INTRODUCTION
In a patient suffering with severe disorders of consciousness, it is important to evaluate the condition of consciousness properly. Since a patient in a vegetative state (VS) is characterized by the return of arousal without responses to peripheral stimulation, being incapable of conscious action, they have been excluded from rehabilitation that is intended for regaining consciousness through repetitive training or learning. Minimally conscious state (MCS) differs from persistent vegetative state in that the patient is capable of conscious actions more than reflexes, which includes following some orders or chasing after something with eyes.1 Such a level of consciousness may be a phased standard that would eventually develop into a better condition of consciousness or rather a case of marking time without change of state, which requires an active approach to change the diagnosis of consciousness. Occassionally patient confirmed to be in a vegetative state could be rediagnosis as MCS, which propose a positive prognosis in a patient.2 If it were possible to investigate an indication of potential learning in a patient who has been determined to be in a vegetative state, we could also confirm the change of consciousness level via Coma Recovery Scale-Revised (CRSR) on the state of consciousness, and accordingly we should be able to select a proper rehabilitation scheme for treating the patient.3 Thus, by performing training using microswitch which can be controlled by tiny movement the authors were able to re-diagnose a patient to have MCS and observed improved progress.
CASE REPORT
A patient, in this case a 65-year-old female, with traumatic subarachnoid hemorrhage and intracranial hemorrhage in the right frontal lobe and temporal lobe-parietal lobe due to a traffic accident in 2009, underwent a craniectomy as well as a hematoma and was in a coma for 2 months after the accident. The patient awoke from the coma and experienced a sleep-wake cycle but was diagnosed to be in a vegetative state for 10 months until she was admitted to this hospital.
The patient scored 6 in the Glasgow coma scale (GCS) and 4 in the Coma Recovery Scale-Revised (CRSR) at the time of hospitalization, demonstrating eye blinks to stimuli for visual and auditory startle reflexes but not to a pain stimulus. Our subject's sleep cycle remained in the form of wake in presence of light but sleep in absence of light. The patient had a percutaneous gastrostomy for nutrition, retaining a suprapubic foley catheter and also underwent tracheostomy. On visual evoked potential, the right side was normal, however a delayed response was observed from the left side. On auditory evoked potential, since there was a response only on the left side with 50db SPL intensity, the right eyesight of the patient was used assuming that she could hear sound because of left-side hearing ability.
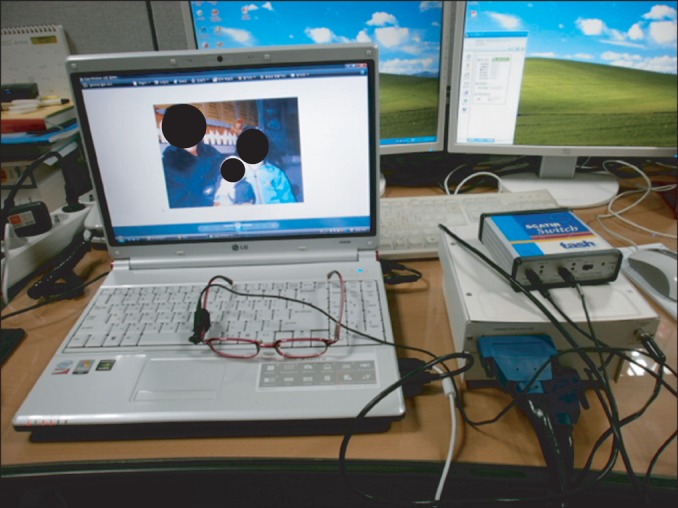
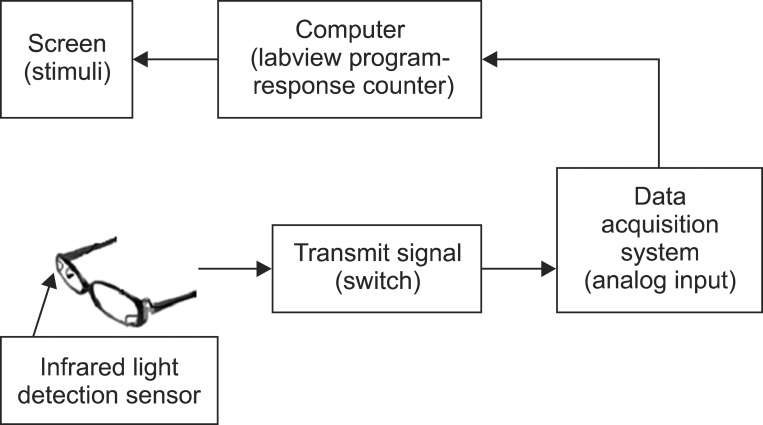
Microswitch-based technology identifies patient response to diverse sensory stimuli. In this case, we used it analyze blink response of the patient to visual and auditory stimuli. Since a patient with decreased motivation can be underestimated3 and the stimuli introduced were comprised of items particular to her liking. Pictures of granddaughters and recordings of her voices as well as certain hymns of the patient's liking were made into a video to give visual and auditory stimuli simultaneously. The patient was fitted with eyeglasses that contained a sensor which determines blink by sensing infrared rays reflecting off the patient's eyeball, attached on the right-side rim of the eyeglasses. This was fixed for sensing from the same position throughout the study. An electronic machine, which converts the blink sensed by the sensor into an electrical signal, was connected to computer to measure the frequency of blinks and receive feedback (Fig. 1). The video was set to be reproduced both at a certain time interval in addition to each time it received feedback. Eye blinking, a scale for evaluating the level of response based on its frequency, can also be a switch for reproducing the video on the basis of setting (Fig. 2).
