Drug Induced Parkinsonism Caused by the Concurrent Use of Donepezil and Risperidone in a Patient With Traumatic Brain Injuries
Article information
Abstract
A 69-year-old male patient with previous history of traumatic brain injury 5 months ago was admitted to the Department of Neuropsychiatry because of aggressive behavior and delusional features. After starting on 2 mg of risperidone per day, his delusion, anxiety, and aggressive behavior gradually improved. Two weeks later, he was given 10 mg of donepezil per day for his mild cognitive impairment. After 6 weeks of admission in the Department of Neuropsychiatry, he showed parkinsonian features including difficulty in walking, decreased arm swing during walking, narrowed step width, scooped posture, bradykinesia, tremor, and sleep disorder. To rule out the primary Parkinsonism, dopamine transporter imaging technique [18F]fluoropropyl-carbomethoxy-iodopropyl-nor-β-tropane positron emission tomography-computed tomography (18F]FP(IT PET-CT)) was performed, and dopamine transporter activity was not decreased. We considered that his parkinsonian features were associated with the combination of risperidone and donepezil. Both drugs were stopped and symptoms rapidly disappeared in several days.
INTRODUCTION
Traumatic brain injury (TBI) has a wide range of influences on brain functions including motor, sensory, language, and cognitive functions. Especially important, the impairment in cognitive functions cannot affect the outcomes of rehabilitation in a negative way [1]. Accordingly, various medications have been used in the cognitive impairment after TBI to improve the cognitive function and to facilitate the greater functional outcomes in a rehabilitation setting. Cholinesterase inhibitor including donepezil, rivastigmine, and galantamine have been frequently used for the improvement of memory, concentration, thinking, and learning, whereas antipsychotics such as risperidone have been indicated for behavioral disorders after TBI. These medications with different purposes have been used in combinations usually according to the patient's symptoms, and there has been no previous report of adverse effects of this combination. We hereby report a rare case of Parkinsonism induced by the use of the donepezil and risperidone in combination, which were used to improve the cognitive impairment and behavioral problems after TBI.
CASE REPORT
A 69-year-old male patient with decreased mental status and headaches after falling down the stairs visited our emergency room on around February 2010. His muscle strength was relatively preserved over a good grade on his all extremities. On the computer tomography of his brain, subdural hemorrhage on the right parietal lobe and the left frontal lobe, subarachnoid hemorrhage on the bilateral temporal lobe, and fracture on the right parietal bone were found (Fig. 1). The diagnosis of TBI was confirmed. He was admitted to the Department of Neurosurgery for a conservative treatment, and his mental status was gradually improved from stupor to alert. He started his rehabilitation therapy including proper evaluations from 2 weeks after the injury. On functional evaluation, he could not sit alone nor stand without assist, and these disabilities could not be ruled out from poor corporations or decreased muscle strength. Three weeks after injury, he was transferred to the rehabilitation department, and he started cognitive rehabilitation program. On 5 weeks after injury, his cognitive function was markedly improved, and his Korean Mini Mental State Examination (MMSE-K) score was 21. His functional level was improved accordingly, and Korean Modified Barthel Index (K-MBI) score was improved from 2 to 81. On 6 weeks after injury, we could evaluate his muscle strength precisely, and all his extremities showed over the good grade on manual muscle test. He was able to walk independently, and was discharged.

Initial noncontrast computed tomography (CT) image after the traumatic brain injury. CT image shows subarachnoid hemorrhage on the right parietal lobe (A) and subdural hemorrhage on the left frontotemporal lobe (B).
