INTRODUCTION
Rheumatoid arthritis (RA) is a systemic inflammatory disease that mainly affects the joints [1]. Although the main manifestations involve the joints, previous studies have reported that extra-articular manifestations occur in 10%-20% of RA patients and that these symptoms correlate with increased mortality [2]. Clinical neuropathy occurs in 0.5% to 85% of RA patients [3,4,5,6], and presents in the form of mononeuritis multiplex, sensorimotor neuropathy, and entrapment neuropathy [5]. Clinical neuropathy may present with a wide variety of symptoms, such as pain, paresthesias, and muscle weakness. These symptoms may mimic and overlap those of arthritis, and it is difficult to distinguish peripheral neuropathy symptoms from arthritis symptoms.
The various causes of peripheral neuropathy in RA include nerve entrapment, drug toxicity, vasculitis, and rarely amyloidosis [7,8]. A few studies also suggest that the development of RA can be attributed to an autoimmune phenomenon [9,10]. However, few reports have explored the relationship between peripheral neuropathy and clinical findings in RA patients. The aim of this study was to electrophysiologically evaluate peripheral neuropathy in RA patients with neurologic symptoms, and to demonstrate the relationships between peripheral neuropathy and demographic, clinical, and laboratory findings.
MATERIALS AND METHODS
Patients
Patients with a clinical diagnosis of RA who had tingling or burning sensation in any extremity were enrolled in this study. All of the patients met the American College of Rheumatology criteria for RA [11]. Exclusion criteria were 1) patients with systemic diseases or conditions that are associated with neuropathy (i.e., diabetes mellitus, hypothyroidism, amyloidosis, alcohol intake, liver failure, chronic renal failure treated by hemodialysis, or pregnancy), 2) patients who underwent orthopedic surgery, and 3) patients with neurologic disorders. The recorded parameters included age, gender, duration of RA, laboratory test results, medications, neuropathic symptoms, and functional status. Laboratory tests included erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), and anti-cyclic citrullinated peptide (anti-CCP) antibody.
Methods
Neuropathic symptom measurement
