngeal swallow was triggered [16]. Pharyngeal transit time (PTT) was measured as the time from the arrival of the bolus head at the lower edge of the mandible until the bolus tail passed through the cricopharyngeal region [16]. The longest time among the three swallowing of the thick liquid was selected for the time parameters. The vallecular and pyriform sinus residues were measured based on the largest amount of residue among all swallowing. Other abnormalities were judged to be present if they were observed at least once during the VFSS examination irrespective of consistency. The results were compared between the pneumonia and the non-pneumonia groups.

Definitions of VFSS parameters for evaluation of the swallowing process
Statistical analysis and study approval
Statistical analyses were performed using SPSS for Windows version 25.0 (IBM, Armonk, NY, USA). Categorical parameters were compared by Pearson chi-square test, and numerical parameters between the groups were compared by the independent t-test with the exception of ordinal variables for which the Mann-Whitney U test was used. Logistic regression analysis was performed for the parameters that exhibited significant differences between the pneumonia and the non-pneumonia group. Significance was accepted for p-values <0.05. The study protocol was approved by the Institutional Review Board of Dankook University Hospital (IRB No. 2020-07-005). The informed consent was waived.
RESULTS
The baseline characteristics of the subjects are presented in Table 2. More males were diagnosed with aspiration pneumonia (p=0.026). The mean duration between the onset of aspiration pneumonia and VFSS was 22.44±22.63 days. Most of the subjects underwent VFSS during hospitalization. The duration of mechanical ventilation was longer (p=0.040) and more tracheostomized patients (p=0.014) were noted in the pneumonia group.

Baseline characteristics
The mean 8PPAS scores of each viscosity are presented in Table 3. For the thick liquid and rice porridge, the mean 8PPAS score was significantly increased in the pneumonia group compared with the non-pneumonia group (p=0.004 and p=0.012, respectively).

Comparison of the 8PPAS between groups
The results of the VFSS parameters are presented in Table 4. For the time parameters, PDT and PTT were significantly prolonged in the pneumonia group compared with the non-pneumonia group (p=0.009 and p=0.025, respectively). The amounts of vallecular and pyriform sinus residue were greater in the pneumonia group compared with the non-pneumonia group (p=0.024 and p=0.008, respectively). The delay in swallowing reflex and the decrease in laryngeal elevation were more frequently observed in the pneumonia group (p=0.045 and p=0.011, respectively).

