A Dynamic Magnetic Resonance Imaging Study of Changes in Severity of Cervical Spinal Stenosis in Flexion and Extension
Article information

Abstract
Objective
To evaluate changes in the severity of cervical spinal stenosis (CSS) in flexion and extension and determine whether the rate of change with motion varied with severity.
Methods
The study included 92 symptomatic patients with a mean age of 57.80±10.41, who underwent cervical spine dynamic magnetic resonance imaging. The severity of stenosis was evaluated using a semi-quantitative CSS score, ranging from 0 (no spinal stenosis) to 18 (severe stenosis). Radiological evaluation included flexion, neutral, and extension measurements, as determined by the C2–C7 Cobb angle. The severity of stenosis was represented by the total CSS score. The total CSS score in flexion, neutral, and extension positions was compared using repeated measures one-way analysis of variance. The change rate of stenosis per angle motion (CRSPAM) was defined as change in total CSS score divided by change in Cobb angle. The correlation of CRSPAM with severity of stenosis, represented by total CSS score in neutral position, was evaluated using Pearson correlation analysis.
Results
The total CSS score was significantly higher in extension (6.04±2.68) than in neutral position (5.25±2.47) (p<0.001), and significantly higher in neutral than in flexion position (4.40±2.45) (p<0.001). The CRSPAM was significantly and positively correlated with total CSS score in neutral position in the flexion-extension range (r=0.22, p=0.04) and flexion-neutral range (r=0.27, p=0.01).
Conclusion
In symptomatic CSS patients, the radiological severity of stenosis increases with extension and decreases with flexion. In patients with CSS, the rate of variation in spinal stenosis increases with increased severity.
INTRODUCTION
Cervical spondylotic myelopathy (CSM) is attributed to compressive forces acting on the spine and spinal cord [1]. Cervical spinal stenosis (CSS) and dynamic changes in the spinal canal space in cervical motion are significant factors contributing to the development of CSM [1-3]. Studies using cervical spine dynamic magnetic resonance imaging (MRI) revealed increased stenosis in extension and flexion, supporting the role of dynamic factors in the development of CSM [4-6].
However, previous studies have been inconsistent on whether increased CSS is observed in both flexion and extension. While multiple studies reported increased CSS in extension [4-7], a recent study reported anterior migration of the nucleus pulposus with cervical extension [8], suggesting that cervical extension may play a role in the reversal of disc prolapse, an important factor in CSS. Several studies have shown increased spinal stenosis in flexion [4-6]; however, the detection rate has been consistently lower than in extension, and one study showed a tendency for decompression of the cervical spine in flexion [9].
Therefore, due to conflicting results, the primary aim of this study was to determine whether CSS increased and/or decreased in flexion and/or extension. The secondary aim of this study was to investigate whether changes per angle motion in CSS differed according to the severity of stenosis.
MATERIALS AND METHODS
The medical records and imaging studies of 176 consecutive symptomatic patients who underwent cervical spine dynamic MRI from May 2012 to April 2014 were reviewed retrospectively. Patients underwent cervical spine dynamic MRI when cervical radiculopathy or myelopathy was clinically suspected but the correlation with neutral position cervical spine MRI findings was not entirely clear, or when patient’s history and X-ray findings suggested cervical spine instability.
Patients aged >30 years with symptoms of cervical radiculopathy or CSM were included. The exclusion criteria were: (1) no evidence of CSS on MRI, (2) presence of any comorbidity significantly affecting general function, and (3) non-spondylotic myelopathy (i.e., traumatic or metastatic).
This study was approved by the Institutional Review Board of Seoul National University Hospital (IRB No. 1611-040-805).
Participants
A total of 92 patients with a mean age of 57.80±10.41 years, were included in the study (Table 1). Most patients (84.78%) manifested mild symptoms of Nurick grade 0 to 1. Upper extremity sensory symptoms (77.17%) were the most frequent source of complaint, with median symptom duration of 4 months.