Neuropathic symptoms and signs were quantified with the neuropathy symptom scale (NSS). The NSS is a five-question multiple-choice self-report inventory that is used for measuring the severity of neuropathic symptoms and signs. The NSS has a maximum score of 9, with a higher score indicating more severe neuropathic symptoms [12]. The functional status of patients with RA was classified as class I-IV according to the revised criteria for the classification of the functional status in RA. A higher class reflects a poorer functional status [13].
Electrophysiological study
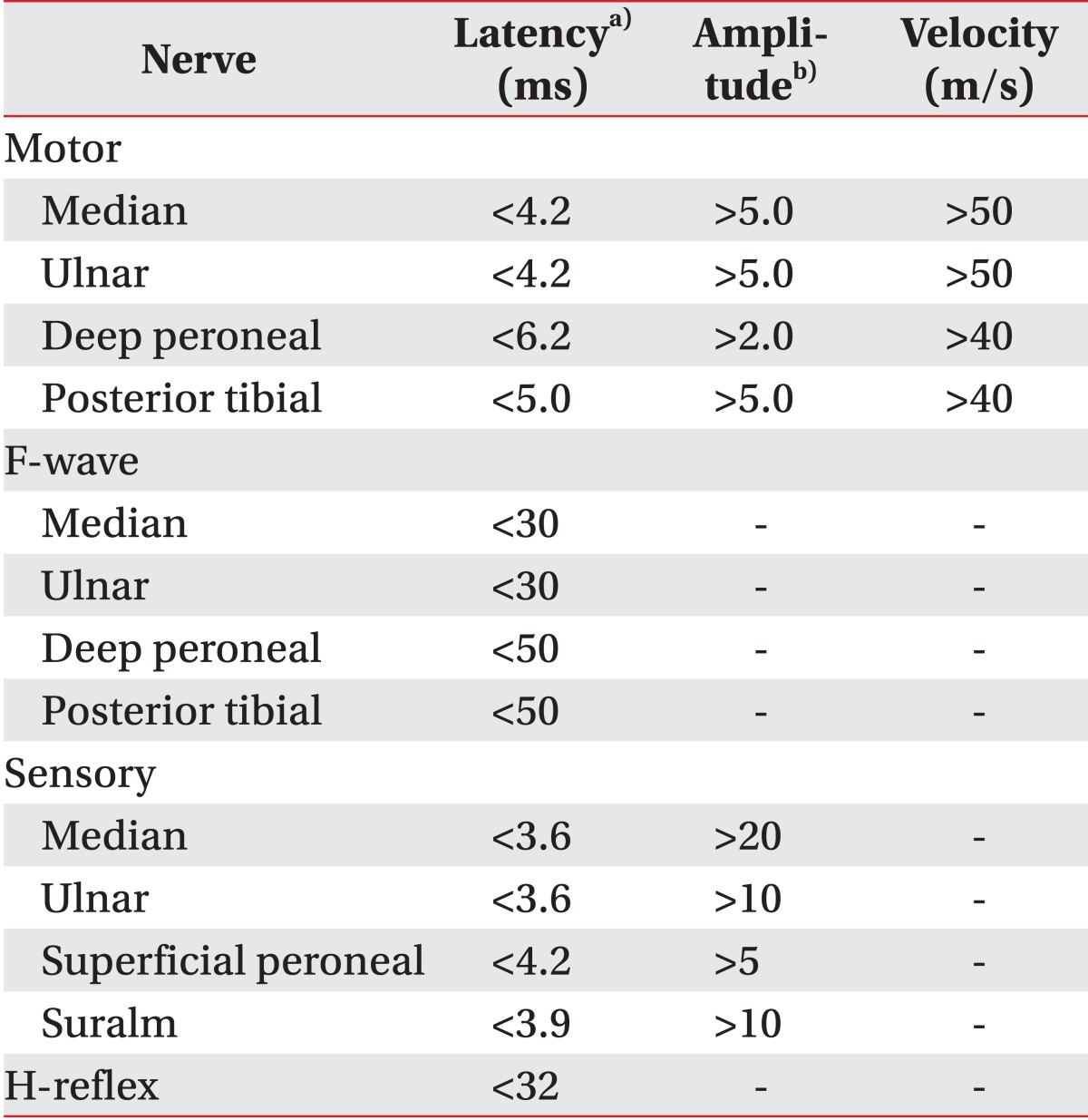
Electrophysiological studies were performed using the Medelec-Synergy EMG instrument (Oxford Instrument Co., Surrey, UK). The skin temperature was kept between 31℃ and 32℃. Median, ulnar, peroneal, and posterior tibial motor nerve conduction studies (NCSs), including F-waves, were performed unilaterally on the symptomatic side. Median, ulnar, superficial peroneal, and sural sensory NCSs were performed unilaterally on the symptomatic side. The latency of the H-wave was measured bilaterally. Motor NCSs were performed using the belly-tendon method. Sensory nerve conduction was studied antidromically. All amplitudes were determined based on the base-to-peak value; the peak latency and onset latency were measured for sensory nerve action potential (SNAP) and compound motor action potential (CMAP), respectively. The conduction velocity of each nerve was measured. Findings were compared with the reference values that are used in our center as described in Table 1.
A bilateral study of three extremities was conducted if the NCS showed abnormal findings. Polyneuropathy was diagnosed when at least three abnormal parameters were present. If the median CMAP latency was greater than 4.2 ms or the median SNAP was greater than 3.6 ms, we used the 'mid-palm' technique to diagnose carpal tunnel syndrome (CTS). In this technique, the median nerve was stimulated at the wrist and the median SNAP was recorded in digit 3 at a 7-cm distance (palm). The median nerve was then stimulated at the palm at a 14-cm distance (wrist). Presence of CTS was considered when the ratio of palm to wrist latency was lower than 50%. All of the patients gave informed consent, and the study was approved by the ethics committee of our university. Patients were then divided into two groups according to the presence or absence of peripheral neuropathy. The clinical and laboratory findings were compared between the two groups.
