Functional Electrical Stimulation to Ankle Dorsiflexor and Plantarflexor Using Single Foot Switch in Patients With Hemiplegia From Hemorrhagic Stroke
Article information
Abstract
Objective
To evaluate the effects of functional electrical stimulation (FES) to ankle dorsiflexor (DF) and ankle plantarflexor (PF) on kinematic and kinetic parameters of hemiplegic gait.
Methods
Fourteen post-stroke hemiplegic patients were considered in this study. Electrical stimulation was delivered to ankle DF during the swing phase and ankle PF during the stance phase via single foot switch. Kinematic and kinetic data were collected using a computerized motion analysis system with force plate. Data of no stimulation (NS), DF stimulation only (DS), DF and PF stimulation (DPS) group were compared among each other.
Results
Peak ankle dorsiflexion angle during swing phase is significantly greater in DS group (-1.55°±9.10°) and DPS group (-2.23°±9.64°), compared with NS group (-6.71°±11.73°) (p<0.05), although there was no statistically significant difference between DS and DPS groups. Ankle plantarflexion angle at toe-off did not show significant differences among NS, DS, and DPS groups. Peak knee flexion in DPS group (34.12°±13.77°) during swing phase was significantly greater than that of NS group (30.78°±13.64°), or DS group (32.83°±13.07°) (p<0.05).
Conclusion
In addition to the usual FES application stimulating ankle DF during the swing phase, stimulation of ankle PF during stance phase can help to increase peak knee flexion during the swing phase. This study shows the advantages of stimulating the ankle DF and PF using single foot switch for post-stroke gait.
INTRODUCTION
Adults with hemiplegia often demonstrate gait impairments, such as foot drop due to inadequate dorsiflexion and decreased push off due to plantarflexor weakness or spasticity. Foot drop is a common impairment in gait of hemiplegics, contributing to an asymmetric gait pattern, and has been shown to be correlated with delayed recovery of functional ambulation in individuals after stroke. Foot drop is also a cause of falling down and related secondary injury to trauma. Multidisciplinary approach to correct foot drop made it possible to use effective methods, such as ankle-foot orthoses, antispastic drug, chemical and or surgical neurolysis. Functional electrical stimulation (FES) is another intervention that is used to stimulate the ankle dorsiflexor (DF) muscles during the swing phase to correct foot drop [1]. FES to ankle DF during the swing phase can help with correcting foot drop and improve walking [2,3,4]. During the gait, ankle plantarflexor (PF) muscles also play an important role in generating propulsive force at the transition from stance to swing, which is essential for walking speed. Decreased force generation by the ankle PF of hemiparetic side resulted in decreased swing phase knee flexion [5,6].
Recently, there have been a few research studies that demonstrated improved walking with additive PF stimulation to the traditional DF stimulation [7,8]. One of these reports showed increase in peak knee flexion angle when FES is applied [8]. These endeavors have produced results that may aid in improving hemiplegic gait; the studies also had limitations on practical application. One such study used two foot switches, which might limit practical use [7]. Another report contained data regarding walking on treadmills only, and did not include data on walking on grounds [8].
Thus, we proposed FES with a single switch which controls stimulation of ankle DF and PF alternately on the ground. The aim of this study was to evaluate the effects of delivering FES using a single switch to the ankle DF during the swing phase and ankle PF during the stance phase on kinematic and kinetic data of hemiplegic gait.
MATERIALS AND METHODS
Subjects
Fourteen patients (8 males, 6 females) with post-stroke hemiparesis participated in this study. Inclusion criteria were as follows: independent walking more than 5 minutes without gait device, sufficient passive range of motion to neutral position (0°) or a plantarflexion with the knee flexed more than 5°, 3 months after an instance of stroke. Exclusion criteria were as follows: inability to communicate with investigators, skin lesions on electrical stimulation sites, pacemaker insertion status, pregnancy [7,8]. All of the 14 subjects had a hemorrhagic stroke. Of the subjects, one female subject's data were excluded from the analysis due to equipment error during data collection (subject no. 13). Another female subject did not finish the entire course of evaluation (subject no. 14) (Table 1). Data of the remaining 12 subjects were analyzed. The mean age of the subjects was 40.4±11.6 years, (8 males, 6 females). The mean post-hemiplegic incident was 2±2.8 years and at least 4 months after incident.
