INTRODUCTION
Although the position changing maneuver known as "come-to-sit" is routine and performed several times a day, it is one that may present performance challenges after central nervous system (CNS) injury. A person who is unable to take a sitting posture will encounter limitations in activities of daily living (ADL) and will also be problematic for care-givers.1,2 Since the main goal of rehabilitation is to diminish dependency when performing ADLs, retraining of the "come-to-sit" activity is necessary to achieve ADL independence.3
In rehabilitation of CNS injury, the movement between a lying and sitting posture is an essential part of the recovery phase. In order to accomplish tasks such as feeding, washing of hands, grooming and dressing, the patient must achieve a sitting posture, after which advances into transfer activity and gait are possible. In stroke patients, the development of "come-to-sit" activity is divided into three stages: a total assist requiring state, the decreasing of assist, and an independent state. Susan and Kathryn4 analyzed and confirmed this pattern examining selective patterns of trunk movement from a side lying to a sitting posture. Yet assessment of this task has mostly depended on subjective tools such as 'performance-based assessment (PBA)5 or 'the ability for basic movement scale' (ABMS).6
This study was therefore designed to resolve the following issues: first, to devise an objective assessment for "come-to-sit" maneuvers, using quantitative analysis with a specifically designed jacket and a measurement scale. Second, to find the correlation between the subjective assessment tools (PBA or ABMS) and assessment of the side lying posture, for both hemiplegic-side and sound-side lying. Third, to investigate the correlation between the subjective analysis of acquired independence on "come-to-sit" and 'performance-based, ability to basic movement scales' such as the Korean version of the Berg scale (K-BBS),7 the Korean modified Barthel index (K-MBI),8 the Korean mini-mental status examination (K-MMSE),9 and the Brunnstr├Čm stage.10
MATERIALS AND METHODS
Subjects
Twenty two outpatients (14 male, 8 female) with stroke who visited rehabilitation between December 2008 and May in 2009 were enrolled. The mean age was 62.5 years. The subject group consisted of 15 patients with cerebral infarction and 7 with intracranial hemorrhage. 12 patients had left hemiplegia, and 21 were right handed. The average time from injury was 198.5┬▒318.2 days and subjects' average body weight was 60.2┬▒11.9 kilograms. Patients who were unable to obey commands or had limitations in their range of movement were excluded.
Methods
All participants in the PBA and ABMS were tested by same examiner, who was an expert practitioner in the field. Based on PBA5 scales, patients were subdivided into 5 stages: independence, supervision, minimal assistance, moderate assistance and maximal assistance.
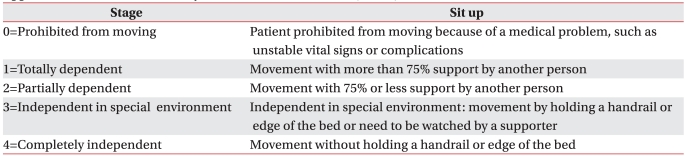
Independence (stage 1) was defined as the 'patient is able consistently to perform the skill safely without no one present', whereas supervision (stage 2) denoted that the 'patient requires someone within arm's reach as a precaution'. Minimal assistance (stage 3) meant that the 'patient is able to complete a majority of the activity without assistance'. 'The patient is able to complete part of the activity without assistance' and 'the patient is unable to assist in any part of the activity' were defined as fourth and fifth stages, respectively (Appendix 1). ABMS scores were organized into five stages based on sitting ability, defined as follows.6 Stage 0 denotes a prohibition from moving because of a medical condition. Stage 1 is a totally dependent stage that requires more than 75% assistance. Stage 2 is partially dependent stage, with a <75% assistance requirement. Stage 3 is the 'independent in special environments' stage, wherein movement by holding a handrail or sitting is possible, and stage 4 is a completely independent stage, wherein sitting is possible without assistance (Appendix 2).
