Effectiveness of Active Rehabilitation Program on Sports Hernia: Randomized Control Trial
Article information

Abstract
Objective
To determine whether an active rehabilitation program that involves repetitive effortful muscle contractions, including core stability, balancing exercises, progressive resistance exercises, and running activities, after a sports hernia, is effective.
Methods
Forty soccer players with sports hernias were randomly divided into two equal groups: group A (active rehabilitation program) and group B (conventional treatment). The methods of assessment included a visual analog scale (VAS) and hip internal and external range of motion assessments. Group A received conventional treatment (heat, massage, transcutaneous electrical nerve stimulation, and mobilization) plus an active rehabilitation program, while group B received only conventional treatment. Three treatment sessions were given each week for 2 months. Evaluations were performed pre- and post-treatment.
Results
A decrease in VAS was seen in both groups at the end of treatment, 80.25% in group A and 41.93% in group B. The difference between the two groups was statistically significant (p=0.0001), whereas there were no statistical differences in internal and external rotation between the groups at the end of treatment (p>0.05). After treatment, an improvement in outcome measures of group A compared to group B (p=0.01) was seen. Thirteen patients in group A and only three patients in group B returned to sports activities without groin pain.
Conclusion
Active rehabilitation was effective for sports hernia management measured by a decrease in pain and the return to sports.
INTRODUCTION
Hip and groin pain is problematic for athletes, particularly in sports involving high amounts of running, changes in direction and kicking [1]. Gilmore reported that sports hernias were present in 59% of patients who participated in soccer, 10% of rugby, 4% of racquet games, 4% of athletics, 2% of cricket, 2% of hockey, and 19% of alternative sports players [2], while in the United States, sports hernias were observed in 46% of patients who participated in soccer, 17% of hockey, 13% of football, and 24% of different sports, including swimming, tennis, basketball, and golf [3].
A sports hernia is a painful condition, noted for soreness and sharp pain at the groin area near the pubic tubercle at the onset. The symptoms reflect injuries to the outer inguinal ring, which becomes dilated with posterior wall deficiency of the inguinal canal (fascia transversalis,) and tears in the conjoint tendon [4]. Different hypotheses explain the possible causes of pain in sports hernia, including posterior wall distension can contribute for torn of conjoint tendon. It was proposed that outer inguinal ring dilation caused by tearing of the external oblique aponeurosis, in addition to conjoint tendon laceration, leading to impairment and fragility between the inguinal ligament and the conjoint tendon [5]. Others have suggested that either the ilioinguinal or genitofemoral nerve entrapment could give rise to the pain [6,7]. Entrapment of the ilioinguinal nerve caused by a hernia of the external oblique aponeurosis is called hockey groin [8]. However, nerve entrapment or stretching is, evidently, not the only reason for sports hernia pain because it is indistinguishable from nerve stretching experienced by athletes with torn conjoint tendons.
The expression of a sports hernia includes many structural abnormalities along with a set of secondary causes. The most commonly hypothesized cause is that sports hernias occur secondary to intensive hip muscle contractions and excessive use of flexion, extension, abduction, and adduction moments across the hip joint with twisting or hyperextension of the trunk during sports, leading to exaggerated movement of the pelvis that creates a shearing force over the symphysis pubis [9,10]. The force is further exaggerated by the imbalance between the two opposing forces acting on the pubis, the upward and oblique dragging of the abdominal muscles from one side and the downward and lateral dragging of the adductors on the other side. This disequilibrium of forces can cause injuries to both the abdominal and hip adductors [11]. The traction of hip adductors against the non-moving lower limb may generate shearing forces across the hemipelvis and has been considered an additional cause of sports hernias [12].
Therefore, the ideal functional stability of the groin can be lost by this disequilibrium between the abdominal and hip muscles. Thus, a vigorous off-season conditioning program that puts more emphasis on strengthening the lower limbs, while ignoring the abdominal muscles, may lead to a pelvic balance disturbance and shortening of the hip flexors and adductors, which increase the opportunity for sports hernia development [8].
The diagnosis of sports hernias should include at least three of these five clinical findings: (1) tenderness at the insertion of the conjoint tendon, (2) tenderness at the inner inguinal ring, (3) dilated superficial inguinal ring without clinical signs of a hernia but with painful points at the hip adductors attachment, (4) hip adductor longus muscle pain at its origin, and (5) widespread inguinal distress extending to the perineum and femoral interior surface and intersecting the midline [13].