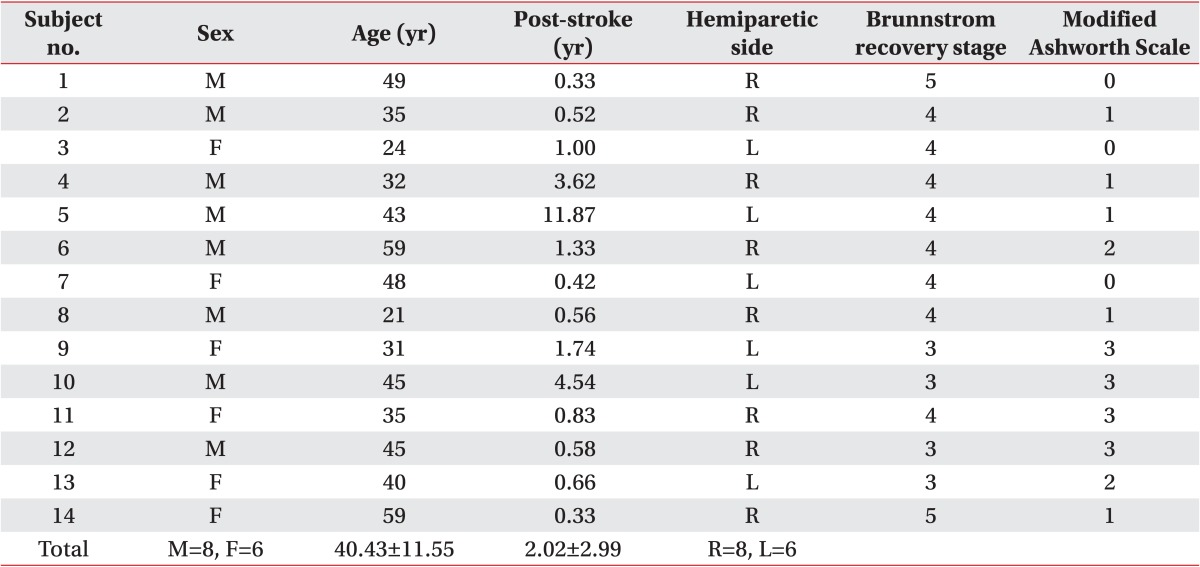
Demographic and general characteristics for the 14 subjects
Functional electrical stimulation
Adhesive surface electrodes were located at the site which showed maximal contraction on the ankle DF and PF. Novastim CU-FS1, functional electrical stimulator (CU Medical Systems Inc., Wonju, Korea), was used to deliver electrical stimulation. This equipment used a single compressive foot switch, and was programmed to deliver electrical stimulation to one channel while the foot switch was opened and to the other channel while foot switch was closed. One compressive switch was attached to the hemiparetic heel pad. At the time of heel contact, electrical stimulation was delivered to stimulate ankle PF. At the time of heel off, electrical stimulation was delivered to ankle DF [5]. Symmetric biphasic wave was set at 35 Hz and 300 µs pulse width. Stimulation amplitude was set until the subject's maximal tolerance was reached [7,8].
Gait analysis
Data were collected by computerized motion analysis system with 6 cameras (Vicon; Oxford Metric Ltd., Oxford, England) that collected data from attached reflective markers at 100 Hz. Ground reaction forces (GRFs) from hemiparetic leg was measured by force platforms (ATMI, Suwon, Korea) which was synchronized with the motion analysis system at 1,000 Hz.
Axial GRF and electrical current from the functional electrical stimulator were used to determine gait events and timing of FES. Patients were asked to ambulate 6 m on an even surface without walking device.
Total of three test sessions were performed at the subject's self-selected walking speeds. At the first session, patient was asked to ambulate on the test way without any stimulation (NS). At the second session, the patient ambulated with ankle DF stimulation during the swing phase (DS). At the third session, the patient ambulated with additive ankle PF stimulation during the stance phase (DPS). Each session was composed of 5 trials. To avoid fatigue, a 10-minute intersession break and a 3-minute inter-trial break were given to the patient (Fig. 1).

Performed total of three test sessions: 1) patient was asked to ambulate on test way without any stimulation (NS); 2) patient ambulated with ankle DF stimulation during the swing phase (DS), 3) patient ambulated with additive ankle PF stimulation during the stance phase (DPS), which is composed of 5 trials each, these were performed with 10-minute intersession break and a 3-minute inter-trial break to avoid fatigue. DF, dorsiflexor; PF, plantarflexor; NS, no stimulation; DS, DF stimulation only; DPS, DF and PF stimulation.