Statistical analysis
Statistical analyses were performed with SPSS 13.0 for Windows (SPSS Inc., Chicago, IL, USA). For comparison between the two groups, a Mann-Whitney U test or t-test was used for continuous variables and a Fisher exact test was used for categorical variables. The variables were analyzed with univariate logistic regression analysis to determine their effects on polyneuropathic involvement. Odds ratios and 95% confidence intervals (CIs) were calculated for each factor. In addition, multivariable regression analyses were performed to assess the independent association between peripheral neuropathy and each factor. All of the variables with p-value <0.2 by univariate analysis were selected for the multivariable logistic regression analysis. A p-value of <0.05 was considered statistically significant.
RESULTS
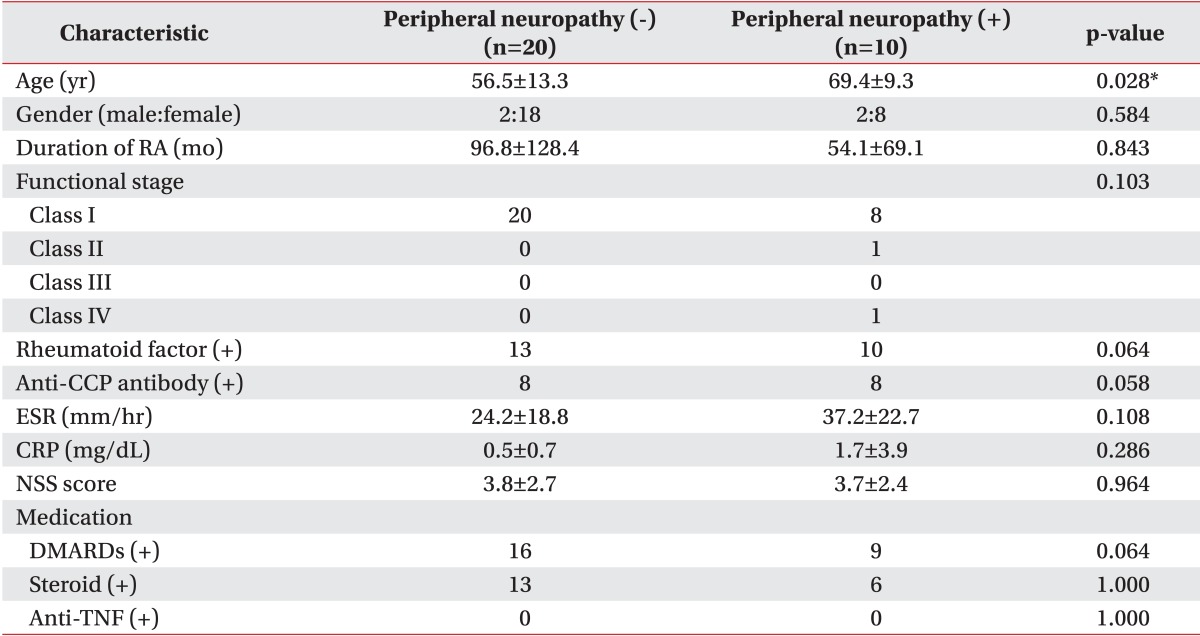
A total of 30 RA patients (26 women and 4 men) were enrolled in this study. Of these, 10 patients showed peripheral neuropathy in the electrophysiological study: 2 had bilateral CTS, 5 had unilateral CTS, 1 had sensory polyneuropathy, and 2 had sensorimotor polyneuropathy. Two patients had peripheral neuropathy of the lower limbs, 1 patient had neuropathy of both upper and lower limbs, and 7 patients had isolated upper limb involvement. The mean ages of the patients with and without peripheral neuropathy were 69.4 and 56.5 years, respectively (p<0.05). The duration of the disease was 96.8 months in patients without peripheral neuropathy and 54.1 months in patients with peripheral neuropathy, respectively. All of the patients without peripheral neuropathy were in functional stage class I, whereas some of the patients with peripheral neuropathy were in class II and class IV. However, there was no statistically significant difference in the RA duration and functional stage between the two groups. Among the 20 patients without peripheral neuropathy, 13 patients (65.0%) showed a positive RF and 8 patients (40.0%) showed a positive anti-CCP antibody. In contrast, among the 10 patients with peripheral neuropathy, all of the patients were positive for RF, and 8 patients (80.0%) were positive for anti-CCP antibody. Patients with peripheral neuropathy were thus more likely to have a positive serological marker for RA than those without peripheral neuropathy; however, this difference was not statistically significant using the Fisher exact test (Table 2).
