Factors Affecting Compliance With Weight-Bearing Restriction and the Amount of Weight-Bearing in the Elderly With Femur or Pelvic Fractures
Article information

Abstract
Objective
To determine the factors affecting the amount of weight-bearing during gait training in the elderly patients who underwent internal fixation after femur or pelvic fractures and how well they performed the weight-bearing restriction as directed by the physiatrist.
Methods
In this retrospective chart review study, we measured the amount of weight-bearing on the affected side in 50 patients undergoing internal fixation surgery and rehabilitation after femur or pelvic fracture using a force plate. Patients receiving non-weight-bearing or partial weight-bearing education were considered to perform weight-bearing restriction well when the amount of weight-bearing was <50 lb. Furthermore, regression analysis was performed to determine the effects of postoperative complications, age, cognitive function, and pain on weightbearing restriction.
Results
Variables affecting the amount of weight-bearing were age (r=0.581, p<0.001), weight-bearing education type (r=0.671, p<0.001), manual muscle strength of hip flexion on the non-affected side (r=-0.296, p=0.037), hip abduction (r=-0.326, p=0.021), knee extension (r=-0.374, p=0.007), ankle plantar flexion (r=-0.374, p=0.008), right hand grip strength (r=-0.535, p<0.001), Korean version of Mini-Mental State Examination (r=-0.496, p<0.001), Clinical Dementia Rating (r=0.308, p=0.03), and pain visual analog scale scores (r=0.318, p=0.024). The significant predictor of the amount of weight-bearing among these variables was age (β=0.448, p=0.001). The weight-bearing restriction adherence rate was significantly lower, at 22%, for patients aged ≥65 years as compared to 73% for those <65 years.
Conclusion
Age was a major variable affecting the amount of weight-bearing. Compliance with weight-bearing restriction was significantly lower in patients aged ≥65 years than in patients <65 years.
INTRODUCTION
In the United States, an estimated 258,000 hip fractures occurred in the elderly in 2010, and approximately $17– $20 billion was paid for the management of hip fracture patients in 2010 [1]. According to multicenter and cohort analysis studies reported in Korea in 2014, the initial age of hip fracture among the Korean elderly population is 79 years, and fractures occur within 9.2–30.2 months after the first fracture [2-5]. As life expectancy increases, the hip fracture incidence is expected to increase as well. By 2030, the number of hip fractures in the United States is expected to increase to 289,000 [6].
The clinical effect of controlling postoperative weightbearing in rehabilitation after lower limb fractures remains controversial. There is a clear recommendation for early weight-bearing after lower limb fracture, since there is an apparent advantage that early weight-bearing improves bone turnover metabolism and promotes bone growth [7,8]. In a similar perspective, prolonged nonweight-bearing is associated with the occurrence of delayed bony union and worse functional recovery [9].
To date, however, the relationship between the amount of weight-bearing and weight-bearing time as well as bone mineral density or functional recovery is not wellknown [10]. A study reported that too heavy weight-bearing at the initial stage after surgery may adversely affect the surgical and reconstructive outcome stability [11]. Some suggested that weight-bearing should be restricted for 2–6 weeks depending on the fracture site [12].
Hoyt et al. [11] reported that although there are differences on the fracture site and operation method, partial weight-bearing or non-weight-bearing postoperatively is usually performed in the rehabilitation stage for patients with lower extremity fracture and reconstructive surgery. In general, patients were encouraged to perform early mobilization and to gradually increase their weightbearing until they attain full weight-bearing.
A study used instrumented hip implants specially designed for weight-bearing after fracture [13], but the literature and rationale for the weight-bearing time and extent is not clear [14]. Therefore, based on continuous X-ray radiographic examinations, we observed changes in the surgical site such as in the fracture site gap, alignment, displacement, and callus formation. Rehabilitation was subsequently performed based on the experience of the physiatrist. This physiatrist-recommended weightbearing is a key component in the load and rehabilitation process of the fracture site [15]. However, in the clinical setting, it is difficult to know how much weight-bearing is performed by the patient during the treatment process and whether the weight-bearing is achieved as recommended by the physiatrist.
The purpose of this study was to determine the factors affecting the amount of weight-bearing in the gait rehabilitation process especially in the elderly patients who underwent internal fixation after a femur or pelvic fracture and how well they performed the weight-bearing restriction as directed by the physiatrist.
MATERIALS AND METHODS
Study patients and setting
A retrospective chart review was performed to evaluate patients who received rehabilitation treatments after sustaining lower extremity fractures at one university hospital between August 2017 and April 2019.