Outcome variables and data analysis
One of outcome measures for the effectiveness of FES during gait were knee flexion angle, ankle DF angle and PF angle in the sagittal plane, during the gait cycle for the paretic leg. The other outcome measures were peak GRF in anterior to posterior (AP) and axial axis. Peak GRF was defined as ratio of the anteriorly or upwardly directed maximum GRF to the weight of the participant. Repeated-measures one-way ANOVA were performed to detect differences among NS, DS, and DPS groups. Sphericity was violated because Mauchly test was significant (p=0.37). Greenhouse-Geisser correction was used as epsilon was smaller than 0.75 (ε=0.673). Tukey honest significant difference was used as a post-hoc analysis. All statistical analyses were performed using the IBM SPSS Statistics ver. 20 (IBM Korea Inc., Seoul, Korea).
RESULTS
Peak ankle DF angle during swing phase was significantly greater in the DS (-1.55°±4.55°) and the DPS group (-2.23°±4.82°), compared with the NS group (-6.71°±5.86°) (p<0.05), although there was no statistically significant difference between the DS and DPS groups (Fig. 2). Initial contact ankle DF angle was also significantly greater in the DS (-4.53°±2.73°) and DPS groups (-5.20°±3.01°), compared with the NS group (-8.55°±3.93°) (p<0.05) (Fig. 3). And there was no statistically significant difference between the DS and DPS groups like the preceding results (Fig. 3). Ankle plantarflexion angle at toe-off did not show significant differences among the NS (0.00°±7.73°), DS (0.73°±7.44°), and DPS groups (0.16°±7.54°).
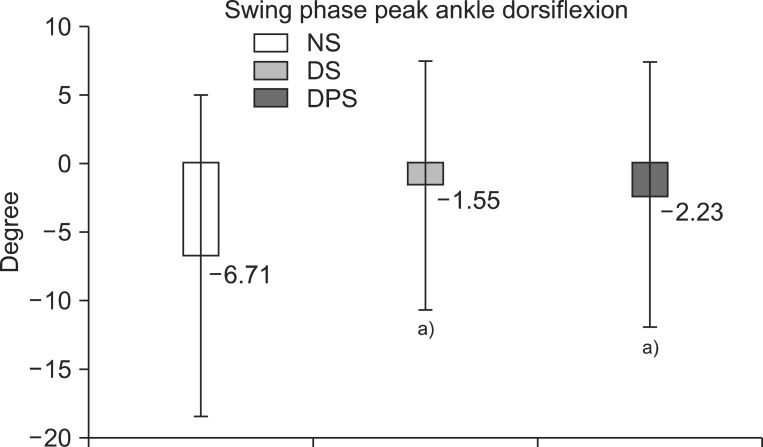
Swing phase peak ankle dorsiflexion angle was significantly greater in dorsiflexor stimulation only group (DS, -1.55°±9.10°) and dorsiflexor and plantarflexor stimulation group (DPS, -2.23°±9.64°), compared with no stimulation group (NS, -6.71°±11.73°) (p<0.05), although there was no statistically significant difference between DS and DPS groups. a)p<0.05, significant difference from no stimulation.

Initial contact ankle dorsiflexion angle was still significantly greater continuing to swing phase (Fig. 2) in dorsiflexor stimulation only group (DS, -4.53°±2.73°) and dorsiflexor and plantarflexor stimulation group (DPS, -5.20°±3.01°), compared with no stimulation group (NS, -8.55°±3.93°). a)p<0.05, significant difference from no stimulation.
Peak knee flexion angle during swing phase of the DPS group (34.12°±4.77°) was significantly greater than that of the NS group (30.78°±4.64°) or the DS group (32.83°±4.07°) (p<0.05) (Fig. 4).
