INTRODUCTION
Parkinson disease (PD) is a complex, progressive, neurodegenerative disorder resulting in a wide range of deficits [1,2]. Speech and swallowing function are impaired, even in the early stages, significantly affecting health and the quality of life [3].
The cause of dysphagia in patients with PD is not clearly understood; however, a dysfunction involving the central pattern generator for swallowing in the brainstem and degeneration of the substantia nigra are possible causes that contribute to damaged non-dopaminergic neural networks [4,5]. Such damage leads to oral and pharyngeal phase dysfunction, which is characterized by abnormal bolus formation, repetitive tongue pumping, delayed swallowing reflex, decreased elevation of the hyolaryngeal complex, residues in both the vallecular and pyriform sinuses, and limited pharyngeal peristalsis [6].
Dysphagia not only affects the nutritional status of patients, but also their social interaction, susceptibility to fatigue, quality of life, and many other aspects. It may also lead to aspiration pneumonia, which is a major cause of death in patients with PD [1,4,7].
Conventional treatments such as bolus modification, postural and airway protective maneuvers, and pharmacological interventions, as well as other treatments such as expiratory muscle strength training, thermal-tactile stimulation, electrical stimulation, logopedic dysphagia treatment, and surgical intervention have been used to manage dysphagia in patients with PD. However, the long-term effects have yet to be verified, while a few studies have shown short-term benefits [4,8].
Since organs related to swallowing and speech are structurally and neurologically linked, speech therapy has been used to treat dysphagia without any evidence of sustained long-term benefits [4,9].
This study was conducted in patients with PD and Parkinsonian syndrome (PS) to identify the relationship between the maximum phonation time (MPT) and swallowing function, as well as the elements of swallowing, to provide a rationale for the use of voice therapy for the treatment of dysphagia.
MATERIALS AND METHODS
Subjects
Thirty patients diagnosed with PD or PS, who visited the clinic of the Department of Rehabilitation Medicine from January 2007 to December 2016 and underwent speech evaluation and videofluoroscopic swallowing study (VFSS), were included in this study. VFSS and speech evaluation were conducted simultaneously on eligible and selected patients. Patients with secondary Parkinsonism related to drugs, infection, or hydrocephalus were excluded. Patients with other neurological deficits and medical diseases, such as stroke or severe cardiopulmonary disease that may affect dysphagia were also excluded.
Of the 30 patients, 10 manifested PD and 20 had PS. The 20 patients with PS included 15 manifesting multiple system atrophy, 2 cases of dementia with Lewy body, and 1 with corticobasal degeneration. Of the 30 patients, the MPT was found normal in 9 and abnormal in 21. The baseline characteristics, including ambulatory and functional status and dysphagia scale scores, are listed in Table 1. This study was approved by the Institutional Review Board of Yonsei University Health System (No. 4-2014-0528).
Methods
Speech evaluation and VFSS were conducted to compare swallowing and speech. The speech evaluation was conducted by speech therapists in the form of one-on-one sessions in the treatment units. The MPT was measured with the pronunciation of /aa/ as the primary value. The MPT represent the maximum time (in seconds) for which an individual can sustain a vowel sound when uttered on one deep breath at a reasonably comfortable pitch and loudness. MPT is used to indirectly evaluate the laryngeal function and vocal cord vibration [10,11]. It was widely used since it is easier to access than the other parameters of evaluation. Compared with other acoustic parameters, MPT is relatively easy to evaluate regardless of the patient’s function or cognition. It can be used in older patients and patients with Parkinsonism. Furthermore, MPT is user-friendly since the patients or the caregivers can evaluate the changes themselves. In addition, its relationship with aspiration, which is the most important factor in dysphagia, was observed in previous studies [12].
MPT testing requires deep inhalation and a relaxed voice without stopping. The normal standard for MPT was based on the normal standards for age and sex as recommended by ‘Neurologic Speech-Language Disorders’ [13].
VFSS was performed by experienced physiatrists in a fluoroscopy/radiography room. The subjects sat laterally in a posture that was appropriate for observation of the anatomical structure and function. The subjects swallowed 5 mL and 15 mL of 12% semisolids followed by 5 mL and 15 mL of liquid, in the stated order, which were all mixed with barium sulfate solution. The test was recorded on video, which was evaluated by two physiatrists. The Penetration Aspiration Scale (PAS), National Institutes of Health-Swallowing Safety Scale (NIH-SSS), and Videofluoroscopic Dysphagia Scale (VDS) scores were evaluated.