Patients who underwent internal fixation after a femur or pelvic fracture, were evaluated for the measurement of the amount of weight-bearing on the affected side using a force plate after approximately 30 days of surgery, and who received gait rehabilitation therapy in the Department of Rehabilitation Medicine were included. Patients with multiple traumatic injuries, upper extremity fractures, and lower extremity fractures other than those of the femur or pelvis were excluded from this study. This study was approved by the Institutional Review Board of Chungbuk National University Hospital (No. 2017-04-009). The informed consent was waived.
Patient evaluation and data acquisition
Considering the elderly hip fracture complications, such as deep vein thrombosis, nerve injury, and delirium [16], the variables that could affect the amount of weight-bearing were selected, namely lower extremity edema, peripheral nerve injury, Clinical Dementia Rating (CDR), Korean version of the Mini-Mental State Examination (K-MMSE), and Hamilton Depression Inventory (HDI). In addition, fracture site, body mass index (BMI), days since surgery and rehabilitation, visual analog scale (VAS) scores, age, sex, hand grip, and lower extremity strength, which were expected to affect weight-bearing, were added.
We performed a retrospective review of medical records of our clinical series of patients; their baseline characteristics included age, sex, BMI number of days since surgery and rehabilitation, fracture sites (femoral neck, intertrochanteric, subtrochanteric, femoral shaft, and pelvis), weight-bearing education types (none, partial, full), manual muscle strengths (hip flexion, hip abduction, knee extension, and ankle plantar flexion), hand grip strength, K-MMSE, CDR, VAS, HDI and peripheral nerve injuries, and lower extremity edema.
In addition to the above mentioned evaluation, all patients underwent rehabilitation therapy consisting of weight-bearing exercises, strengthening exercises, gait training, aerobic exercise, and functional training once a day for 30 minutes under the supervision of the physical therapist. The physiatrist determined the degree of weight-bearing, non-weight-bearing, partial weightbearing, and full weight-bearing in gait training based on X-ray radiography (fracture site stability, callus formation) and physical examination (manual muscle test).
After more than 3 weeks of gait training, the amount of weight-bearing on the affected side was measured. We used a force plate (HWK-200RT; Motion Analysis, Rohnert Park, CA, USA) to measure the amount of weight-bearing with walker gait. The force (newton, N) applied to the force plate in real time was checked via the monitor. The maximum peak force on the affected side was measured thrice and the mean value was used for the analysis (Fig. 1).
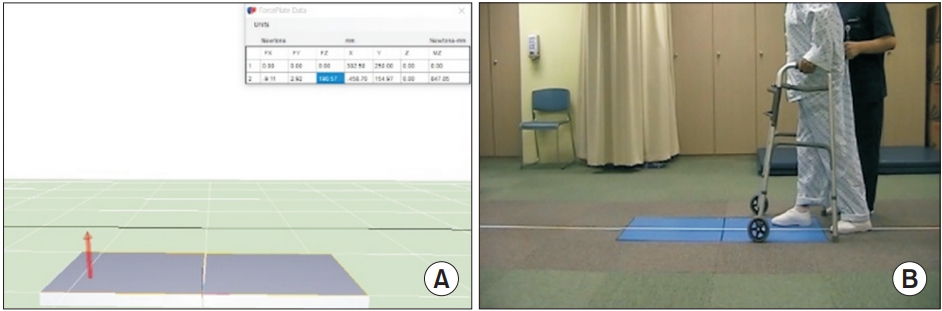
The maximum peak force on the affected side of the patient is measured through the force plate. (A) Real-time peak force measurement and (B) image of a patient walking.
Partial weight-bearing definition
To determine the partial weight-bearing specific criteria, we asked four physical therapists to apply the force plate test and perform two instructional tasks: toe-touch weight-bearing with walker and 20% partial weight-bearing with walker. A total of 95 and 84 measurements were taken for the toe-touch weight-bearing and 20% partial weight-bearing, respectively. In the toe-touch weight-bearing task, the mean weight-bearing was 103.1±66.9 N, 14.3%±9.1% (body weight percentage), and in the 20% partial weight-bearing task, the mean weight-bearing was 225.9±88.9 N, 30.6%±9.3%. The mean weight-bearing of 225.9 N (22.59 kg) in the 20% partial weight-bearing task was almost equivalent to the maximum weight load of 50 lb (22.67 kg) for 12 weeks after femur or pelvis internal fixation operation [17]. Therefore, we performed gait training for toe-touch weight-bearing in partial weight-bearing gait training to lower the amount of weight-bearing to less than 50 lb. The cutoff value for whether the 20% partial weight-bearing training was well performed was set to 50 lb (approximately 226 N); patients with weight-bearing greater than 50 lb, despite partial weight-bearing gait training, were considered overweight-bearing and not adequately weight restricted.