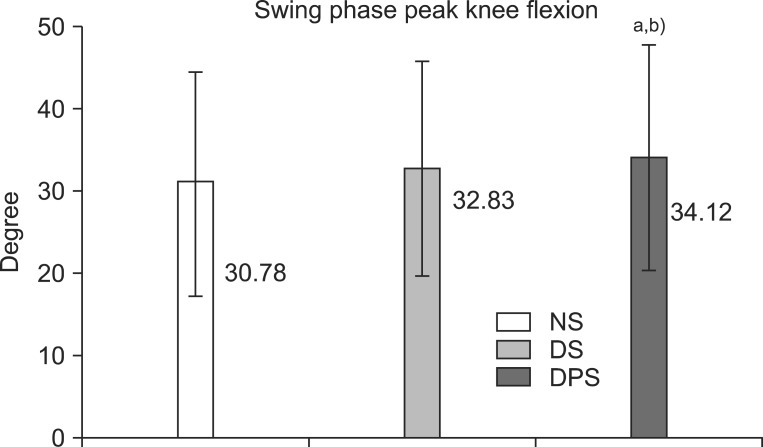
Swing phase peak knee flexion was significantly greater in order of dorsiflexor and plantarflexor stimulation group (DPS, 34.12°±13.77°), dorsiflexor stimulation only group (DS, 32.83°±13.07°), and no stimulation group (NS, 30.78°±13.64°). a)p<0.05, significant difference from no stimulation. b)p<0.05, significant difference from dorsiflexor stimulation only.
Peak knee flexion angle did not show a significant difference between the NS (30.78°±4.64°) and the DS group (32.83°±4.07°) (Fig. 4). Mid-stance knee extension angle did not show a significant difference among the NS (-5.27°±4.44°), DS (-5.24°±4.64°) and DPS groups (-5.49°±4.67°). Knee flexion angle at toe-off also showed no significant difference among the NS (-8.55°±7.87°), DS (-4.53°±5.46°), and DPS groups (-5.20°±6.01°) (Table 2). Parameters of kinematics and kinetics, such as gait speed (0.49±0.26, 0.48±0.24, 0.49±0.26 m/s), step length (0.40±0.12, 0.40±0.10, 0.40±0.12 m), stride length (0.72±0.23, 0.71±0.21, 0.72±0.23 m) (Table 3), toe-off timing during gait cycle, AP GRF (9.61±0.55%, 9.82±0.86%, 9.77±0.64% of body weight), and axial GRF (43.7±38.6%, 47.8±44.7%, 48.6±42.1% of body weight) (Table 4), did not show significant differences among the NS, DS, and DPS groups.

Comparison of group-pairs of knee angle during gait

Temporal data during gait cycle depend on electrical stimulation
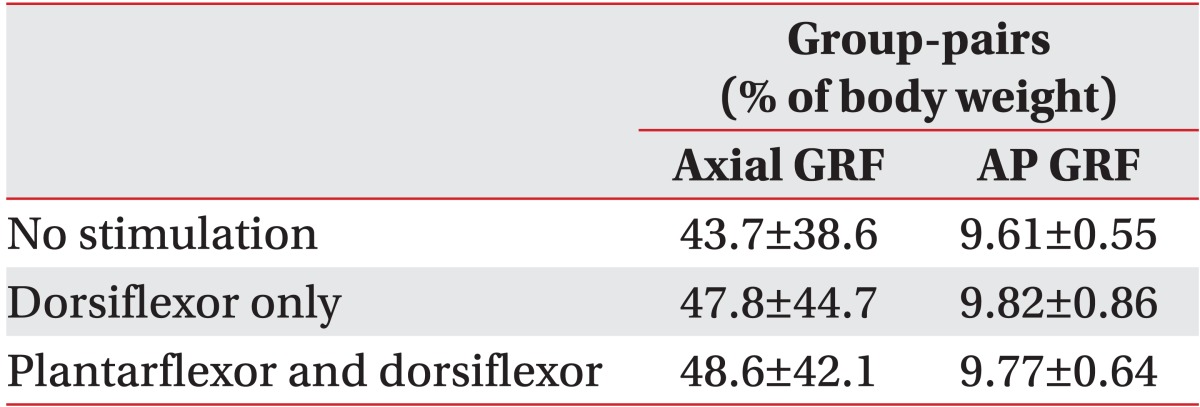
GRF at stance phase of hemiparetic side
DISCUSSION
The post-stroke hemiplegic patient suffers not only from ankle DF weakness but also PF weakness. Studies have shown that adults with stroke do not push effectively with their PF during gait [9,10,11]. FES for hemiplegic gait is typically delivered only to the ankle DF to correct 'foot drop' during the swing phase, thereby failing to address other important stance and swing phase post-stroke gait deficits at the hip and knee [8,12].