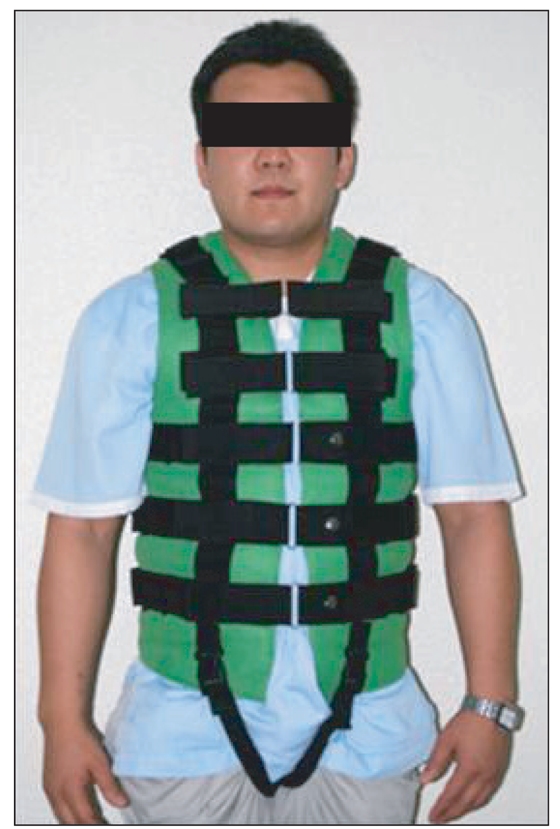
We created a specially designed jacket (Fig. 1) with a hook attached to two scales (Travelon®, Elk Grove Village, USA) (Fig. 2) measuring the maximal value of pulling weight, so that the patient could be pulled in the same direction while sitting constantly with repetitive assessments. The specially designed jacket was tailored in its vest shape by an experienced orthotist and tailored for comfortable fit (Fig. 1). To maintain a constant angle as the patient went from a supine to sitting position, we attached several hooks at the front of jacket to connect the two scales. Through a process of investigation, we determined the best position for the hooks to pull the weight with even distribution.
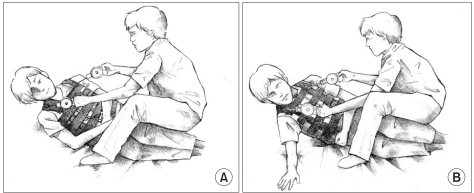
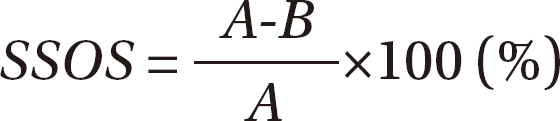
A patient wearing the jacket was ordered to move into "come-to-sit" from a side lying posture, and the examiner supported the patient's buttock with a knee while assisting the patient by pulling the attached scales with both hands. The test was divided into patient with total dependency (Fig. 3-A) and maximal effort to take "come-to-sit" posture independently (Fig. 3-B). The maximum weight loaded on the scale during taking the "come-tosit" posture was measured three times, then calculated on the side lying to sit objective scale (SSOS) using the following equation.
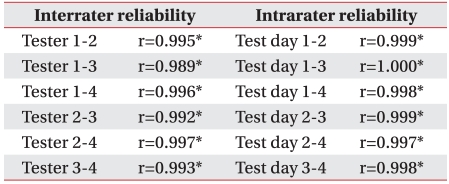
Before proceeding, we performed a pilot study to verify the reliability of the SSOS measurement tool. The pilot study was to determine reliabilities between examiners and within the same examiner's results. The interrater reliabilities among examiners were analyzed by Spearman correlation coefficient (rho) with 4 examiners who used the SSOS with 10 patients. The intra-rater reliabilities for individual examiners were also analyzed by Spearman correlation coefficient, with an examiner performing SSOS measurements four times for 10 patients within 12 hours. The result of this pilot study for the inter-rater reliability among examiners (r, correlation coefficient) was 0.989-0.997 (p<0.01) and the intra-rater reliability (r) within examiners was 0.997-1.000 (p<0.01). These results indicated that the SSOS measurement was highly reliable (Table 1).