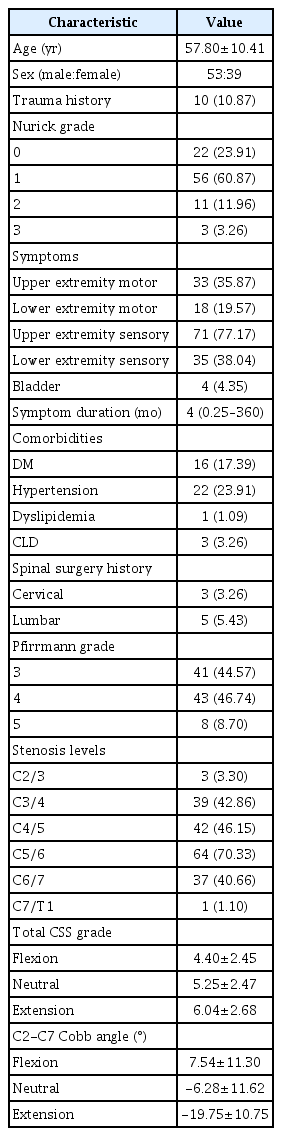
Patients’ demographics
Intervertebral disc degeneration was assessed [10], and the highest Pfirrmann grade between C2/3 and C7/T1 segments was recorded. Cervical intervertebral disc levels with the most severe CSS were defined as stenosis levels and recorded. Multiple levels were recorded if cervical canal stenosis of the same severity was found at multiple levels. The most severe level of stenosis was found at the C5/6 vertebral segment (70.33%), followed by C4/5 (46.15%).
Patient positioning for MRI
All patients were examined with cervical dynamic MRI (1.5 T or 3.0 T) in the supine position. Dynamic MRI was performed by positioning cushions under the posterior neck for extension and posterior head for flexion, as tolerated. T1- and T2-weighted sagittal images and T2-weighted axial images were acquired in the neutral position, and sagittal T2-weighted images were acquired in flexion and extension positions.
An illustrative case of cervical dynamic MRI is presented in Fig. 1.
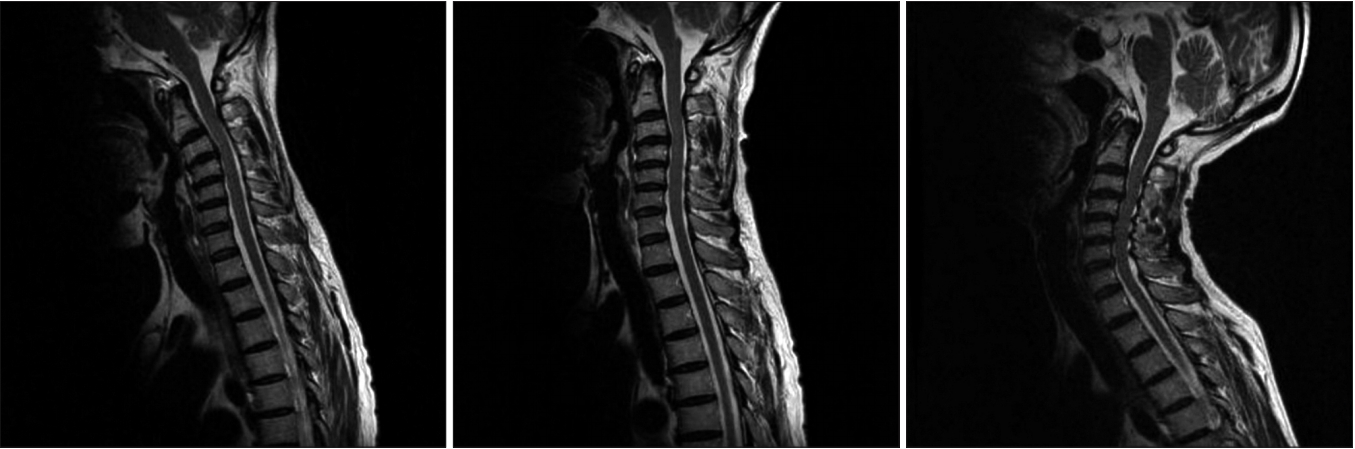
Illustrative case of cervical dynamic magnetic resonance imaging in left-to-right flexion, neutral, and extension positions.
Parameters
The total CSS score was defined as the sum of CSS grades [11] from the vertebral segments C2/3 to C7/T1. The CSS grade was categorized as follows: grade 0, no spinal stenosis; grade 1, more than 50% of subarachnoid space obliterated without signs of spinal cord deformity; grade 2, cord deformity without signal change on the spinal cord; and grade 3, increased signal intensity on the spinal cord in T2-weighted image. Total CSS score was determined in flexion, neutral, and extension positions by a single observer, and was used as a measure of spinal stenosis.
Cervical spine Cobb angle (C2–C7) [12] was measured in flexion, neutral, and extension positions.
The change rate in stenosis per angle motion (CRSPAM) was defined as change in total CSS score divided by change in Cobb angle. The CRSPAM varied with the severity of spinal stenosis, and was determined for flexionextension, flexion-neutral, and neutral-extension ranges.
