INTRODUCTION
Independent ambulation is one of the main goals of stroke rehabilitation. Among the factors that interfere with normal gait in stroke patients are muscle weakness, decreased sensation, impaired coordination, and spasticity of the affected limbs. These post-stroke impairments result in high energy expenditure and abnormal kinetic and kinematic findings, while walking due to forefoot landing, hip circumduction and knee hyperextension [1-3]. Especially, weakness of ankle dorsiflexors usually continues for a long period of time during recovery from a stroke. Among the various methods used to improve ambulation due to ankle weakness, there are also ankle-foot orthoses (AFOs), functional electrical stimulation and peroneal nerve stimulation [4-7].
Custom-molded plastic ankle-foot orthoses (pAFOs) are frequently prescribed for hemiparetic patients with stroke. These pAFOs can easily be inserted inside the shoes and prevent feet from dragging during the swing phase of walking and foot inversion in patients with spasticity. In addition, pAFOs have been reported to significantly improve the gait speed, step length, and balance, when compared with that of barefoot gait [8-10].
In hemiparetic gait after stroke, the foot may externally rotate, causing the affected limb to be out in line with the gait direction. This may lead to decreased stability and gait speed [11]. Two studies showed that external rotation increases when wearing pAFO [12,13]. The exact mechanism is unknown, but Joo et al. [12] reported that external rotation of the paretic foot results from decreased internal rotation of the hip and increased external rotation of the ankle joint. Although pAFO improves gait speed and stability, correction of this external rotation of the foot may further improve the efficiency of hemiparetic gait with pAFO. Therefore, we have modified a pAFO by opening the calcaneal area, resulting in heel-opened ankle-foot orthosis (HOAFO). Our hypothesis was that HOAFO may reduce external rotation torque by allowing heel cushion and providing sensory feedback, without influencing the ankle stability. We investigate the effects of HOAFO on hemiparetic gait after stroke, especially on external foot rotation during stance phase, and compared the results of HOAFO with those of conventional pAFO and barefoot gait.
MATERIALS AND METHODS
Participants and clinical measurements
A total of 15 hemiparetic post-acute stroke patients were recruited from the inpatient rehabilitation department of a tertiary hospital. All of the study subjects had a first onset stroke diagnosed by brain magnetic resonance imaging. Patients were included if they were able to follow a command for more than 2 stages; if they could walk independently regardless of their usual use of a cane; and if they had Modified Ashworth Scale (MAS) 1 to 3 spasticity of the affected ankle and weak ankle dorsiflexion of less than grade 3. Exclusion criteria were severe ankle spasticity or contracture, visual defects or severe hemineglect, unstable medical conditions, or other musculoskeletal or dermatologic problems, such as pressure ulcer in the affected lower limb. The local research ethics committees of our hospital approved the study, and informed consent was obtained from all study subjects.
Patient's age, sex, affected side, and onset duration of stroke were obtained from a review of medical records, and proprioceptive sensory function was measured by physical examination performed by a single physiatrist. We initially measured the impairment or function of the affected limb using several tools. The MAS was used to measure the grade of spasticity in the ankle plantarflexors of the affected side [14]. Motor recovery and function of the affected lower limb were measured using the Brunnstrom stage and Motricity Index (MI), respectively [15,16]. The Berg Balance Scale (BBS) was used to assess the balance of subjects [17].