Thus, we hypothesized that delivery of FES to the ankle PF of hemiparetic leg during stance phase combined with traditional FES to the ankle DF would increase propulsive force generation required to push off and this increased push off would change knee and ankle angles during gait, compared to the traditional FES delivery to ankle DF.
A few recent research studies demonstrates some advantages of delivering electrical stimulation to ankle PF during the stance phase and to stimulation of ankle DF during the swing phase. The advantages are the increase of peak knee flexion angle during the swing phase and AP GRF. But, these results were deduced from gait on the treadmill, which is different from ground walking [7]. Another advantage of DF and PF stimulation is improved performance of hemiplegic gait. Subjects who received ankle DF and PF stimulation that is delivered from a wearable FES system during walking, showed improvement in the 6-minute walk test, Emory Functional Ambulation Profile, and Stroke Impact Scale compared with subjects who conducted walking exercise without the FES system. But, this study did not measure knee and ankle angle change during the gait cycle [8]. While, it might be beneficial to correct foot drop of post-stroke patients, clinical use also has limitations due to the complicated dual switch system that requires sensors at the hemiparetic side heel and head of first metatarsal, or forefoot and hindfoot [7,8]. It requires larger equipment and more time to apply. It is possible to address these problems with wireless equipment or light weight equipment. Another way to improve efficiency of the method is by simplification of the switch system. We tried the single switch system that performs alternate functions to the dual switch system. In order to confirm the practicability of the dual switch system as previously reported [7,8], we studied ground walking instead of treadmill walking, while also testing the simplified single switch system rather than the dual switch system.
The increase of peak knee flexion angle during the swing phase at stimulation on DF and PF has appeared in line with previous published test results; however, we identified some differences as described below.
While the peak knee flexion angle during the swing phase increased in our research, it had decreased in the prior study, when only DF was stimulated. Also, the value further increased when both DF and PF were stimulated. Furthermore, while the AP GRF value in previous studies had shown significant increases when both DF and PF were stimulated, our studies showed an increasing trend that was not statistically significant. These differences arose due to 1) peak knee flexion angle during the swing phase, 2) AP GRF. First likely cause is the site of the experiment; while the treadmill was used in the previous study, the ground was used in our study [7,13]. The second cause is a different switch system. Dual switch system was used in previous studies, while we used the simplified single switch system in our study [7,8,13]. Negative effect on AP GRF in our study may limit the practical applicability of the single switch system. Further investigation is clearly needed.
Hemiplegic gait is affected by additive ankle PF stimulation which increased swing phase knee flexion angle in the previously mentioned study, as well as in our current research. Stroke patients with different levels of motor recovery show compensatory adaptation to control the proximal lower limb and improve walking velocity [14]. Chronic stroke survivors generally show decreased knee flexion in the paretic leg during swing phase compared with the non-paretic leg, or compared with neurologically unimpaired control subjects walking at matched speeds [15,16].
We observed some interesting results. First, peak swing phase ankle DF angle showed no statistical significance between the DS (-1.55°±9.10°) and DPS groups (-2.23°±9.64°) (Fig. 2). Swing phase ankle DF might have experienced interference with delayed effect of electrical stimulation triggering muscle contraction during the stance phase. The result of our study implies no negative effect of stance phase ankle PF stimulation on swing phase ankle DF. Second, ankle DF angle that increased during the swing phase is maintained until the initial contact of gait cycle (Fig. 3).
A notable limitation of this study was fatigue resulting from the long experimental time. It took about 2 hours from subject preparation and for equipment mounting to the end of the test. Additionally, the subject was informed on their own gait pattern, allowing them to know the location of the force plate. Consequently because of inappropriate stepping on force plate measuring GRF, more trial repetitions than necessary were conducted in order to obtain the values for 5 trials per session. Thus, fatigue that could influence gait performance occurred despite of the inter-trial and intersession resting. Another limitation was the non-randomized order of the test session.
In this study, we delivered electrical stimulation to two separate channels, one for ankle DF during the swing phase and the other for ankle PF during the stance phase via single switch system for hemiplegic foot drop. Our study showed that knee flexion angle during the swing phase increased when electric stimulation was applied only to DF during the swing phase, while knee flexion angle during the swing phase further increased with ankle DF stimulation during the swing phase together with PF stimulation during the stance phase.
Notes
No potential conflict of interest relevant to this article was reported.