INTRODUCTION
Flank pain is commonly the result of one of three conditions, urinary tract infection, kidney stone, or musculoskeletal disorders [1]. Intraurinary causes of flank pain usually include stimulation of the visceral afferent nerve upon distension of the ureter or renal capsule [2]. Abnormal radiologic findings for the genitourinary system play a critical role in diagnosing the problem. However, similar pain can be caused by extraurinary abnormalities, and it is difficult to distinguish it from the pain originating from the visceral structure. Physical examination plays a crucial role in identifying the location and characteristics of the pain.
Thoracolumbar junction (TLJ) syndrome is often characterized by pain around the iliac crest in the inguinal or lateral thigh area. This may result from dysfunction in the T10ŌĆōL2 vertebral segments of the TLJ [3]. The vertebral segments responsible for visceral pain in the kidney are almost identical to those involved in TLJ syndrome. The clinical features of the two diseases may be similar [4,5].
We describe a patient with flank pain around the iliac crest, initially considered to be caused by renal artery stenosis. Although the anatomical problems were resolved by angioplasty, the pain persisted and eventually improved by treating TLJ syndrome.
CASE REPORT
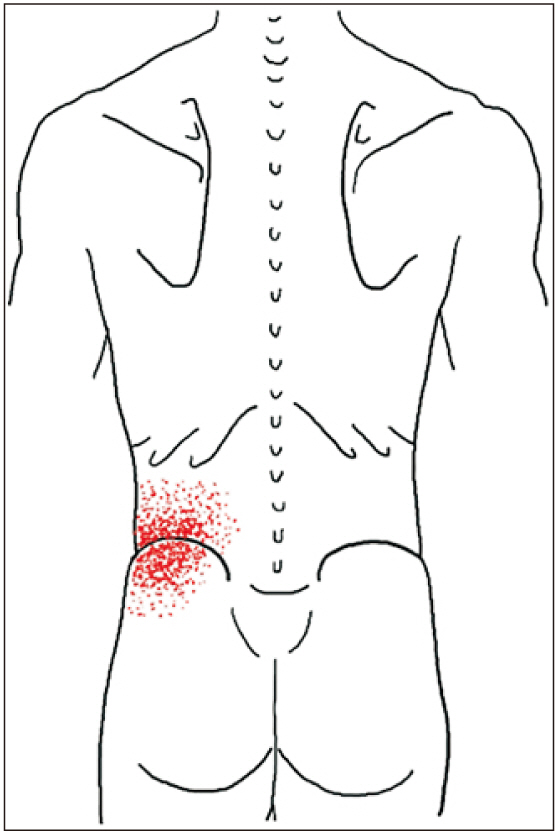
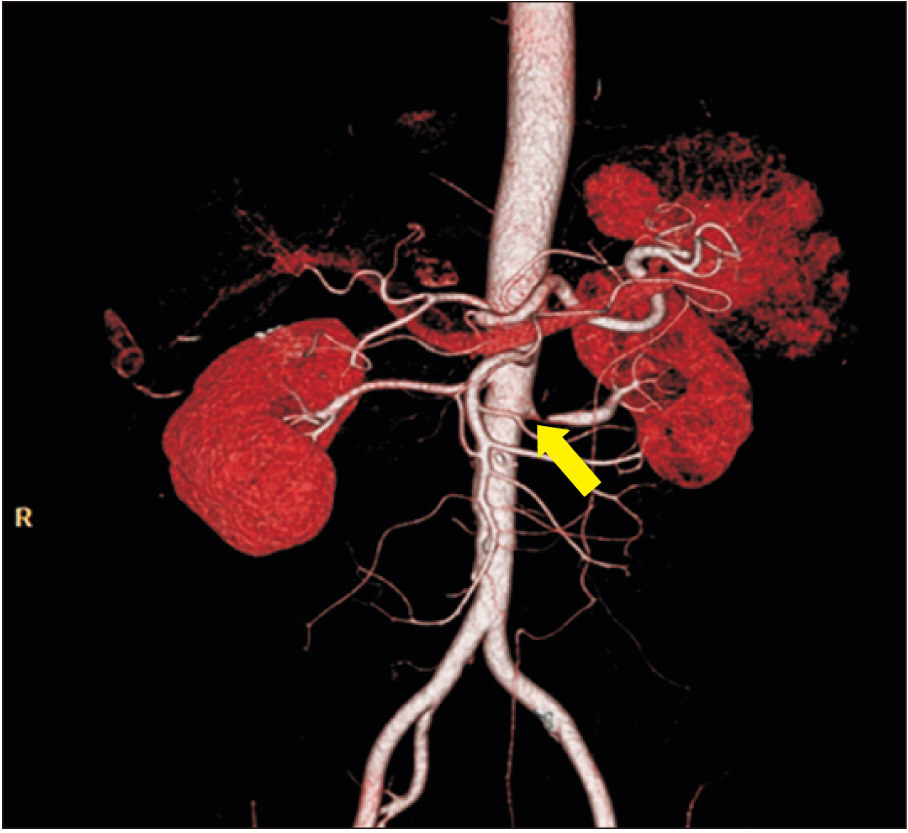
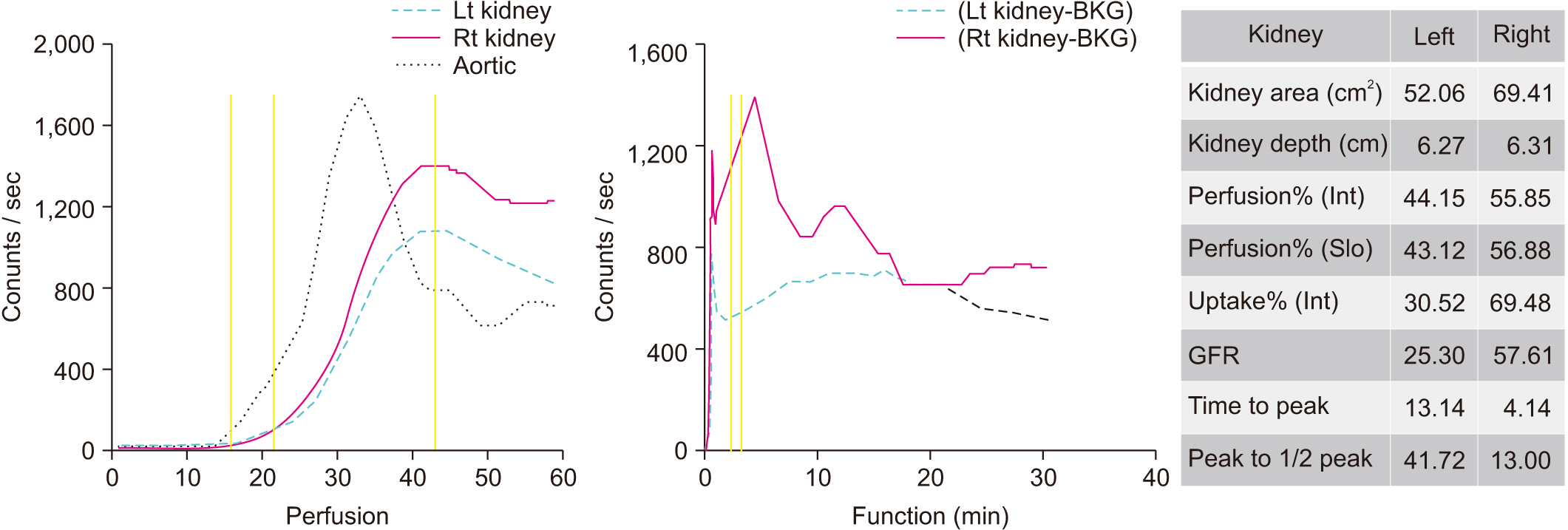