Procedure
Design of HOAFO
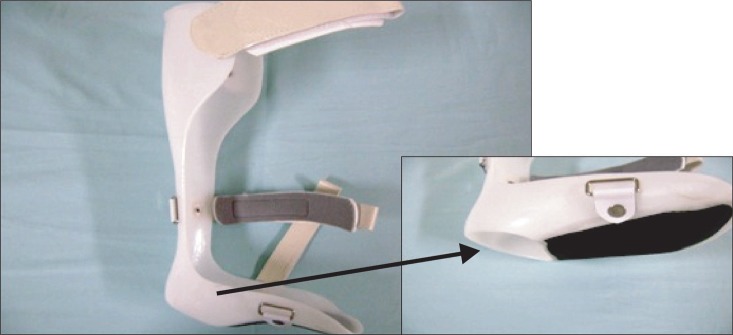
The conventional pAFO frequently prescribed at our rehabilitation center for stroke patients with spasticity is made of 4 to 4.5 mm thick polypropylene. The ankle is a 90° and non-articulated. The length of AFO is about one inch below at the fibular head, with the end of the foot plate located just distal to the metatarsal head. The HOAFO was made of the same material with the same structure, except for cutting the heel area. Part of the heel was cut to expose the calcaneal surface of the rear-foot for sufficient weight-bearing during the stance phase, but was not extended upward to maintain the stability of the ankle joint (Fig. 1). Concrenalysis, it was cut at the half level of calcaneus in an upward direction and transverse tarsal joint area in the front. Three different sizes of pAFO and HOAFO were made, with each subject wearing the orthosis with the best fit. Subjects who already had pAFO or HOAFO wore them during gait analysis.
Gait analysis
Gait analysis was performed using a motion analysis system (Eagle Digital System; Motion Analysis, Santa Rosa, CA, USA), consisting of six Eagle infrared cameras, two force plates (Advanced Mechanical Technology Inc., Watertown, MA, USA), an Eagle hub (100 Mbps), and an analyzing computer. Spatiotemporal parameters and kinematic data were obtained by the infrared camera, which recognized the markers attached to each subject's body. A total of 19 markers were attached to the subject's lower body segment, including the pelvis, both mid-thighs, knee joint, mid-point of lower leg, ankle, and foot. Foot markers were placed at the medial and lateral malleolus, mid-point of the heel, and between the second and third metatarsal head. Each subject was asked to walk in three conditions: 1) barefoot, 2) with a pAFO, and 3) with an HOAFO at a self-determined comfortable speed without wearing shoes. The order of the 3 tests was randomized by a block randomization method. The subjects were allowed to walk back and forth five times before recording to familiarize themselves with their orthoses, and they were also allowed to rest for 5 minutes between conditions.
Spatiotemporal parameters included cadence, walking speed, stride length, step width, percentage of single limb support (SLS) and percentage of double limb support (DLS). Kinematic data on the transverse plane were obtained to investigate the external rotation of the pelvis, hip, and foot. The mean angle of rotation during the stance phase was calculated by averaging the maximal angle at three phases of the stance phase: loading response (0%-10%), midstance (10%-50%), and terminal stance (50%-60% of gait cycle). The angle of foot progression was defined as the angle between the line of progression and the line connecting the midpoint of the second and third metatarsal heads and the midpoint of the heel. For convenience, angles of internal rotation were defined as positive (+), and angles of external rotation as negative (-). After gait analysis, each subject was asked about their preference between the two orthoses.
Statistical analysis
A statistical analysis was performed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). The gait parameters of the three conditions were compared using repeated measures analysis of the variance (ANOVA). If repeated measures ANOVA showed statistically significant differences between conditions and multiple comparisons (Tukey test) were performed. A p-value<0.05 was considered statistically significant.