Video fluoroscopic swallowing study analysis
National Institutes of Health-Swallowing Safety Scale
The NIH-SSS is a numerical scale that quantifies swallowing safety based on the observations derived from the VFSS, including food residue, laryngeal penetration, aspiration response, maximal esophageal entry, and multiple swallows. Higher scores indicate greater impairment [14].
Penetration aspiration scale
The PAS is a numerical scale that quantifies the degree of penetration and aspiration observed during VFSS. This 8-point scale is used to assess the depth of the passage of a bolus into the airway and the patient’s response. Higher scores indicate greater impairment [15].
Videofluoroscopic dysphagia scale
The VDS for oropharyngeal functional assessment during swallowing is based on the following 14 items: lip closure, bolus formation, mastication, apraxia, tongueto-palate contact, premature bolus loss, oral transit time, pharyngeal swallow triggering, vallecular residue, laryngeal elevation, pyriform sinus residue, coating of pharyngeal wall, pharyngeal transit time, and aspiration [16]. The scale has a maximum score of 100. Higher scores indicate poor swallowing function.
Statistical analysis
Data were imported into SPSS version 20.0 (IBM, Armonk, NY, USA) for analysis. Statistical analysis of VDS variables across subgroups was performed using an independent t-test. The differences in MPT between the subgroups, which were classified based on the VDS variables, were compared using the independent t-test. To determine the correlation between dysphagia scales and MPT, Pearson correlation coefficients were calculated; values above 0.6 were considered strong and those ranging between 0.4 and 0.6 were moderate. A p-value <0.05 was considered statistically significant.
RESULTS
Baseline demographic and clinical characteristics
VFSS and speech evaluation were performed in 30 patients (10 PD and 20 PS). The 30 patients included 16 males and 14 females. Sixteen patients were ambulatory (with or without device) and 14 were non-ambulatory. No statistically significant difference was observed in the Hoehn and Yahr (H&Y) stages, Modified Barthel Index, and Functional Independence Measures between patients diagnosed with PD and PS (Table 1).
Comparison of VDS variables among subgroups
The patients were divided into the following groups: PD or PS, independent or dependent ambulation, and normal or abnormal MPT. These groups were compared to determine differences in their VDS variables. The results showed significant differences in bolus formation (0.0±0.0 vs. 0.7±1.3; p=0.021) and laryngeal elevation (0.0±0.0 vs. 1.7±3.6; p=0.042) between normal and abnormal MPT groups (Table 2).
Comparison of mean MPT in the VDS subgroups
Among the 30 patients, 22 (73.3%) showed premature bolus loss. Eight (26.7%) had intact oral transit time. Six (20.0%) exhibited intact swallowing reflex. Nineteen (63.3%) had vallecular residue. Twenty-six (86.7%) showed complete laryngeal elevation. Seventeen (56.7%) carried pyriform sinus residue. Twenty (66.7%) exhibited pharyngeal wall coating. Twenty-seven (90.0%) had an intact pharyngeal transit time. Thirteen (43.3%) showed aspiration.
Comparison of these VDS subgroups revealed significant differences in MPT among those assigned to groups based on bolus formation (7.3±4.9 vs 3.3±2.0; p=0.009), oral transit time (9.5±5.4 vs. 5.6±4.2; p=0.047), pharyngeal swallow triggering (12.4±4.6 vs. 5.2±3.6; p<0.001), and laryngeal elevation (7.3±4.7 vs. 2.1±2.4; p=0.040) (Fig. 1).