A 54-year-old male visited the urology outpatient clinic with left flank pain experienced for 1 week. He had no history of urinary stones and a 5-year history of hypertension with medication. He complained of sharp pain in the left flank and iliac crest areas (Fig. 1). The pain was rated at 10/10 on the Numeric Rating Scale (NRS). Initially, he visited a local clinic and was administered medication for pain control. However, he was referred to our hospital as there was no significant improvement in his symptoms. To evaluate the potential intraurinary causes, he was admitted to the department of urology. Several tests, including routine urine analysis, blood tests, and X-ray were performed. Although there was no evidence of common intraurinary lesions, such as a urinary stones or urinary tract infection, he constantly complained of intense pain. He underwent abdominopelvic computed tomography (APCT), which indicated severe stenosis in the proximal portion of the left renal artery (Fig. 2). There were no abnormal findings in the spinal discs, facet joints and paraspinal muscles in APCT. Renal scan (Tc-99m DTPA [diethylenetriamine-pentaacetic acid]) was performed to evaluate his kidney function. It revealed that the glomerular filtration rate of left kidney was decreased (Fig. 3). The patient underwent percutaneous transluminal angioplasty, wherein a stent was inserted into the left renal artery. Pain improved by 5/10 on the NRS, after intervention. Two days later he was discharged home.
However, the day after he was discharged, he returned to the emergency room with severely aggravated pain of 8/10 on the NRS and was readmitted to the cardiology department. Flank pain worsened again despite stenting having been performed on the last admission, which was considered the cause of pain. The physician considered a musculoskeletal disorder.