Statistical analysis
The movement from side lying to the "come-to-sit" posture was assessed on the sound side and the hemiplegic side, and the PBA, ABMS, SSOS values for these sides were compared through nonparametric analysis. The calculated objective values for the K-BBS, K-MBI, K-MMSE and for the Brunnstr├Čm stages of hand, upper and lower limb were also analyzed by the Spearman correlation coefficient.
RESULTS
Comparison of the values measured from taking the "come-to-sit" posture from a side lying posture on the hemiplegic side or sound side
The PBA values for hemiplegic side lying to sitting were as follows: 2 patients were at stage 1, 4 at stage 2, 4 at stage 3, and 7 at stages 4 and 5. The PBA values for sound side lying to sitting were 1, 1, 2, 1 and 17 patients at the respective stages 1-5. ABMS scores for the hemiplegic side were: 1 patient at stage 0, 5 at stage 1, 5 at stage 2, 6 at stage 3, and 5 at stage 4. ABMS scores for the sound side were 1, 0, 3, 2, and 16 patients, respectively. Since SSOS was measured as 60.9% (┬▒28.0) when sitting on the hemiplegic side and 89.0% (┬▒23.2) when sitting on sound side, these results indicated that lying on the sound side made it easier for patient to take the "come-to-sit" posture. The hemiplegic and sound side values were compared through nonparametric analysis, and all of the PBA, ABMS, SSOS categories showed statistically significant differences (p<0.01). There was no statistical difference between cerebral hemorrhage and cerebral infarction group.
Correlation between SSOS values and subjective assessment tools for hemiplegic side lying
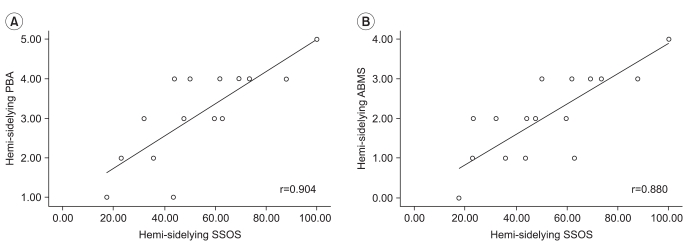
The Spearman nonparametric correlation coefficient analyses between the values of SSOS, PBA and ABMS for the hemiplegic side lying to sit position were as follows: SSOS and PBA (r=0.904, p<0.01) and SSOS and ABMS (r=0.880, p<0.01), showing statistically significant correlations (Fig. 4).
Correlation between SSOS values and subjective assessment tools for sound side lying
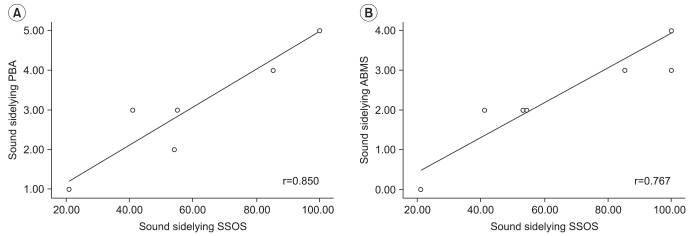
The Spearman nonparametric correlation analyses between the SSOS, PBA and ABMS for the sound side lying to sit position were as follows: SSOS and PBA (r=0.850, p<0.01), SSOS and ABMS (r=0.767, p<0.01). These reflect statistically significant correlations (Fig. 5).
Correlation between SSOS values and functional assessment tools for both hemiplegic and sound side lying
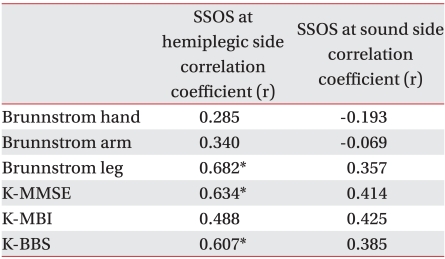
The SSOS for hemiplegic side lying to sit showed statistically significant correlations with the Brunnstrom lower limb stage, the K-BBS, and the K-MMSE when using Spearman nonparametric correlation coefficient analysis (p<0.05), but there were no significant correlations with the Brunnstr├Čm stages of hand and upper limb, or the K-MBI (p>0.05) (Table 2). The SSOS for sound side lying to sit revealed no statistical correlations with any of the examined functional assessment tools.