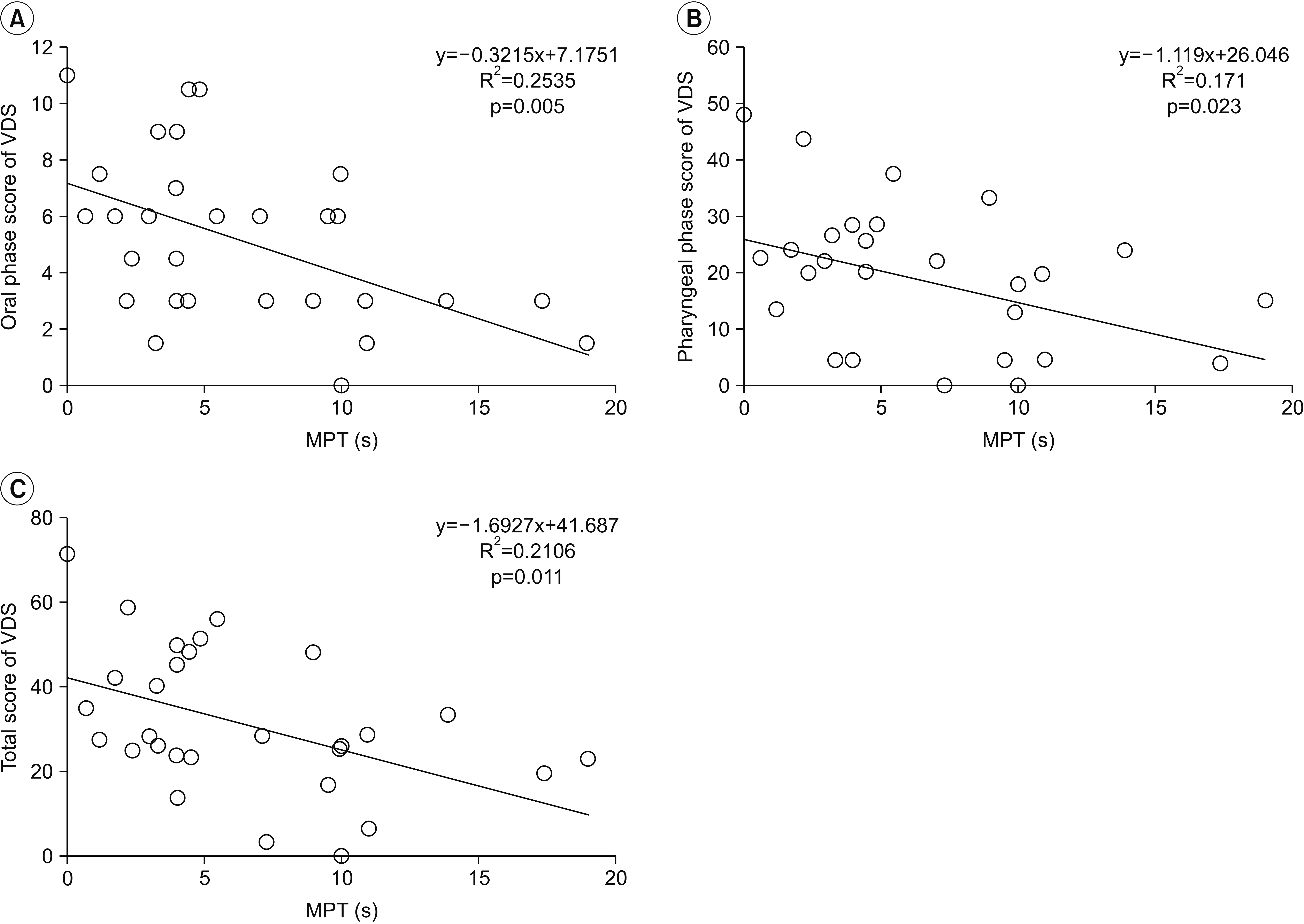
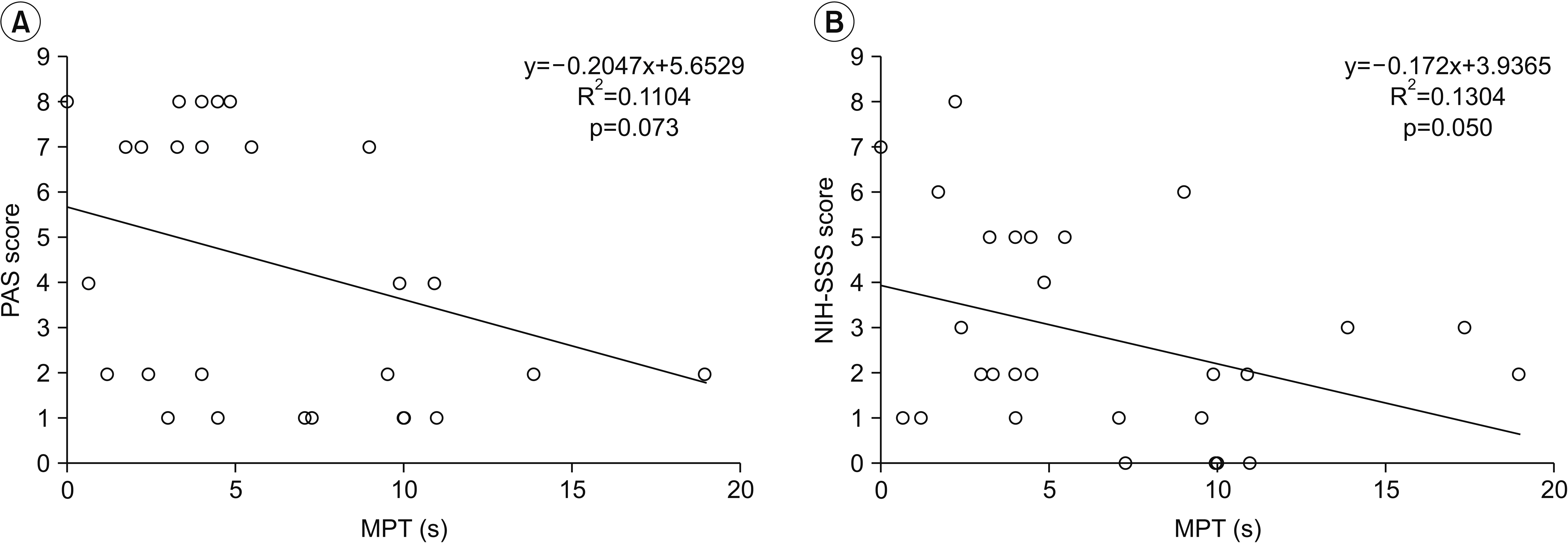
Correlation of MPT with VDS, PAS, NIH-SSS scores
A correlation analysis was conducted between the MPT and the dysphagia scales. Oral phase of VDS was defined as the sum of lip closure, bolus formation, mastication, apraxia, tongue-to-palate contact, premature bolus loss, and oral transit time. Pharyngeal phase of VDS was defined as the sum of pharyngeal swallowing triggering, vallecular residue, laryngeal elevation, pyriform sinus residue, coating of the pharyngeal wall, and pharyngeal transit time. The MPT was moderately correlated with total score of VDS (r=-0.459, p=0.011), oral phase score of VDS (r=-0.504, p=0.005), and pharyngeal phase score of VDS (r=-0.413, p=0.023) (Fig. 2). It also showed a weak correlation with the NIH-SSS (r=-0.361, p=0.050), but not the PAS (Fig. 3).
DISCUSSION
In this study, bolus formation and the laryngeal elevation functions were significantly higher in the normal MPT group compared with the impaired group. When the VDS variable subgroups were also compared, those with intact bolus formation, oral transit time, pharyngeal swallow triggering, and laryngeal elevation showed significantly longer MPTs compared with the impaired groups, indicating an interactive correlation between swallowing and phonation.
In addition, the MPT correlated with oropharyngeal motor function, such as tongue movement (bolus formation, oral transit time), laryngeal elevation, and pharyngeal swallow triggering. This function may be attributed to an increased bolus volume with appropriate tongue movement when swallowing, leading to increased stimulation of sensory receptors that trigger a pharyngeal swallowing reflex [6,17].
VDS and NIH-SSS correlated with MPT in patients with PD and PS, which provides additional evidence that oropharyngeal dysphagia correlates with phonatory dysfunction. There was no correlation between PAS and MPT, a weak correlation between NIH-SSS and MPT, and a moderate correlation between VDS and MPT. The PAS focuses on the presence of aspiration, whereas the NIH-SSS indicates remnant peristalsis, and other aspects of the pharyngeal phase. The VDS additionally indicates oral phase elements, showing comprehensive oropharyngeal dysfunction in patients suggesting that phonatory function is related to the quality of oropharyngeal swallowing function, but not directly to the aspiration itself.