Statistics
Statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). To compare the degree of CSS in flexion, neutral, and extension positions between individual patients, the total CSS score in each position was compared using one-way repeated measures analysis of variance.
To examine the rates of CSS variation in relation to the severity of stenosis, the CRSPAM was determined in the flexion-extension, flexion-neutral, and neutral-extension ranges, and its relationship to total CSS score in neutral position was evaluated using Pearson correlation analysis.
RESULTS
Total CSS scores in flexion, neutral, and extension positions were 4.40±2.45, 5.25±2.47, and 6.04±2.68, respectively. Total CSS score was significantly higher in extension than in neutral (p<0.001) and significantly higher in neutral than in flexion positions (p<0.001) (Fig. 2).
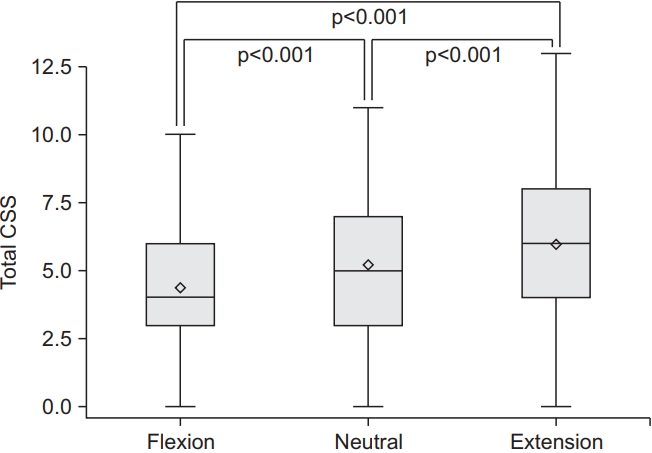
Total cervical spinal stenosis (CSS) score in flexion, neutral, and extension positions.
CRSPAM showed a weak positive correlation (r=0.22) with total CSS score in neutral position in the flexion and extension range (p=0.04) (Fig. 3A). CRSPAM also showed a weak positive correlation (r=0.27) with total CSS score in neutral position in the flexion and neutral range (p=0.01) (Fig. 3B). However, such correlation was not detected in the neutral and extension ranges (Fig. 3C).
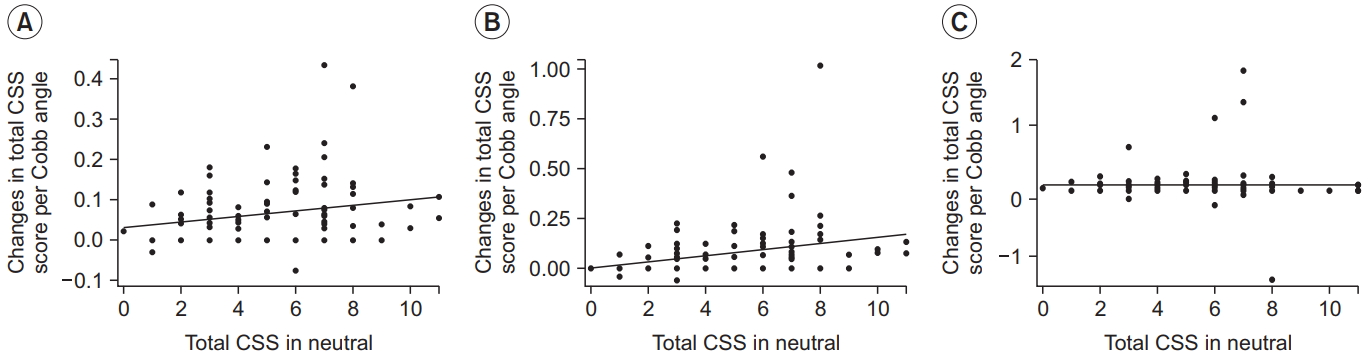
Change rate in stenosis per angle motion in flexion and extension (A), flexion and neutral (B), and neutral and extension (C) ranges in relation to total cervical spinal stenosis (CSS) score in neutral position.
DISCUSSION
This study demonstrated that in symptomatic patients with CSS, extension was associated with narrowing of the cervical spinal canal and flexion, with decreased stenosis. The severity of CSS increased with progression from flexion to neutral and extension positions. With extension, the rate of variation in stenosis increased with increased CSS severity (Fig. 3A).