Management of sports hernias usually follows different strategies which depend on combined treatments encompassing medications, surgical interventions, and physical therapy [14,15]. Non-surgical intervention is the first recommended treatment and includes rest (6 to 8 weeks), NSAIDs, ice packs, massage, and exercises [12]. Limitations in hip range of motion (ROM) have been reported in athletes suffering from groin pain [16] as with the chronicity of sports hernias, there is a decrease in hip ROM for external and internal rotation [17]. It has been hypothesized that the hip-joint capsular twisting performed during participation in Australian Rules Football may produce movement restrictions like those created at the glenohumeral joint by repetitive throwing [18]. Restricted joint mobility can be managed with joint mobilization of the proper part of the joint capsule, usually the posterior, inferior, and lateral parts [19], and stretching is also commonly used during rehabilitation to decrease joint stiffness and increase ROM [20]. Vigorous exercises or stretching used in an attempt to increase the hip ROM should be avoided to prevent excessive pain [21].
Physical rehabilitation programs for sports hernias should mainly include core stabilization, strengthening of the hip adductors and abdominal muscles, balancing, and postural training exercises [12,19,21]. Core strength exercises involving muscle strengthening and balancing exercises are always used to reinforce and strengthen abdominal and pelvic muscles [22] because these muscles play a significant role in improving muscle flexibility, lumber stability, and body balance [23]. Several studies have reported the importance of core stability and its effects to prevent sports injuries and improve athletic activity and performance through inhibition of false motion patterns and the maintenance of good postural alignment [24].
Active physical training aiming to strengthen hip adductors and abdominal muscles and improve endurance, balance, and coordination between the hip and trunk muscles was found to be an effective method for sports hernia management [25]. In a randomized experimental study comparing active physical training and passive therapy in athletes with groin pain, active exercise training was found to be more effective and have greater benefits to return of athletes to their pre-injury activity levels faster [26].
Rehabilitation and exercise therapy for sports hernias usually depends on the past experience of the therapist rather than on an integrated protocol [14,15]. Therefore, this study was designed to evaluate the efficacy of active rehabilitation for the management of sports hernias.
MATERIALS AND METHODS
Subjects
Forty soccer players diagnosed with sports hernias participated in this study. The diagnosis was made by magnetic resonance imaging, which revealed disruption of the distal rectus abdominis/adductor aponeurosis, and was correlated with information provided from the patient’s medical history and physical examination. The athletes complained of a dull and diffuse pain in the groin, radiating to the lower abdomen and proximal thigh. The pain was worsened by coughing, sneezing, or other Valsalva-type maneuvers. During the examination, the abdominal obliques, transversus abdominis, conjoint tendon/rectus abdominis, and adductor longus were palpated. The diagnosis of sports hernias should include at least three of these five clinical findings: (1) pinpoint tenderness over the pubic tubercle at the point of insertion of the conjoint tendon, (2) palpable tenderness over the deep inguinal ring, (3) pain and/or dilation of the external ring with no obvious hernia evident, (4) pain at the origin of the adductor longus tendon, and (5) dull, diffuse pain in the groin, often radiating to the perineum and inner thigh or across the midline. Two special tests were done to confirm the diagnosis, resisted sit-ups and single or bilateral resisted leg adduction tests. To be included in the study, the athletes had to be male, aged 18–25 years, have groin pain for at least 2 months due to playing sports, and exhibit at least three of the five clinical findings mentioned above. The exclusion criteria included a palpable inguinal or femoral hernia; evidence of lumbar radiculopathy; sacroiliac dysfunction; nerve entrapments of the ilioinguinal, genitofemoral, or lateral femoral cutaneous nerves; hip joint disorders, such as osteoarthritis, osteochondritis dissecans, and bursitis; and femoroacetabular impingement.
Design
The study was a single-blinded randomized controlled clinical trial and was approved by the ethical committee of the Faculty of Physical Therapy, Cairo University. All patients provided informed consent before participating in the study. After inclusion, the patients were randomly divided into two equal groups. The randomization process was applied using the envelope method. Cards on which either ‘conventional treatment’ or ‘active rehabilitation program’ was written on them were sealed in envelopes. The envelopes were given to a staff physical therapist who was blinded to this study and she/he picked one envelope. Depending on the card selected, the participants were allocated to their respective group. Appointments to begin the allocated treatment were arranged and treatment was started within one week of randomization. The examining physical therapist was not involved in the randomization process and remained unaware of the treatment allocation. Athletes were instructed not to reveal their treatment allocation to the physical therapist during their assessment.
