Fear of Falling in Subacute Hemiplegic Stroke Patients: Associating Factors and Correlations with Quality of Life
Article information
Abstract
Objective
To determine the associating factors of fear of falling (FOF) and the correlations between FOF and quality of life (QOL) on subacute stroke patients in Korea.
Method
Fifty hemiplegic subacute stroke patients in our clinic were recruited. We directly asked patients with their fear of falling and interviewed them with the Korean version of falls efficacy scale-international (KFES-I). We divided the participants into two groups; with FOF and without FOF. We compared these groups with the strength of hemiplegic hip abductor, knee extensor, ankle plantar flexor, functional ambulation category (FAC) scale, stroke specific quality of life (SSQOL), and hospital anxiety depression scale (HADS).
Results
Thirty-four participants were enrolled, and more than half of the patients with subacute stroke had FOF. We compared the patients with and without FOF. According to the results, FOF was associated with the strength of hemiplegic hip abductor, knee extensor and ankle plantar flexor, FAC, total SSQOL, and domains (energy, mobility, self care, upper extremity function) of SSQOL (p<0.05). FOF was also associated with the anxiety score of HADS (p<0.05). KFES-I had a significant negative correlation with the strength of hemiplegic hip abductor, knee extensor and ankle plantar flexor, FAC, total SSQOL, and domains (energy, mobility, self care, upper extremity function) of SSQOL (p<0.01).
Conclusion
The FOF was associated with not only QOL but also with the physical and psychological factors, and in particular, anxiety. Therefore, further concerns about FOF in subacute stroke patients might be required.
INTRODUCTION
Falling is a major threat to stroke patients. Physical injury, such as fracture resulting from falling, has been reported and it could affect the rehabilitation potential and functional recovery.1-3 In addition, the fear of falling (FOF) is as important as falling itself in stroke patients. FOF has also been known to be common in strokes and associated with many negative physical and psychological factors.4-6 It not only affects a simple health concern, but also avoidance of activities and a loss of confidence.5,7-9 In some stroke patients, the experience of prior falling develops FOF.4 However, even though those without such experience suffer psychological or physiological difficulties due to FOF.5,10-19
Prior study showed the several adverse effects of FOF, such as declines in activity, depression, lower quality of life (QOL), and changes in psychological and social functioning.10 In acute stroke patients, more than half of the patients demonstrated FOF. They had higher anxiety and lower QOL in some domains.5 As FOF may impair the rehabilitation outcome and QOL, it is an important issue for patients with stroke.20 Studies prior to this focused on the elderly and patients with neurologic impairment. Studies about strokes were a portion of them, and the length of morbidity was not noted.4-20 In a clinical point of view, rehabilitation is conducted more frequently in the subacute phase, rather than in the chronic phase. This means there is more exposure to fall down injuries. Furthermore, subacute patients differ from chronic patients due to the fact that chronic patients have already adjusted to their disabilities, while subacute patients have not. This means more physical and emotional difficulties. Also, there have been studies about the patient's lower extremity muscular strength or balance sense with the fear of falling, but measuring muscular strength was done with a force plate, which is hard to apply to clinical use.21,22 As a result, the fear of falling in a stroke patient has a huge effect in a patient's life and is frequently studied in overseas; yet, no such study has been done in Korea. In this study, we focused on stroke patients in the subacute phase, questioned their QOL and psychological status, and looked at the relation of FOF with the physical factors that can be easily applied in the clinical field.
MATERIALS AND METHODS
Subjects
Fifty hemiplegic subacute stroke patients (3 to 6 months of stroke duration) were recruited from our clinic from March 2010 to April 2011 with informed consent. The diagnosis of the stroke was based on neurologic examination and findings of brain computed tomography or magnetic resonance imaging studies. We included only the first onset hemiplegic stroke patients who had been able to perform activities of daily living independently until the onset. The questionnaire in this study was made easy such that it can be completed with minimal comprehensive skills. We checked the Korean version Mini-Mental state Examination (K-MMSE) reference value and put into consideration the gender and age factors. An uneducated woman under one standard deviation compared to the mean was 20 points; thus, we selected this value as the threshold of patient selection.23 Patients with 20 points or under were excluded from this study. General characteristics of participants were collected by review of the patients' charts. We measured the FOF, physical and psychological factors, and QOL, as followed.
Experience of falling
We asked patients their experience of falling before and after a stroke. We did not consider the severity of the falling event itself, but investigated the memory of the patient in their falling experience. We intended to investigate the relationship of experience and fear; hence, there was a need to exclude data about episodes of falling that are not in the patient's memory. Thus, data about the falling experience before stroke was limited to episodes that the patient actually had recollection of.