To invoke the patient's response prior to actual testing, stimulus for visual startle reflex was introduced before her eyes. The research proceeded with the ABABCB method where A is based on the time period of giving no stimulus after evoking visual startle reflex, B is the process in which stimulus given evokes another stimulus with feedback of patient response, and C is the process in which stimulus is provided at a fixed interval regardless of patient response. With one session for 120 seconds, one period was composed of several sessions. We arranged times of sessions according to the patient's medical condition and the experiment was executed for approximately 10-30 minutes a day in the order of A1B1A2B2CB3 for each turn, for 3 to 5 days a week for 5 weeks. Sessions increased as the patient's condition improved. The A1 period was 11 sessions and the A2 period was 17 sessions. B consisted of three periods including 16, 24 and 7 sessions, while C consisted of a single period that including 7 sessions.
Frequencies of patient response in our study were presented in Table 1, where the average frequencies of period A were 10.08, B and C were 20.71 and 8.7 respectively. The frequencies of period B were significantly higher compared with other periods (p<0.05) (Fig. 3). Upon completing the research study, the patient CRSR score rose to 10 points form 2. For improved items, when a sound was introduced to the left side, the patient responded with a movement of turning the neck to the left; when a picture was shown moving in the up and down directions, the patient's eyeball moved in the same manner, following the image; when the limb was pinched, her right hand and foot moved towards that pain; when the lips were pressed smoothly with a tongue depressor, she showed an oral reflex movement (smacking her lips).
DISCUSSION
Increase in times of response for period B, compared to period A, illustrate that the patient reacted by sensing the change of environment from the stimulus. Since period B was set for the patient to evoke stimulus by feedback, a greater response as compared to period C, which was given no feedback, can be explained as the result of learning effect that the patient realized stimulus had been connected to her response. This proves the patient has the ability to learn, suggesting the presence of consciousness, and becomes the basis for re-diagnosing her to be in MCS from the existing vegetative state.4 In identifying MCS in patients diagnosed as being in a vegetative state, CRSR provides more specificity than GCS.2 In our study, CRSR score was measured before and after the experiment to evaluate if there was a sign in the patient's consciousness to be determined as MCS, which resulted in a significant increase in the score. Of these, movement of the right hand and foot response to pain and visual pursuit are the reflections of both the motional function scale and visual function scale, and correlate with the result of this study in that CRSR score can also be a useful scale n determining MCS.5
To identify MCS in patients with serious brain damage is a challenge. Moreover, patients with MCS can have their cognitive ability underestimated because they have a language disorder, loss of sensory or motor function, and derived lower desire.1 According to the literature, it is reported that in 43% of patients diagnosed as being in a vegetative state, conscious movements requiring re-diagnosis have been observed. Regardless of brain damage mechanism, misdiagnosis is more often in chronic than acute patients, while the most frequent misdiagnosis was caused by failing to sense the patient's conscious eye blink.6 This suggests difficulty in distinguishing whether a patient's eye blink is an awareness movement or not. Natural course or long-term prognosis for patients in MCS is not well known yet, but they seem to offer better a prognosis than those in the vegetative state, and a recent report claims that in many cases improvement occured even one year after attack.7 Thus, in the case of misdiagnosis as a vegetative state, it can have a negative effect on determining patient prognosis, often leading to neglect of rehabilitation. In this study we were able to re-diagnose vegetative patient as MCS by revealing her blink is conscious acting.
Unlike this case report which showed the effectiveness of learning, another study suggested that an increase of responsiveness during stimulation is significant itself even without a feedback response.8,9 Even if sign of learning like a feedback response has not been found in a patient, increase in times of response to stimulus suggests the presence of consciousness in a patient. Despite the difference, those studies share the common aspect that the presence of consciousness determines MCS.
Further study is needed to universally apply this learning practice using microswitch-based technology. In this case, it is difficult to ascertain whether improvement of the patient's condition and increase of CRSR score were the result of a natural course or rather of the learning practice. Nonetheless, this case will prove to have a positive effect on the progress of the patient as a starting point for suggesting a new rehabilitation scheme because it diagnoses patients for MCS more positively and performs learning practice on those with limited rehabilitation.