Treatment
All patients were evaluated before and after the end of the treatment. The visual analog scale (VAS) was used for pain assessment and a goniometer was used to assess the ROM of the hip internal and external rotation. Pain was assessed with Valsalva’s maneuver, forcibly exhaling against a closed airway, and with a resisted sit-up and the mean was determined. Hip internal and external rotations were measured in the supine position with the hip and knee at 90° flexion.
After the end of the treatment, the outcome measures of successful treatment were evaluated. Successful treatment was defined as no pain at palpation of the adductor tendons and the adductor insertions at the pubic bone and no pain during active adduction against resistance, no groin pain in connection with or after athletic activity in the same sport and at the same level of competition as before the onset of the groin pain, and return to the same sport and at the same level without groin pain. If all three measures were reached, the result was labeled excellent, if two measures were reached, the result was good, if one measure was reached, the result was fair, and if no measures were reached, the result was poor.
In this study, both groups received conventional treatment as described in Table 1. Conventional treatment included heat, transverse friction massage, transcutaneous electrical nerve stimulation (TENS) and mobilization. Both groups were instructed to perform stretching exercises included in the treatment program for the adductor, hamstring, and hip-flexor muscles on the days between the treatment days.
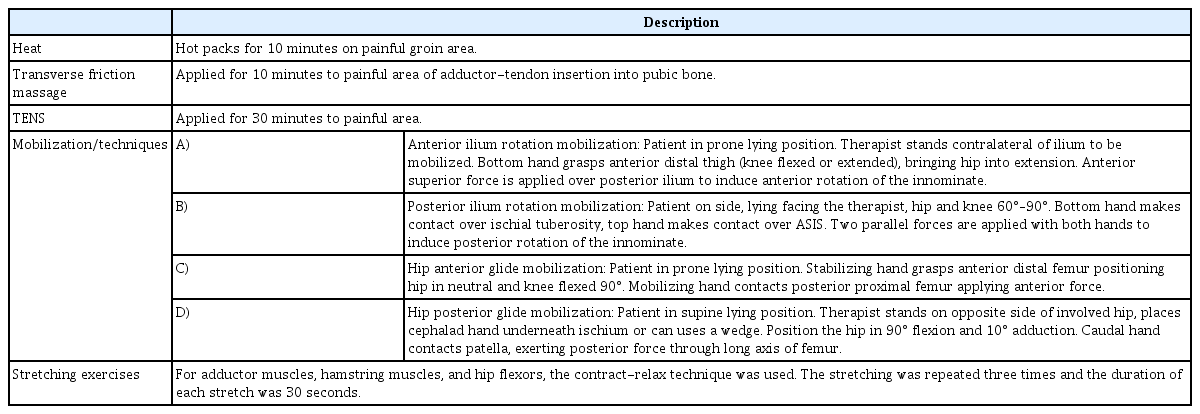
Conventional treatment program
In addition, participants in group A received an active rehabilitation program, which included strengthening exercises for the hip and abdominal muscles, core stabilization, and balancing exercises (Table 2). The patients were instructed to perform the exercises included in the treatment program on the days between the treatment days.

Active rehabilitation program
Patients in both groups were not allowed to receive any other treatments for groin pain during the study period. Patients in both groups were instructed to return to a running program at the sixth week of the study, which progressed from slow jogging to straight sprints and finally ended with cutting. The progression of exercise was performed in the absence of pain during exercise, the acquisition of functional control, and the ability to complete a functional exercise or a set number of repetitions of an exercise.
Statistical analyses
Descriptive statistics and t-tests were conducted for the comparison of subject characteristics between the groups. t-tests were conducted to compare the mean values of VAS and ROMs between both groups and paired t-tests were conducted to compare the pre- and post-treatment mean values of the measured variables in each group. Chi-square tests were conducted to compare outcome measures between the groups. The level of significance for all statistical tests was set at p<0.05. All statistical tests were performed using the Statistical Package for Social Sciences (SPSS) version 19 for Windows (IBM SPSS, Armonk, NY, USA).
RESULTS
A diagram of the study randomization is shown in Fig. 1. A total of 55 male patients were admitted and assessed for eligibility. Fifteen of them were excluded because they did not meet the eligibility criteria, while 40 patients were found to be eligible to participate in the study. All patients completed the treatment program without withdrawal.