Statistical analysis
To analyze the factors affecting the amount of weightbearing, the Pearson correlation coefficient and multivariate linear regression analyses were performed, and the body weight percentage was used as the amount of weight-bearing. To analyze the difference in adherence to weight-bearing restriction according to age, the chisquare test was performed. A cutoff value of 50 lb, which was the mean weight-bearing in the 20% partial weightbearing task of four physical therapists, was used for analysis of adherence to weight-bearing restriction. In the adherence analysis, only patients with partial weightbearing and non-weight-bearing education were included. All statistical analyses were performed using the SPSS version 25.0 for Windows (IBM Corp, Armonk, NY, USA), with a p-value of <0.05.
RESULTS
Patients’ baseline characteristics
Ninety-three patients who received rehabilitation treatments after sustaining lower extremity fractures at one university hospital between August 2017 and April 2019 were evaluated. Fifty patients were included in this study based on the inclusion and exclusion criteria mentioned in the methods section. Twenty-nine (58%) were males and 21 (42%) were females, and the average age was 70.3±16.2 years. The force plate test was performed on an average of 38.2±17.7 days postoperatively. The most frequent fracture was the intertrochanteric fracture in 25 patients (50%) followed by the pelvic fracture in 14 patients (28%). The most frequent weight-bearing education type was partial weight-bearing with 25 patients (50%). CDR was categorized as normal cognition or questionable dementia in most patients with 0 point (26 patients, 52%) or 0.5 point (20 patients, 40%) (Table 1). The amount of weight-bearing according to weight-bearing education type is presented in Table 2.

Baseline characteristics of the patients (n=50)

Amount of weight-bearing according to weight-bearing education type
Factors associated with the amount of weight-bearing
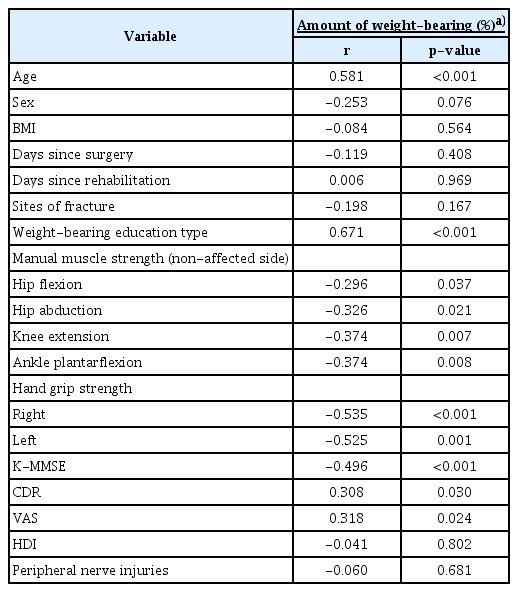
Age, weight-bearing education type, CDR, and VAS showed positive correlation with the amount of weight-bearing, whereas lower extremity strength on the nonaffected side, both hand grip strengths, and K-MMSE revealed negative correlation with the amount of weightbearing (Table 3).
Factors associated with the amount of weight-bearing
In the multivariate linear regression analysis with seven variables related to the amount of weight-bearing, only two variables, age and weight-bearing education type (none, partial, full) were statistically significant predictors for the amount of weight-bearing (Table 4). The standardized coefficients of weight-bearing education type were 0.418 and the p-value was 0.002. Moreover, the standardized coefficient of age was 0.448 and the p-value was 0.001.

Multivariate linear regression analysis for predictors of the amount of weight-bearing
Difference in adherence to non-weight-bearing or partial weight-bearing according to age
To analyze the difference in adherence to weight-bearing restriction according to age, we divided the patient group into two groups, <65 years and ≥65 years. Significant differences in the proportion of patients who had received non-weight-bearing education were not observed between the two groups. The amount of weight-bearing of patients who were instructed to perform partial weight-bearing or non-weight-bearing was checked if it was <50 lb to confirm the rate of adherence to the weight-bearing restriction. There was a statistically significant low adherence rate of approximately 22% in patients ≥65 years (p=0.002); however, the adherence rate was about 73% in patients <65 years (Table 5).

Difference in adherence to non- or partial weight-bearing according to age
DISCUSSION
It is generally common to train patients on a specific weight-bearing protocol depending on their clinical conditions, because it helps to heal and restore the fracture site [18]. Furthermore, postoperative weight-bearing restriction in older patients with hip fractures has been generally performed in the clinical practice [19], and was considered an appropriate option in the 2015 OrthoGuidelines of the American Academy of Orthopedic Surgeons [20]; however, it is very difficult for the patient to be trained to achieve the desired weight-bearing [12]. In this study, on average, 30.6%±9.3% weight-bearing was measured even if the trained physical therapists were ordered 20% partial weight-bearing in the force plate test. This suggests how difficult weight-bearing restriction is for the patient. In this study, the amount of weight-bearing of patients with non-weight-bearing education type was 22.8%±19.1%, partial weight-bearing 51.3%±19.1%, and full weight-bearing 73.3%±17.1%, respectively (Table 2).