He received the rehabilitation therapy as an outpatient until 8 weeks after injury, and then he was encouraged to exercise alone at home receiving only outpatient follow-up. However, during staying in his home without serial rehabilitation therapy, his personality took on aggressive and delusional characteristics. His cognitive impairment and aggressive behavior got worse, and he was admitted to the Department of Neuropsychiatry with diagnosis of the delusional disorders on 3 months after his first discharging from the hospital. At the time he was hospitalized again, no auditory or visual hallucination was found; however, he appeared to have anxiety, delusion, and aggressive behavior. The magnetic resonance image (MRI) of his brain showed no additional lesion than the chronic changes from hemorrhages on bilateral cerebral hemisphere of his previous TBI. Accordingly, with the diagnosis of delusional disorder which occurred after TBI, he was treated with 2 mg of risperidone per day. After starting this medication, his delusion, anxiety, and aggressive behavior gradually improved enough to cooperate with the therapists. Two weeks later, he was given 10 mg of donepezil per day for his mild cognitive impairment. After 6 weeks of admission in the Department of Neuropsychiatry, he was transferred to the Department of Rehabilitation for the proper rehabilitation therapy, because he showed problems in his gait. He could walk independently, but he showed no movements in his upper extremities and his step-width was narrow. Additionally, he had scooped posture, bradykinesia, tremor in both hands, and sleep disorder. He complained of difficulty in walking, and he could not start any movement promptly. He had difficulties in all activities of daily living, and K-MBI score was 56/100. These symptoms were characteristics of Parkinsonism, and we assumed that this parkinsonian features were related with the administration of risperidone and donepezil, which were started before the onset of his parkinsonian features. Therefore, dopamine transporter imaging with [18F]FP-CIT PET-CT was performed to distinguish his parkinsonian features from idiopathic Parkinson's disease, and normal dopamine transporter density was observed in bilateral caudate nucleus and putamen (Fig. 2). With this result, we could exclude idiopathic Parkinson's disease, and we diagnosed his parkinsonian features as drug-induced Parkinsonism caused by concurrent use of risperidone and donepezil. We discontinued both donepezil and risperidone, and the parkinsonian features gradually disappeared. He was discharged with much improved functions, and K-MBI score was 75.
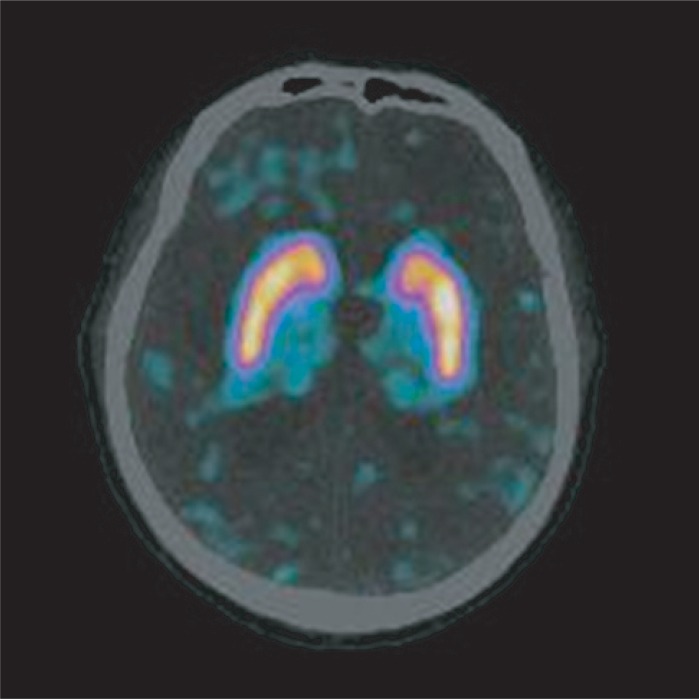
[18F]fluoropropyl-carbomethoxy-iodopropyl-nor-β-tropane brain positron emission tomography-computed tomography image. Normal dopamine transporter density in the bilateral putamen and bilateral caudate nucleus are observed.