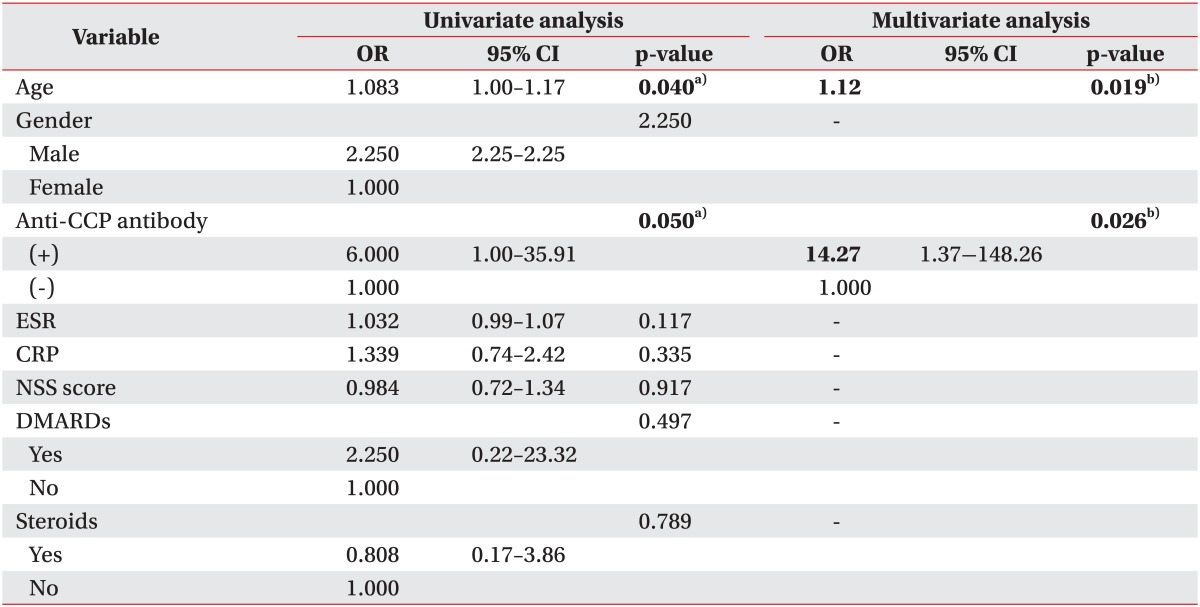
We found that anti-CCP antibody was significantly associated with an increased risk of polyneuropathy using a univariate logistic regression model (relative risk [RR], 6.00; 95% CI, 1.00-35.91). Age was also significantly associated with presence of peripheral neuropathy in univariate logistic regression analysis (RR, 1.083; 95% CI, 1.00-1.17). Multiple regression analysis demonstrated that peripheral neuropathy in RA patients was independently increased by age (RR, 1.12; 95% CI, 1.02-1.13) and anti-CCP antibody (RR, 14.27; 95% CI, 1.37-148.26) (Table 3). Age of patients did not show a difference according to the presence or absence of anti-CCP antibody. Age of patients who were positive for anti-CCP antibody and negative for anti-CCP antibody was 59.2±12.4 and 61.1±14.1 years, respectively. When we compared the odds ratio of anti-CCP antibody for peripheral neuropathy according to age, odds ratio of anti-CCP antibody was higher in the old age group (Table 4). No significant association was found between peripheral neuropathy and gender, NSS, functional stage, ESR, CRP, type of medication, and RF.