Fear of falling
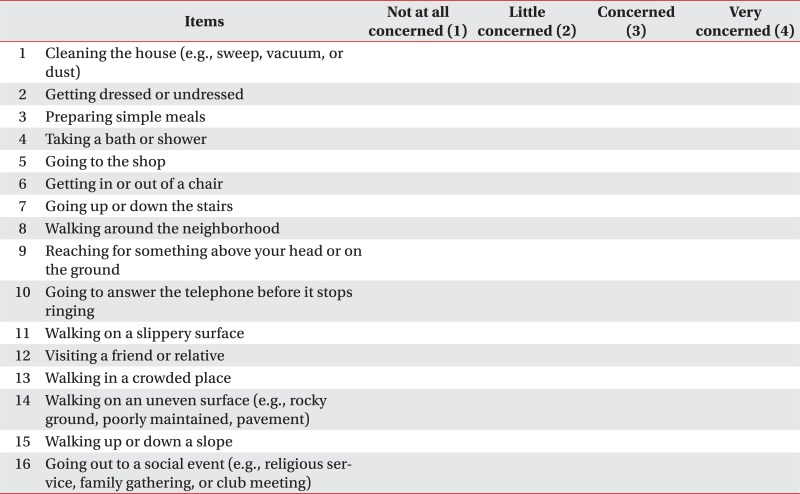
First, we asked the question, "Are you afraid of falling down?"5,24 We also tested the participants with the Korean version of falls efficacy scale-international (KFES-I).25 KFES-I, which was developed to assess fear of falling, is composed with 16 items. Each item is measured with a 1-4 scoring, where a higher score means a higher level of fear of falling (Appendix 1).
Physical factors
The impaired standing postural control is an important risk-factor for falls. In standing and walking, the hip abductor, knee extensor, and ankle plantar flexor muscular strength are important. In other studies, ankle plantar flexor and other ground push off force inducing muscles were shown to be important.21,22,26 Therefore, in this study, the strength of hip abductor, knee extensor, and ankle plantar flexor were measured by the manual muscle test (MMT). MMT is measured on a 0-5 scoring scale; a higher score means stronger power of each muscle. The functional ambulation category (FAC) scale, which was developed to assess the efficacy of ambulation, is measured on a 0-5 scoring scale where a higher score means more independence in ambulation.27
Psychological factors
The hospital anxiety depression scale (HADS) was used for evaluating psychological factors. HADS is composed of anxiety and depression domains. Each domain is composed with 7 items that are measured on a 0-3 scale. A higher score means greater anxiety or depression.28
Quality of life
Stroke specific quality of life (SSQOL) was used for evaluating QOL. SSQOL is composed of 12 domains (self-care, vision, language, mobility, work, upper extremity function, thinking, personality, mood, family, social, and energy). Each domain is comprised with 3-12 items measured on a 1-5 scoring scale. There are 78 items in SSQOL; a higher score means increasing QOL. Both the individual domain and total scores are available to describe the QOL of participants.29
Statistical analyses
The relationship of FOF and other factors were analyzed with Pearson's correlation analysis and chi-square test. The p-values less than 0.05 were considered statistically significant. The SPSS 13.0 program was used for the statistical analyses.
RESULTS
Sixteen participants who gave up on the exam were excluded. Excluding these cases, 34 patients were included in the final study.
Fear of falling
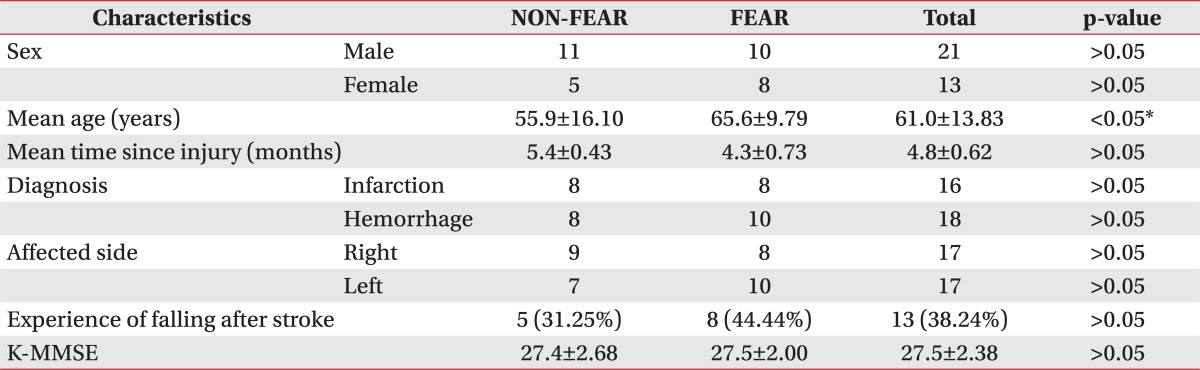
According to the question of "Are you afraid of falling?", 18 participants responded "Yes" (FEAR) and 16 participants said "No" (NON-FEAR) (Table 1).