DISCUSSION
The "Come-to-sit" transfer maneuver is one of the most important basic actions in activities of daily living. If a child with cerebral palsy can sit alone before 2 years of age, the chance of his acquiring independent ambulation is very high. However, if the child is not able to sit alone by the age of 4, he is unlikely walk independently.11 This finding suggests that independent sitting ability has great influence on future activities of daily living.
The reliability of subjective assessment tools rarely surpass those of objective assessment tools, but there has not been sufficient data relating to the previously utilized assessment tools for sitting maneuvers. Quantitative analysis of sitting maneuver ability has never been attempted. This study therefore has significance because it is the first to use an objective assessment tool to substantiate the reliabilities of 5 stage measuring methods based on clinical decision through observation.
We invented a new, specially-designed jacket which can constantly measure the level of assistance needed for "come-to-sit". To determine the proper position at which to attach the scale to enable constant weight measurement during "come-to-sit", we analyzed the force of pulling scale, with the aid of physicists. The success of this was proven by the reliability analysis between examiners and within examiners for the assessment tool.
In general, the "come-to-sit" transfer maneuver has three trunk initiation patterns. First, the upper trunk is rotated to the left side due to rotation started from the upper trunk and body weight supported by extension of the upper limb then the forearm. The right upper limb extends furthermore and the left upper limb fl exes more with the left hip and thigh supporting the body weight in lower limbs. The second pattern starts in the lateral lower trunk and the extended arm pattern corresponds with the lower trunk lateral flexion to the left side, the convex to the left side, with weight supported on the unilateral extended arm and body weight supported with the left hip and thigh. Third, the flexed arm pattern starts with the upper trunk in a lateral position, puts the upper trunk in a left lateral flexion position with left convexity, and weight is supported with the unilateral left forearm then with hip and thigh.4
Using quantitatively objective analysis of the "come-to-sit" posture, subjective assessment conducted by an experienced examiner had highly significant correlation with objective assessment in this study. Therefore, it was indicated that subjective assessment by an experienced examiner is suitable for clinical use. However, if examiners are not experienced as those in this study, assessment errors during evaluation could be problematic. Therefore, the development of standardized tools for quantitative measurement, such as the jacket developed in this study, is necessary.
Hemiplegic patients usually depend on their sound side arm to perform the "come-to-sit" maneuver. At present, subjective assessment tools for evaluating the "come-to-sit" maneuver have tended to evaluate the side with less difficulty with regardless of hemiplegic or sound side. We noticed that assessment using the hemiplegic side has more significant correlation with the patient's recovery of functional outcomes in this study. However, this result was not meant to encourage patients to sit on their hemiplegic side, and evaluation of the assistance requirement during the "come-to-sit" maneuver on the hemiplegic side had a more objective relationship with the prediction of patient's recovery.
SSOS values for hemiplegic side sitting had no significant correlation with values related to activities of daily living such as the K-MBI, but the Brunnstr├Čm lower limb stage and the K-BBS showed statistically significant correlation with SSOS values for the hemiplegic side. Based on this correlation, we could assume that a sense of balance and the functional recovery of the lower limb play an important role in performing the "come-to-sit" posture. However, given that there were only 22 participants enrolled in this study, more participants would be needed to generalize these results.
CONCLUSION
By quantization of stroke patient's "come-to-sit" maneuver using a specifically designed jacket and scales, this study is significant in that it is the first to evaluate the reliability of pre-existing subjective assessment tools. It found that assessment of the hemiplegic side lying to sit maneuver has more advantages for predicting the progression of patient's functional recovery over the routinely performing assessment of the sound side lying to sit maneuver.