DISCUSSION
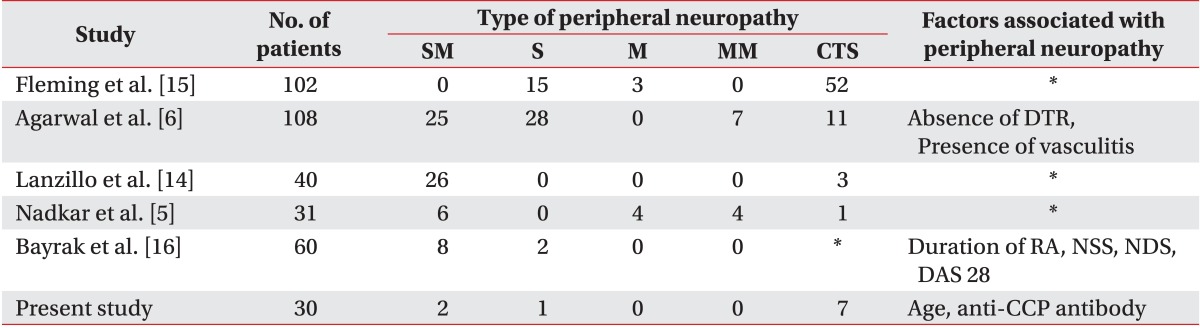
The prevalence and electrophysiological findings of peripheral neuropathy and their relationship with demographic, clinical, and laboratory findings have not been clearly demonstrated in the literature. The prevalence of peripheral neuropathy and its related factors vary among previous studies, as shown in Table 5 [5,6,14,15,16]. Furthermore, it is difficult to compare studies examining peripheral neuropathy in RA because the inclusion criteria and neuropathy assessment methods varied between previous reports. In our current study, we reported a frequency of peripheral neuropathy, including entrapment neuropathy of 33.3% in RA patients, which appears to be lower than that in previous studies with a large series of patients, which included entrapment neuropathy as peripheral neuropathy. The frequency of peripheral neuropathy in this study was higher than the frequency of idiopathic polyneuropathy of 8%, which was reported previously in a population-based epidemiological study [17].
Although we included RA patients with neurological symptoms in our current study, the prevalence of neuropathy in the electrophysiological study was lower than that in other studies. In addition, there was no relationship between the NSS and the presence of peripheral neuropathy, which may be because the NSS consists of questions that focus on positive symptoms, such as burning and tingling, which are subjectively reported by the patients. Furthermore neuropathic symptoms mimic the symptoms of arthritis. Because of these reasons, symptoms of patients might show a poor correlation with results of electrophysiological studies. A poor correlation between the clinical and electrophysiological parameters in our study is in accordance with the results of some studies [6,14], although not all of the studies [18].
In our present study, we did not find a significant association between peripheral neuropathy and gender, RA duration, functional status of patients, RF, ESR, CRP, and type of medication. We found that RA patients with peripheral neuropathy were older than RA patients without peripheral neuropathy. Age is a known risk factor for polyneuropathy [19], and RA patients with peripheral neuropathy in our electrophysiological study showed similar results. However, the prevalence of peripheral neuropathy in patients with RA in this study was higher than that of peripheral neuropathy in patients without the underlying disease.
The important finding of our current study was that patients who were positive for anti-CCP antibody showed an increased risk of peripheral neuropathy. The anti-CCP antibody has become a focus of attention for diagnosis and it is a marker of severe RA [20]. A recent study reported that anti-CCP antibody is associated with human leukocyte antigen (HLA) class II RA-related susceptibility alleles and severe disease manifestations [21]. Although some authors have observed a tendency for a positive association between anti-CCP antibody titer and extra-articular manifestations in RA, there is no data on the effects of anti-CCP antibody on the development of peripheral neuropathy [22,23,24]. Our current study is the first study to investigate the relationship between anti-CCP antibody and the development of peripheral neuropathy in RA patients. According to our results, RA patients who had anti-CCP antibodies have about a 14-fold increased risk of peripheral neuropathy. Also, the effect of anti-CCP antibody on peripheral neuropathy seems to increase with age.
Our study was limited by its small sample size and cross-sectional design. In addition, we were unable to conduct an electrophysiological study for the same duration from symptom onset. Moreover, we were unable to determine a definite cause of peripheral neuropathy and CTS in this study; whether it was as a result of a direct nerve injury due to joint deformity or it was an independent disease. Further longitudinal studies in a large population are needed.
It is difficult to distinguish the symptoms of peripheral neuropathy from those of arthritis, and the subjective symptoms of patients do not correlate with electrophysiological results. Hence, electrophysiological studies should be performed in patients with RA, particular in older patients and anti-CCP antibody positive patients.