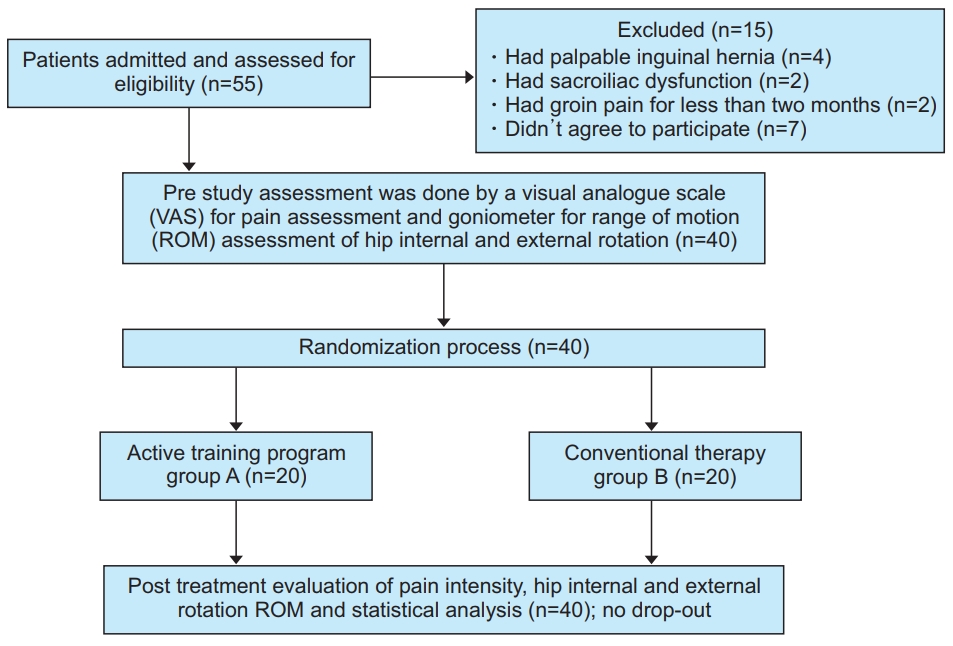
Participant flowchart.
Demographics
The mean±standard deviation for age, weight, and height of group A were 26.2±2.94, 71.05±2.7, and 169.9±3.3 and the values for group B were 26.75±3.02, 70.45±3.21, and 170.15±3.77, respectively. There was no statistical difference between the groups (p=0.56, p=0.52, and p=0.82, respectively).
Within-group comparison
The results showed a statistical decrease in VAS after treatment in group A and B compared to the pre-treatment scores (p=0.0001). The percent decrease in VAS of group A and B were 80.25% and 41.93%, respectively.
There was a statistical increase in internal and external rotation ROM after treatment in group A and B compared to pre-treatment (p=0.0001). The percent increase in internal and external rotation ROM of group A and B were 22.18%, 17.32%, 23.45%, and 16.24%, respectively.
Comparison between groups
The results showed no statistical difference between the groups in VAS, internal rotation, or external rotation ROM before treatment (p>0.05). There was a statistical decrease in the VAS of group A compared to group B (p=0.0001), while there was no significant difference in internal and external rotation ROM between the groups after treatment (p>0.05) (Table 3). There was an improvement in outcome measures of group A compared to group B after treatment (p=0.01) (Table 4).

Comparison of VAS, internal rotation, and external rotation ROM between groups A and B pre- and post-treatment

Comparison of outcome measures between groups A and B
DISCUSSION
Sports hernias are more common in athletes who are engaged in sports requiring highly repetitive booting and twisting movements [27]. The exact progression of sport hernia development is still unknown but a combination of several factors may play roles in its development, including balance disturbances between the hip adductors and abdominal muscle power, impairment of the hip ROM, and lack of hip adductors flexibility with repetitive shear force on their attachments at the pelvis [4].
A systematic review of the effectiveness of exercise therapy for groin pain management in athletes concluded that exercise therapy was a key factor in rehabilitation [15]. However, in another review by Swan and Wolcott [28] concerning the diagnosis and operative findings of sports hernias, the authors concluded that surgical interventions provided results that were superior to conventional therapy. Other studies have recommended conventional therapy, including physical rehabilitation with manual therapy for 6 to 8 weeks as the first choice of treatment [29], followed by operative repairs if physical rehabilitation failed and the athlete did not return to pre-injury levels [30,31].