Comparison of VFSS parameters
To identify the significant variables for predicting the risk of aspiration pneumonia, logistic regression analysis was performed for the parameters that exhibited significant differences between the pneumonia and the non-pneumonia group. The results of logistic regression analysis showed that PDT (odds ratio [OR]=4.01; 95% confidence interval [CI], 1.267–12.703; p=0.018) and PTT (OR=3.63; 95% CI, 1.154–11.494; p=0.027) were significant predictors of aspiration pneumonia (Table 5).
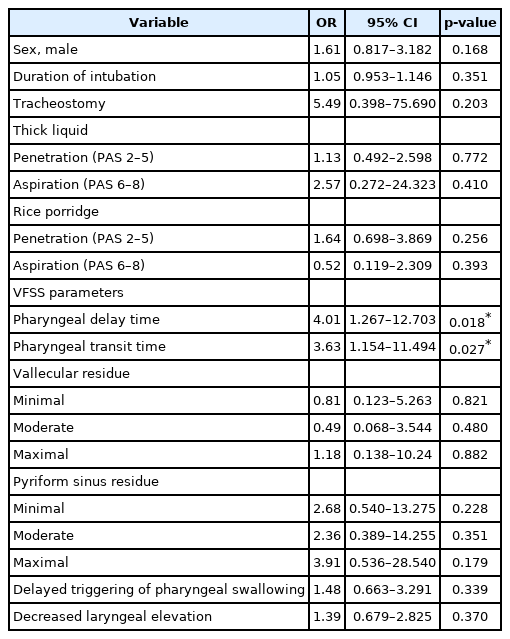
Logistic regression analysis for predicting aspiration pneumonia
DISCUSSION
Swallowing dysfunction often results in aspiration of oral or gastric contents, which can cause aspiration pneumonia [2]. Given its pathophysiologic characteristics, swallowing dysfunction is associated with various risk factors [7]. In a previous systematic review, age, male gender, dysphagia, dementia, angiotensin I-converting enzyme deletion genotype and use of angiotensin-converting enzyme inhibitors were identified as risk factors for aspiration pneumonia [6]. However, no difference was observed in the present study with the exception of the male preponderance in the pneumonia group. The difference was not observed likely because the pneumonia group was compared with patients with dysphagia symptoms not with the normal subjects.
The pneumonia group in the present study exhibited higher 8PASS with high viscosity boluses, such as thick liquid and rice porridge (p=0.004 and p=0.012, respectively). Previous studies have reported that swallowing function can be improved by increasing bolus viscosity in neurological patients and that the incidence of penetration and aspiration can be reduced [21,22]; however, the amounts of oral and/or pharyngeal residue and the risk of post-swallow airway invasion may also be increased [23]. The results of the present study suggest that a high-viscosity diet may not decrease the risk of aspiration pneumonia in patients with dysphagia. However, generalization of such speculation is limited because the control group in the present study consisted of subjects with symptoms of dysphagia that were not essentially normal.
In the present study, the PDT, representing the time interval for initiation of the swallowing reflex, was significantly delayed in the pneumonia group and revealed as a significant predictor. Logemann [16] stated that pharyngeal swallowing is initiated when laryngeal elevation begins. Kim et al. [24] emphasized the importance of appropriate timing of the hyolaryngeal elevation for the following reasons: (1) epiglottic closure can prevent premature bolus leakage of material into the laryngeal vestibule before initiation of pharyngeal swallowing and (2) continuous bolus movement through the pharynx into the esophagus can be accomplished through opening of the upper esophageal sphincter in a proper timing. Following this description, a longer pharyngeal delay time may indicate an increased risk of laryngeal penetration or aspiration.
The present study showed that PTT was also significantly delayed in the pneumonia group and another significant predictor. Previous studies demonstrated that prolonged PTT can increase the incidence of aspiration pneumonia in some patient groups, including stroke or Parkinsonism [25-28]. It seems that delayed PTT can increase the risk of aspiration pneumonia in the general elderly group as well as specific patient groups, such as stroke or Parkinsonism. In a previous case-control study, Almirall et al. [9] demonstrated that 91.7% of elderly patients with community-acquired pneumonia have oropharyngeal dysphagia using the volume-viscosity swallow test. In another study by Park et al. [15], 70 of 105 patients with aspiration pneumonia exhibited abnormal findings during the oral or pharyngeal phase or both in VFSS. The present study provided stronger evidence that oropharyngeal dysphagia can be more severe in patients with aspiration pneumonia using quantitative analysis for time parameters not attempted in previous studies.
The time parameters, such as OTT, PDT, and PTT, were prolonged in the non-pneumonia group as well as the pneumonia group, when referring to the normal range generally accepted (OTT <1.5 seconds, PDT <0.5 second, PTT <1.0 second) [16]. Prolongation of those time parameters suggests that the subjects in the non-pneumonia group also had milder forms of swallowing dysfunction; however, they did not have aspiration pneumonia. However, increased prolongation of PDT and PTT indicates that the pneumonia group exhibits more advanced dysphagia.
The pneumonia group also exhibited decreased laryngeal elevation more frequently (p=0.011). In normal individuals, when the pharyngeal swallow is triggered, the larynx elevates and moves anteriorly to tuck itself under the base of the tongue as a component of airway protection [16]. During swallow, the larynx elevates approximately 2 cm in normal young adult men [29]. Reduced laryngeal elevation can result in inability of the arytenoids to tilt anteriorly enough to make good contact with the epiglottic base, leaving the entrance to the airways lightly open, allowing penetration of the bolus into the airway entrance, and this penetrated material is typically aspirated after the swallow [16]. The residues in the valleculae and pyriform sinuses were significantly more abundant in the pneumonia group (p=0.024 and p=0.008, respectively). The greater amount of food residue along with the longer stay in the pharynx may contribute to the increased chance of aspiration to the lung [16].
This study has some limitations. The control group with normal swallowing function could not be recruited and compared due to ethical issues. However, proving the significance of dysphagia in the development of aspiration pneumonia was possible by comparing the pneumonia group with the non-pneumonia group with less severe dysphagia. Aspiration pneumonia was diagnosed by conventionally accepted criteria, but other causes of pneumonia could not be completely differentiated because the study was performed retrospectively. Patients with silent aspiration were included in the pneumonia group, but it is uncertain whether those patients were included in the non-pneumonia group. Discrepancy of patient configuration between groups may have affected the results. Although every effort was made to exclude secondary causes for dysphagia, a history of old neurological disorders could affect swallowing function. However, there was no significant difference in the proportion of underlying co-morbidities between the groups.
In conclusion, the present study delineated the findings of VFSS, suggesting an increased risk of aspiration pneumonia in elderly patients with dysphagia: delay of initiation of swallowing reflex, longer stay of bolus in the pharynx, greater amount of residue, and incomplete elevation of larynx. Increasing the viscosity of the diet may not be effective in reducing the risk of aspiration pneumonia in those patient group. Among the parameters, prolonged PDT and PTT were identified as significant predictors of aspiration pneumonia.
Notes
No potential conflicts of interest relevant to this article were reported.
Acknowledgements
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2018R1D1A3B07049300).
Notes
Conceptualization: Ko JY, Lee SJ. Methodology: Lee SJ, Ko JY, Sin DY. Formal analysis: Lee SJ, Ko JY, Hyun JK, Kim TU, Kim SY. Project administration: Lee SJ. Visualization: Lee SJ, Ko JY. Writing – original draft: Ko JY. Writing – review and editing: Lee SJ. Approval of final manuscript: all authors.