General Characteristics of Subjects
The differences of general characteristics between NON-FEAR and FEAR
The mean age was higher in FEAR than NON-FEAR (65.56±9.79, 55.88±16.10, respectively, p<0.05). There were no definite differences in factors such as sex, time lapse since injury, diagnosis, and affected side between FEAR and NON-FEAR (p>0.05) (Table 1).
Experience of falling
Only 2 patients reported to have a recollection of falling down prior to their strokes. Both patients had no experience of falling down after the stroke, and thus, had no fear of falling. Therefore, incorporating only 2 cases into consideration within the statistical analysis was not convenient. Hence, we excluded these cases and proceeded the research with falling after stoke. The results regarding FOF and experience of falling were listed on Table 1. The experience of falling after stroke was not associated with FOF (p>0.05).
Physical factors
The FAC scale, MMT of hemiplegic hip abductor, knee extensor, and ankle plantar flexor had statically significant association with FOF (r=-0.673, r=-0.534, r=-0.478 and r=-0.501, respectively, p<0.01) and KFES-I (r=-0.764, r=-0.558, r=-0.546 and r=-0.571, respectively, p<0.01) (Table 2).
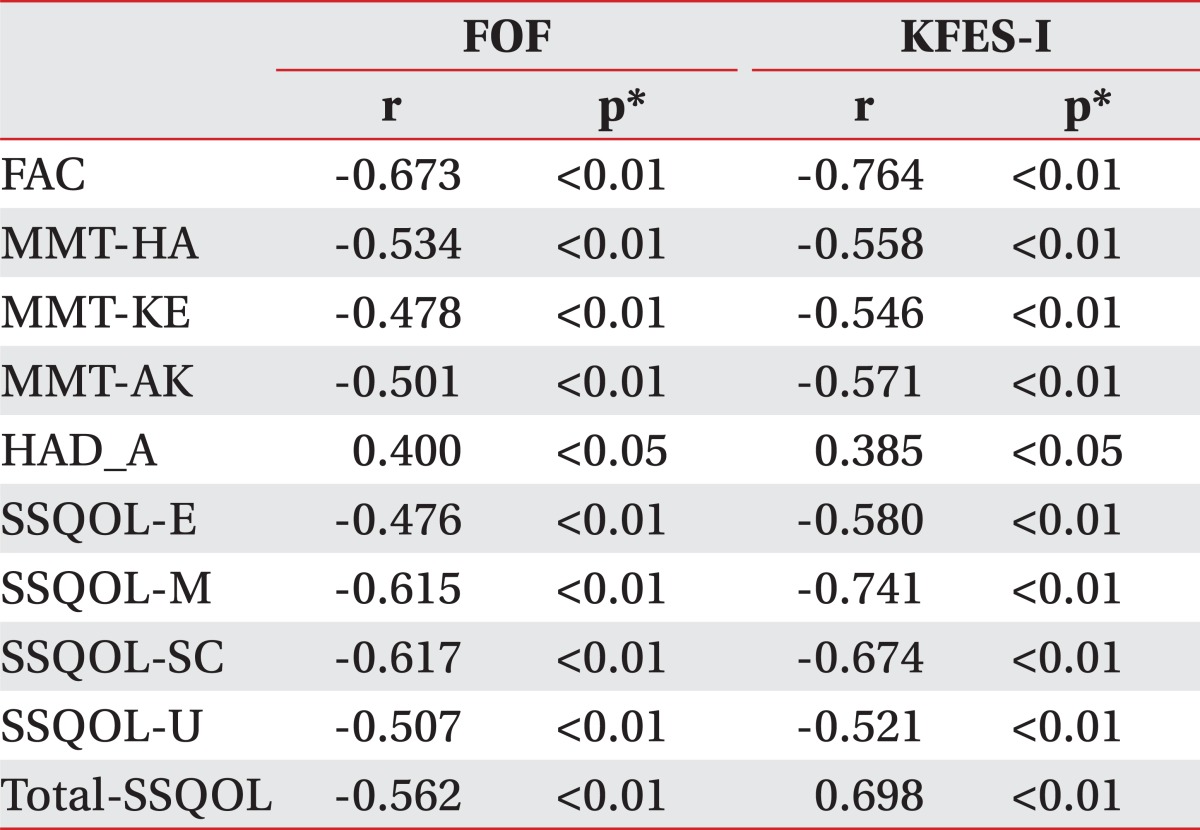
Pearson Correlation Analysis of FOF and KFES-I
Psychological factors
The anxiety score of HADS had significant association with FOF (r=0.400, p<0.05) and KFES-I (r=0.385, p<0.05) (Table 2.). However, the depression score of HADS was not associated with FOF (p>0.05).