An analysis of this study, which identified the factors affecting the amount of weight-bearing of patients, in addition to the weight-bearing education type showed that age, lower extremity strength on the non-affected side, bilateral hand grip strength, K-MMSE, CDR, and VAS were identified. However, in the multivariate linear regression analysis of these variables, only age was identified as a statistically significant variable to account for the amount of weight-bearing in addition to the weight-bearing education type. Decreased physical and cognitive functions as well as reduced peripheral nerve sensory feedback may be factors that account for the increased amount of weight-bearing of patients with aging [21]. Because of this change in physical and cognitive functions with aging, muscle strength and cognitive function did not appear to have a direct effect on the amount of weight-bearing in this study.
Age was assessed as an important variable in the amount of weight-bearing, and we divided the patients into two groups, <65 years and ≥65 years, to determine the difference in the rate of adherence to weight-bearing restriction according to age. The percentage of patients who performed well weight-bearing restriction <50 lb was much higher, at 73%, in patients aged <65 years as compared to the 22% in patients ≥65 years, among patients trained with non-weight-bearing or partial weight-bearing. This means that compliance with the weight-bearing restriction is much lower in patients aged ≥65 years. In an additional analysis, the adherence rate was 5% in patients aged ≥75 years and significantly lower than 75% in patients <75 years. Therefore, the compliance with weight-bearing restrictions under the supervision of medical staff in hospitals is low. Obviously, the compliance with weight-bearing restriction is much lower in the absence of medical staff supervision in the environment outside the hospital [22].
As we have seen so far that clinically, compliance with weight-bearing restriction is low [12], and especially much lower in patients aged ≥65 years. Despite this low compliance, complications, such as implant failure, nonunion, and delayed-union are very rare [15]. A study on large populations showed that the non-union probability after a femur or pelvic fracture increased at age ≥85 years, but the probability decreased more in patients ≥65 years old than in those <65 years [23]. Therefore, in the rehabilitation of patients aged ≥65 years, a more active training and management system will be needed for specific patients with higher risk, such as those with fracture site instability or large amount of fracture gap, non-union, and malunion, which is more individualized than overall weight-bearing restriction, which is less feasible.
This study has some limitations. First, despite the retrospective nature of the study, the number of patients included in the study was only 50. Fifty patients are not very sufficient for multiple linear regression analysis with seven independent variables [24]. This is because of the limited number of patients who underwent internal fixation, mainly weight-bearing restriction, among femur and pelvic fracture patients who were transferred to the department of rehabilitation medicine. Second, a force plate was used to measure the amount of weight-bearing on the affected side of the patient, but this is an instantaneous measurement rather than a continuous measurement. If a continuous measurement was feasible, it would have been clinically more meaningful. Third, cognitive function is thought to influence the compliance with weight-bearing restriction clinically, but the multivariate linear regression analysis of this study shows that cognitive function does not directly affect the amount of weight-bearing. This may be because the number of patients with low cognitive function was very small, i.e., of the 50 patients, 26 (52%) were normal, 20 (40%) had questionable dementia, and only 4 (8%) had mild dementia [25]. Finally, we did not perform the analysis according to the difference of operation method for femur fracture. Among 36 patients with femur fracture, 33 patients received proximal femoral nail anti-rotation surgery and only 3 patients received screw fixation surgery. Further comparative studies will be needed with a more large-scale patient population.
In conclusion, age is a major variable affecting the amount of weight-bearing, and compared with patients <65 years, compliance with weight-bearing restriction was significantly lower in patients ≥65 years. This study suggests the need for further investigation, and questions the gait rehabilitation therapy validity based on an overall weight-bearing restriction, which has low feasibility. A large-scale prospective study of compliance with weight-bearing restriction according to age and related side effects and clinical outcomes is needed. In addition, the result of this study suggests that a new rehabilitation technique may be needed to control weight-bearing in the elderly patients with lower extremity fractures.
Notes
No potential conflict of interest relevant to this article was reported.
Conceptualization: Lee GJ, Seo HS. Methodology: Lee GJ, Seo HS, Shon HC. Formal analysis: Lee GJ, Seo HS, Cho HG, Oh MW, Lee CJ. Funding acquisition: Lee GJ. Project administration: Lee GJ, Seo HS. Visualization: Lee GJ, Seo HS, Lee CJ. Writing – original draft: Seo HS, Lee GJ. Writing – review and editing: Seo HS, Lee GJ, Kong HH. Approval of final manuscript: all authors.