Our study included 40 soccer players with sports hernias who were divided into two equal groups. Both groups received conventional treatment (heat, massage, TENS, and mobilization), while the study group received an active rehabilitation program. The treatment period lasted 2 months. After the end of treatment, VAS decreased in groups A and B to 80.25% and 41.93%, respectively. The significant difference in VAS between the groups (p=0.0001) can be attributed to the effect of the active rehabilitation program which aimed to increase strength, pelvic stability, and coordination, and correct the biomechanical abnormalities developed from practicing soccer, which may lead to stress and repetitive trauma to the anatomical structures of the pelvis, subsequently causing pain.
Hip internal and external rotation ROM increased in both groups but there was no statistical difference between the groups after treatment. The improvement in ROM in both groups may be due to decreased pain, stretching exercises, and mobilization techniques which were applied to both groups. However, the post-treatment outcome measures were improved in group A compared to group B (p=0.01). Thirteen patients in group A and only three patients in group B returned to sports activities without groin pain. We believe that core strengthening and balancing exercises played a significant role in the faster return of sportsmen to full activity, hence we suggest that improvement in the target group was due to the type of exercises used.
Several case reports/series have described a proposed rehabilitation protocol for inguinal disruption. Woodward et al. [30] described a three-phase rehabilitation protocol for sports hernia management in a hockey player with groin pain, which included electrotherapy, hydrotherapy, pain modalities, balancing, and strengthening rehabilitative exercises for the trunk, abdominal and hip muscles. By the end of the study, the patient experienced no pain at rest or during activities and was able to return to a full level of activity in National Hockey League competitions for 7 years.
Yuill et al. [17] reported that non-surgical management of chronic groin pain, including electrotherapy, pain modalities, and physical rehabilitation exercises for eight weeks increased the muscle power and balance of both the hip and abdomen. By the end of the study, all patients returned to their activities without the recurrence of symptoms at a 2-year follow-up.
Holmich et al. [26] concluded that a rehabilitation program that utilized active exercises could provide an injured athlete with over 10 times the potential to return to active sports. They found that the outcomes of a rehabilitation program that involved active exercises were much better than a passive program. The study found that 79% of the athletes treated with an active program were able to return to pre-injury status after a seven-month follow-up, compared to 14% of athletes treated with a passive program.
There were similarities between these former studies and this study. In the first two studies, the treatment used was a combination of passive and active training programs. The passive program consisted of manual therapy and electrotherapy, while the active training program was directed toward improving strength, core control, coordination, and correcting pelvic muscle imbalance. The latter study compared a passive program with an active training program to treat long-standing groin pain. The results agreed with our results, that active training program was very effective in treating groin pain.
In another case study, rehabilitation of the lower abdominal groin pain was done by structured core muscle retraining. The sportsman was a golfer and the exercise program utilized a stepwise progression in order to increase stability and neuromuscular control. The patient was able to return to the complete practice of golf after four weeks of treatment [27]. The athlete in that study returned to sports in much less time than those in our study. The similarity here was the use of exercises that improved core strength and pelvic stability, indicating their importance in the management of sports hernia.
Sports hernias are usually part of a much wider and serious inguinal disruption injury. Moreover, sports hernias can be caused by many diverse causes which may affect the selection of effective conservative treatment and is considered a limitation of our study. Our study was also limited by small sample size, the absence of muscle strength assessments of the abdominal and adductor muscles, which may have enabled better statistical analysis, and the larger amount of treatment time allocated to the treatment group than the control group. In future studies, a follow-up study is necessary to reveal long-term results and recurrence rates.
In conclusion, the results of this study showed that active exercises were a very essential part of sports hernia rehabilitation. An active rehabilitation program was effective for sports hernia management, resulting in decreased pain and a return to sports.
Notes
No potential conflict of interest relevant to this article was reported.
Conceptualization: Abouelnaga WA. Methodology: Abouelnaga WA, Aboelnour NH. Formal analysis: Aboelnour NH. Funding acquisition: None. Project administration: Abouelnaga WA. Visualization: Aboelnour NH. Writing – original draft: Abouelnaga WA, Aboelnour NH. Writing – review and editing: Aboelnour NH, Abouelnaga WA. Approval of final manuscript: all authors.