Quality of life
Each SSQOL score of energy, mobility, self care, upper extremity function, and Total SSQOL had significant negative correlation with the presence of FOF (r=-0.476, r=-0.615, r=-0.617, r=-0.507 and r=-0.562, respectively, p<0.01) and KFES-I (r=-0.580, r=-0.741, r=-0.674, r=-0.521 and r=-0.698, respectively, p<0.01) (Table 2). Otherwise, other domains of SSQOL (family roles, mood, personality, social roles, thinking, language, vision, and work) were not associated with FOF nor KFES-I (p>0.05).
DISCUSSION
FOF was introduced as the post-fall syndrome, including not only a simple concern of health, but also avoidance of activities and a loss of confidence without sustaining a falling.5 We defined FOF according to the question "Are you afraid of falling down?" that could be helpful for assessing the FOF in previous studies.4,5 In addition, we found that some physical factors, such as FAC, MMT of hemiplegic hip abductor, knee extensor, and ankle plantar flexor, were associated with FOF in subacute stroke patients. In previous studies, a low status of physical factor in the elderly was associated with FOF, which was similar to our results.11,13,17,20
More than half of the patients had FOF in this study. One study showed that more than half of acute stage stroke patients demonstrated FOF in a hospital setting.5 This suggested that FOF might not disappear over time.
There were some studies that associated psychological factors, such as anxiety or depression, with FOF. In our results, although anxiety was associated with FOF, depression was not. Some studies showed the same results; yet, others suggested that there was a relation between depression and FOF.4,5,15,20,30 Thus, there is debate in the relationship of depression and the fear of falling. But regarding anxiety, there is little controversy. We thought that it might be affected by the difference of serotonin pathway between anxiety and depression. As it is already known, dorsal raphe neclues serotonin pathway is related to fear and anxiety. Clinically, there is also a relationship with unlearned fear and anxiety.31 However, depression is also related to serotonin but is known to be associated in another pathway.32 Our conclusion to the controversy in the relationship of depression and FOF is that patient recruitment was done without consideration of these physiological matters. It is interesting that experience of falling after stroke were not associated with FOF and anxiety. Our results showed statistical relevance between anxeity and FOF, and the odds ratio was 0.608. This is consistant with the results from previous research, which stated the relationship between anxiety and FOF.4,5,30,31 Unlearned anxiety predicts that learned fear and FOF might exist with or without prior falling.31 We suggest that the anxiety from the abrupt physical changes after a stroke might induce FOF, which is associated with physical deficit regardless of the experience of falling. Although not showing a high odds ratio, such as quality of life, anxiety and FOF does indeed have a relationship. Thus, controlling anxiety will be a playing factor in controlling FOF.
In the previous study, FOF was only associated with the SSQOL score of thinking, personality, and energy domains.5 However, in our results, the total score of SSQOL as well the domains are associated with body function, such as energy, mobility, self care, and upper extremity function. In addition, KFES-I had a significant negative correlation with the same domains. These differences with the previous study might have originated from the difference of period after a stroke. Unlike our suggestion in the acute phase, patients might be more concerned with physical movements in the subacute phase.
The QOL of patients with stroke was affected by FOF.4-6,13 Furthermore, FOF was associated with not only the physical factors but also the psychological factors, particularly, anxiety. Although further studies are needed, it may be helpful that the evaluation and treatment of these physical and psychological factors with FOF could improve the QOL of the stroke patients. The QOL also had significant associations with physical factors and psychological factors. Since the QOL is the subjective satisfaction, which reflects the overall status including physical and psychological factors, it is important to assess stroke patients.
This study also had other limitations. First, we did not consider the severity of the falling. There can be a more severe falling accident and a less sever one. These must have different effects on the patient; yet, this difference was not considered in this study. Further study should be done considering this factor. Second, the sample size was too small to say that the results of this study represent the subacute stroke patient's frequency of FOF. However, this study emphasized the importance of FOF in subacute stroke patients, and can lead to larger studies that can find out the epidemiologic relationship in the FOF frequency in stroke patients. Third, the polypharmacy induces fear itself, and moreover, 4 or more drugs have a direct relationship with FOF itself. This was not considered in this study because all of the cases in this study took 4 or more drugs. This was due to the fact that all patients were in the subacute phase of a stroke, thus, requiring polypharmacy. Further studies need to examine the relationship between the number of polypharmacy and FOF. Forth, we intended to find out how the experience of falling affects FOF and whether or not stroke changes the physical status of the patient. However, the group was too small to conclude a significant result in this matter. We propose a need for a larger scale study in order to investigate the relationship of the experience of falling before stroke and FOF.
CONCLUSION
The FOF was associated with not only QOL but also with the physical and psychological factors, particularly anxiety. Therefore, further concerns about FOF in subacute stroke patients are essential.
Appendices
Appendix 1
FES-I