This study reinforced the results of a previous report of increased CSS in extension and a relative decrease in stenosis in flexion [9]. However, the results of previous studies varied, with a few reporting increased stenosis in both flexion and extension [4-7], while others suggested decreased disc prolapse in extension [8,13]. The inconsistent results may be attributed to differences in participant characteristics. The study reporting anterior migration of the nucleus pulposus in extension was conducted on healthy volunteers [8]. With disc degeneration, the nucleus pulposus condenses and the annulus is weakened and stiffened [14], leading to difficulties in anterior migration of disc material. Furthermore, neck extension may lead to posterior spinal cord compression due to ligamentum flavum hypertrophy [15], which is not common in healthy volunteers with minimal cervical spondylosis.
In contrast to previous studies reporting the association of flexion with increased spinal stenosis, our results showed that spinal stenosis was decreased in flexion. This discrepancy may have been due to differences in the method of spinal stenosis evaluation. This study used total CSS score to measure spinal stenosis. Since CSS grading at each vertebral segment was totaled, small changes may have been accentuated or significant changes at a single level may have been diluted. In most cases, a tendency for decreased spinal stenosis in flexion was seen in all vertebral segments (illustrative case, Fig. 1). However, cases of instability evident at a single level and aggravated spinal stenosis in flexion were not adequately appreciated in our study. With cervical flexion, the ligamentum flavum becomes relatively thinner than in extension [16], leading to posterior decompression. However, the spinal cord is also stretched and compressed against the posterior longitudinal ligament and vertebral body [17]. Therefore, despite the decrease in total CSS score in flexion, the spinal cord may be injured during motion, warranting caution in translating results into clinical practice. Furthermore, increased stenosis at the most stenotic level is clinically more important than the total CSS score.
Interestingly, our study results showed that increased severity of spinal stenosis markedly elevated the rate of change in spinal stenosis in the flexion-neutral range (Fig. 3B), but not in the neutral-extension range (Fig. 3C). A possible explanation is the ‘ceiling effect’ of CSS grading. Patients with more severe stenosis may have higher changes in the flexion-neutral range because of lack of free space, without significant changes in the neutralextension range because of the ceiling effect. However, in such a case, patients with mild stenosis show significant changes in the neutral-extension range, which was not observed in our study. Studies have reported differences in spinal kinematics according to sagittal alignment and disc degeneration [18,19]. Our study findings may have been affected by differences in kinematics. Further studies using quantitative kinematic analysis are needed for verification.
Our study has clinical implications. A cervical extension maneuver is still widely used to treat cervical spinal pain [20]. Our findings indicate that caution is needed in extension, especially in patients with severe CSS. Clinically, it is still uncertain whether extension should be limited, because it is established that disc degeneration and ensuing kyphotic posture are delayed with extension exercises [21,22]. Since the rate of increase in CSS was greater in patients with a higher severity of stenosis, patients with severe stenosis may need to restrict cervical motion. Our findings of increased stenosis in extension and a relative decrease in flexion may explain the kyphotic posture in CSM patients [23], a compensatory action to degenerative changes, although the association was not investigated.
This study has several limitations. First, it was a retrospectively study. Second, MRI was performed with patients in the supine position. Results may differ in the upright position. Third, semi-quantitative evaluation was conducted using a CSS score. Semi-quantitative analyses are less reliable than quantitative analysis. In the presence of cord signal changes, CSS was graded as 3 in all three positions regardless of change in canal space. Therefore, in the presence of cord signal changes, narrowing of the spinal canal was not reflected in the CSS score. Total CSS score was used in our study to represent the total stenosis severity score. The contribution of spine motion to canal stenosis according to the spine level was not evaluated due to inherent limits of the CSS grading, which was not sensitive enough to capture delicate changes in canal stenosis. Due to limitations associated with time and cost, the dynamic cervical spine MRI protocol at our hospital does not include axial images in all the three positions and stenosis was only evaluated in the sagittal plane, and not in the axial plane. Finally, whether anterior or posterior compression contributed to spinal stenosis was not evaluated.
In conclusion, cervical extension is associated with increased radiological spinal stenosis and flexion with decreased stenosis in symptomatic patients with CSS. The rate of increase in spinal stenosis under extension is associated with the severity of spinal stenosis. Therefore, caution is needed in performing cervical extension exercises in CSS patients. Further studies using quantitative kinematics with MRI in the upright position are needed to better elucidate mechanisms and factors underlying the dynamic changes in spinal stenosis.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MEST) (No. NRF-2016M3A9F1941984).