RESULTS
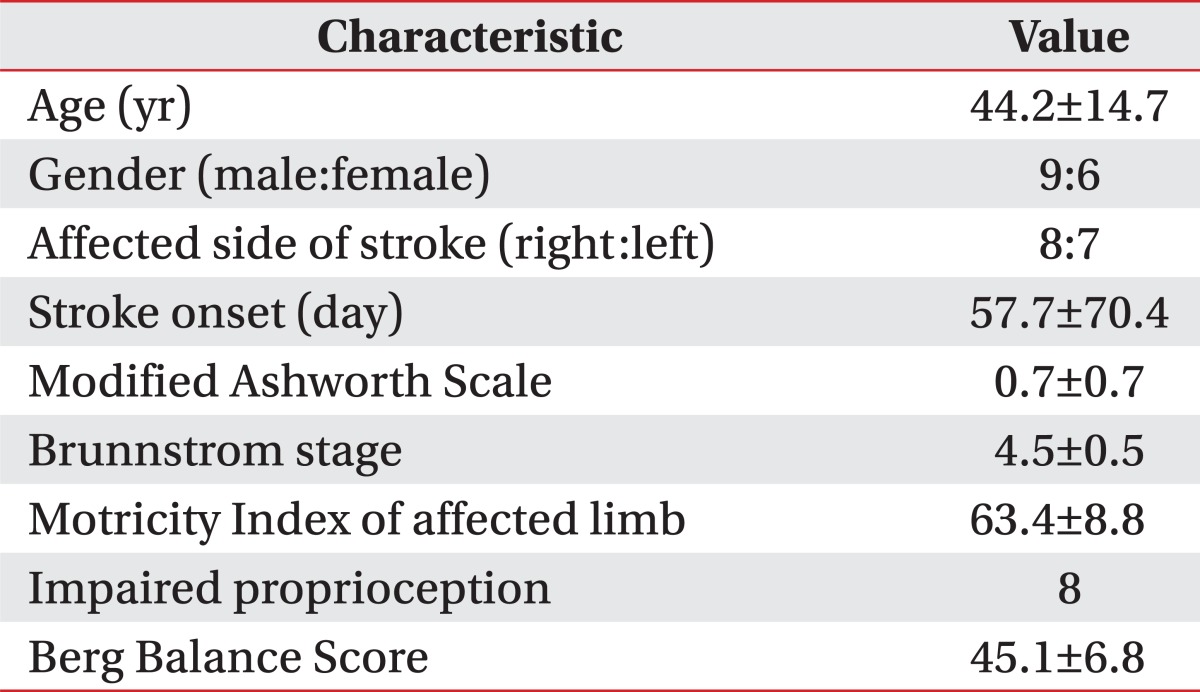
Fifteen subjects consisted of nine males and six females, with the mean age of 44.2 years (range, 23-64 years) and average post onset duration of stroke of 57.7 days (range, 25-300 days). Eight subjects had right hemiparesis and seven had left hemiparesis.
All 15 subjects had some spasticity, but not severe on the ankle plantarflexors and their motor function, and recovery were generally good on the basis of their Brunnstrom stage, MI, proprioception, and BBS score. Table 1 summarizes the demographic and clinical characteristics of these subjects.
Table 2 shows spatiotemporal parameters of the 3 AFO conditions. Walking speed (p<0.01) and percentage SLS (p=0.04) were significantly higher with HOAFO than with barefoot walking. In contrast, cadence, stride length, step width, and percentage DLS did not differ significantly among the three walking conditions.
Kinematic data of pelvic rotation angle on the transverse plane also did not differ significantly among the three conditions. During barefoot and HOAFO walking in the stance phase, the hip rotation angles were 1.38° and 0.78°, respectively, and the foot progression angles were -15.67° and -17.99°, respectively, with neither of these differences being statistically significant. In contrast, on pAFO walking, the mean angles of hip rotation and foot progression were -3.35° and -23.68°, respectively (Table 3). Both hip external rotation and external foot progression were significantly higher after wearing the pAFO (p<0.05) than on barefoot and HOAFO walking. While wearing pAFO, 10 subjects showed maximal external foot progression angle at the loading response. When we assessed the patient preference, we found eight preferred HOAFO, two preferred pAFO, and five reported little difference between them.
DISCUSSION
This study showed that, in hemiparetic stroke patients, the angle of foot external rotation of the affected limb was significantly lower while walking with HOAFO than with pAFO during the stance phase. Since hemiparetic stroke patients who already have pAFO showed excessive external foot progression during gait with pAFO, heel opening of pAFO may be effective without increasing costs or shoe modification. Although there were studies using modified shoes to reduce foot external rotation, the shoes were either bulky or expensive [12,13].