DISCUSSION
Risperidone, a kind of atypical antipsychotics, is known to have antipsychotic effect acting as an antagonist of serotonin 5-HT2 and dopamine D2 receptor [2,3]. Atypical antipsychotics have been used safely, because they have relatively low incidence of adverse side effects compared to the typical antipsychotics [4]. These side effects include cerebrovascular disease, anasarca, increased appetite, weight gain, anticholinergic effects, sedation, and extrapyramidal symptoms such as dystonia, akathisia, pseudoparkinsonism, and dyskinesia [5]. Especially, the extrapyramidal symptoms are known to be caused by the drug in a dose-dependent manner; and over 6 mg per day of risperidone has been known to cause such side effects [4]. In our case, the patient received 2 mg of risperidone per day to treat his behavioral problems, and there was no extrapyramidal side effects during the use of risperidone alone. Cholinesterase inhibitors such as donepezil, rivastigmine, and galantamine have been used for the patients suffering from cognitive impairment in vascular dementia and Alzheimer's disease. Among these, donepezil is the most widely used, because it works as a reversible acetylcholinesterase inhibitor with the highest selectivity in the central nervous system, with relatively few side effects [2,6]. Donepezil combines with nicotinic acetylcholine receptor (nAChR) in brain substrate, and then up-regulates nAChR or blocks the neurotoxicity of glutamate [6]. Several studies, including those of Zhao et al. [2] and Reyes et al. [3], have reported that donepezil alone has no serious side effect such as death, and they reported only minor side effects such as digestive problems in most of the patients [3]. Although extrapyramidal symptom could be one of the side effects of cholinesterase inhibitor because of its inhibitory effect on caudate nucleus, it does not usually appear at the general therapeutic level [3]. A case of extrapyramidal symptom after a high-dose administration of donepezil was previously reported, but the dosage of our patient was not high. Our patient showed extrapyramidal symptoms after the use of 10 mg of donepezil, additional to 2 mg of risperidone, and we conclude that this concurrent administration of the two medicines caused the parkinsonian features of the patient. Several cases have been reported on the occurrence of Parkinsonism after concurrent use of different kinds of medication: a case of a cholinesterase inhibitor and antipsychotic drug; a case of tactine and haloperidol [7,8]; and a case of tiapride and donepezil [9]. A case report was published about the parkinsonian features with generalized rigidity 12 days after concurrent use of 5 mg of donepezil and 1 mg of risperidone per day, and these symptoms were disappeared in 1 week after discontinuation of the drugs [10]. This case report is the only case of parkinsonian features caused by the concurrent medication of donepezil and risperidone. As an underlying mechanism causing Parkinson symptoms due to the concurrent medication, it is assumed that it is because that, in the state of antagonism of antipsychotic drugs such as risperidone to D2 receptor, acetylcholine increasing effect is combined and brings about the un balance of acetylcholine and dopamine in the striatum [4]. After discontinuing both risperidone and donepezil, the parkinsonian features of our patient were disappeared within several days. Six months after discontinuing his medications, he showed no parkinsonian features on his follow-up visit to our clinic.
We used [18F]FP-CIT PET-CT to exclude the suspicion of idiopathic Parkinson's disease, which was possible in his age. As [18F]FP-CIT PET-CT is a kind of the imaging for dopamine trasporter (DAT), the main application has been the quantification of the dopaminergic deficit in Parkinson's disease. Also [18F]FP-CIT PET-CT imaging has a high power to discriminate Parkinson's disease from normal aging, because the pathology of Parkinson's disease consists of the loss of dopamine neurons in the substantia nigra and the reduction of dopamine projections to the striatum. The main clinical application of [18F]FP-CIT PET-CT imaging is the differentiation of degenerative Parkinsonism from conditions not associated with dopamine deficit, such as essential tremor and drug-induced, vascular, or psychogenic Parkinsonism. Our study showed normal DAT density of bilateral putamen and caudate nucleus in [18F]FP-CIT PET-CT imaging. We could exclude idiopathic Parkinson's disease and diagnosed his symptoms as a drug-induced Parkinsonism. The DAT imaging using the radiopharmaceuticals is available as the marker of the differential diagnosis as well as the progression and the therapeutic monitoring in Parkinson's disease. The DAT imaging is expected to be successfully applied to several central nervous system disorders with new radiopharmaceutical in the future.
In conclusion, we report a rare case of drug-induced Parkinsonism related with a combination of risperidone and donepezil in a patient after a TBI, which has been reversible by cessation of the medication. We recommend that combination of risperidone and donepezil needs to be carefully applied, as unexpected side effects may be induced.
Notes
No potential conflict of interest relevant to this article was reported.