A consultation with the rehabilitation department was conducted. During the physical examinations, tenderness was observed at each level of the left deep paravertebral muscles (DPVM) at the T10ŌĆōT12 vertebrae. Local hyperalgesia on the skin over the left flank and iliac crest was identified when a fold of skin and subcutaneous tissue was pinched and rolled. Based on these findings, flank pain was thought to be the result of TLJ syndrome.
To correct the dysfunction of the TLJ segment, injections targeting the multifidus were administered, which plays the biggest role in the DPVM. Each needle was placed 1ŌĆō1.5 cm lateral to the spinous process at the depth of the lamina. After touching the lamia, the physician pulled the needle approximately 5 mm backward and injected 3.5 mL of 0.25% lidocaine at each level. One area was injected per muscle and each of 3 levels were injected. There was no risk of blood vessel or nerve damage as the injection was completed after contact with the lamina bone. The average injection depth was approximately 3.5 cm. The next day the patient reported significant pain relief and a decreased pain score from 8 to 3 on the NRS. A second injection had the same way. Following the second treatment, the patient was discharged home. When he visited the outpatient clinic 9 days after the second injection, the flank pain had resolved almost completely. As there was remaining tenderness in the left T10ŌĆōT12 DPVM, an additional treatment was performed at these levels. Five days after the third injection, flank pain was completely resolved, and no recurrence was detected at the regular checkup at the cardiology department after several months.
Patient has provided informed consent for publication of the case.
DISCUSSION
We report a 54-year-old male who experienced acute flank pain accompanied by renal artery stenosis and TLJ syndrome. Clinically, it is difficult to determine the cause of flank pain for the following reasons.
Afferent impulses from the kidneys are primarily transmitted through the preganglionic sympathetic nerves to the spinal cord at the T10ŌĆōL1 levels [6]. Renal ischemia, such as renal infarction and renal artery stenosis, can induce pain via the afferent nerve pathway to the spinal cord [1,5]. Additionally, there are many trunk muscles, which can be a cause of flank pain. The cutaneous branch of the T10ŌĆōL1 levels can also be associated with flank pain. The lateral cutaneous branch from the dorsal ramus of the T7ŌĆōT12 levels conveys the sensation of the area from the subscapular to the iliac crest. The nerves of the T11ŌĆōL2 levels are a sensory fiber to the area under the iliac crest [7]. In this case, renal ischemia occurring from renal artery stenosis was initially thought to be the cause of the flank pain.
Above all, the medical causes related to the intraurinary condition must be diagnosed for proper treatment to take place. APCT is a reliable test to diagnosis these problems. Other musculoskeletal causes can be detected by computed tomography or magnetic resonance imaging. However, physical examination is more important as symptoms and radiological results are not always consistent.
Maigne [3] described the TLJ syndrome as a condition, typically, with pain on the iliac crest, and tenderness on palpation of the TLJ. As mentioned above, lateral branches of dorsal ramus at the T7ŌĆōL2 levels have cutaneous innervation after passing through the DPVM. These nerves can be functionally entrapped to the point of piercing the DPVM. Seong [8] mentioned that excessive tension and functional shortening of the DPVM can increase pressure of the vertebral foramen, which can result in excitation of the ventral and dorsal ramus of the spinal nerve. If the vasa nervorum of the spinal nerve is compressed, focal ischemia can be induced. Adenosine triphosphate (ATP) production can decrease, causing failure of the Na+/K+ ATPase pump and elevation of the extra-membrane K+ concentration. This may increase the resting membrane potential or reduce the threshold of nerve cells, leading to membrane hyperexcitability [9]. Hyperexcited nerve fiber can produce abnormal excitation signals and cause various types of pain. In this case, flank pain was the result of entrapment of the dorsal ramus of the spinal nerve at the T10ŌĆōT12 levels.
For diagnosis of TLJ syndrome, it is crucial to examine tender points by palpation of the DPVM in the thoracolumbar spine. Additionally, the skin and subcutaneous tissue of the flank and lower lumbar must be examined with the pinch-roll test. This test is accompanied by hyperalgesia at the involved dermatomes. Diagnosis of TLJ syndrome is confirmed by symptoms relieved after DPVM injection.
Conventional treatments of TLJ syndrome include manipulation targeted at restoring motion in the hypomobile segments and injection therapy at the involved segments [3]. A functional restoration program and several exercises, such as pelvic tilt exercises and hip bearing exercises, may also be considered [10].
In conclusion, TLJ syndrome is responsible in a considerable number of cases in patients with flank pain. In patients with flank pain whose internal organ problems have been dealt with, injecting saline or diluted lidocaine surrounding the painful DPVM and around the T12ŌĆōL1 segments can easily relieve flank pain. A physical examination such as the pinch-roll test for somatic sensory nerve entrapment is crucial for accurate diagnosis. Releasing entrapment of the involved spinal segments is a fundamental treatment and can be conducted with simple injection therapy.