Gait pattern analysis comparing AFO with its absence is usually performed in the sagittal and frontal planes, with few studies reporting gait analysis on the transverse plane in patients with stroke. We were concerned about the excessive external foot rotation during the stance phase of gait in patients who wore pAFO. In a previous study, the hip was in a neutral position at its initial contact, with peak internal rotation occurring at the end of the loading response and peak external rotation at the end of pre-swing [18]. Another study showed that hip external rotation occurred at the terminal stance and remained externally rotated during the swing phase. Internal rotation of the hip occurred just before the initial contact, remaining until the terminal stance. These gait patterns were observed in most study subjects, with the average transverse rotation being 13° [19]. Electromyographic analysis showed that the hip abductor muscles, including the gluteus medius, upper gluteus maximus, and tensor fascia lata muscles, were activated during the initial half of the stance phase. Prolonged action of the semimembranosus during these phases maintained the thigh in an internally rotated position resisting the abductors [20]. In statistical results, we found that external rotation of both the hip and foot were increased in subjects who wore pAFO. However, when the degree of rotation was analyzed, external rotation of the foot was greater than the hip. This increase may have been due to the weakness of muscles of the affected limb and increased external rotation torque due to the solid plastic surface at the heel of pAFO during the loading response by decreasing frictional force.
Pelvic movement during gait is another important factor associated with energy efficiency and normal walking [21]. The pelvic rotation angle during comfortable walking has been reported to be about 11.5° in healthy subjects, but was decreased in elderly subjects. Decreased pelvic rotation may decrease stride length and gait speed in elderly individuals [22]. Studies of pelvic rotation in stroke patients, however, have not shown consistent results [23,24]. In one study, pelvic rotation in stroke patients did not differ from that in the normal control subjects, and could be larger or smaller, suggesting that pelvic rotation was not an appropriate tool for evaluating gait pattern in stroke patients [23]. Another study found that stroke patients who had slow walking speed showed pelvic retraction (external rotation) during the stance phase [24]. In the present study, we found that external pelvic rotation during the stance phase was uncertain among the three conditions of walking. Pelvic rotation may have affected the speed and efficiency of gait, but wearing pAFO or HOAFO did not affect pelvic movement of the affected limb in our study. The mechanism underlying this phenomenon warrants further investigation in the assessment of pathologic gait after hemiplegic stroke.
About 70%-80% of stroke patients can walk short distances independently, but only about 50% can walk longer distances; moreover, most of these patients have decreased gait speed, stride length, and stability and increased energy expenditure [25,26]. Wearing pAFO is frequently used to increase gait stability and improve walking function. Our results did not show that wearing pAFO resulted in statistically significant improvements; although, most parameters were generally better than those observed during barefoot walking. Each of our study subjects walked comfortably, but not at maximal speed, during gait analysis. Spatiotemporal parameters showed that wearing HOAFO also improved all parameters, with gait speed and percentage of SLS being significantly improved compared with barefoot walking. These findings indicate that HOAFO may provide additional effects on gait, compared with pAFO, by decreasing external rotation of the hip and foot during stance phase; thereby, improving gait function in patients with hemiplegic stroke.
This study had several limitations. First, the relatively small sample size may have contributed to the lack of significant differences in spatiotemporal parameters and kinematic data. Second, we evaluated only the affected limb and kinematic data on the transverse plane. The angle measured in the transverse plane may have more errors than the values of frontal or sagittal plane, but most subjects of our study showed consistent results. Third, some subjects were not well fitted to these orthoses because only three sizes of pAFOs and HOAFO were available. Fourth, the gait analysis was not performed wearing shoes. Finally, despite the 3-dimensional gait analysis that resulted in improvements in the external progression of foot angle during stance phase after wearing HOAFO, we did not assess the exact mechanism of these improvements. Therefore, additional studies are needed to clarify these mechanisms and to develop other methods to reduce this phenomenon.
In conclusion, we found that HOAFO was superior to pAFO for reducing hip and foot external rotation during the stance phase of the gait cycle in patients with post-stroke hemiparesis. In addition, HOAFO significantly improved gait speed and the percentage of SLS compared with that of barefoot walking. HOAFO may, therefore, be useful for patients with excessive external rotation of the foot during the use of a conventional pAFO and may be created by cutting the calcaneal area of the latter.