Swallowing is an organized sensorimotor process within a complex neural network involving automatic and volitional systems [18]. In patients with PD, dopaminergic drugs had no significant effect on non-motor symptoms [4] and other dysphagia treatments have therefore been attempted. Lee Silverman Voice Treatment (LSVT) resulted in improved tongue movement during swallowing, and swallowing efficiency reduced oral residue and oral transit time [17]. Expiratory muscle strength training in patients with PD for 4 weeks also resulted in short-term improvement in PAS scores. The increase in duration and displacement of hyoid movement led to a wider and longer opening of the upper esophageal sphincter, improving the coordination of airway protection and bolus flow through the oropharynx [18,19]. In another study, a significant improvement in the laryngeal elevation time was reported after 8 weeks of group therapeutic singing, which presumably protected the airway from foreign material for a longer period [20].
These studies did not directly target swallowing. However, these types of training can recruit muscles that are involved in swallowing and stimulate similar central and peripheral neural control elements during training, and are therefore, considered to improve dysphagia [21]. Similarly, our study revealed several swallowing elements related to MPT. Since MPT is improved by training, voice therapy is a potential treatment for dysphagia. The aforementioned studies were typically conducted exclusively in patients with idiopathic PD and with relatively mild H&Y stages. However, patients with PS and those at relatively advanced H&Y stage were also included in this study suggesting that a wider range of patients than previously demonstrated stand to benefit from voice therapy. PS is generally less responsive or not responsive to dopaminergic drug therapies than PD. Therefore, alternative treatment methods are more important.
In previous studies, MPT was used to indirectly evaluate laryngeal function and vocal fold vibration efficiencies. Instead of solely targeting MPT for training, MPT was included as a part of voice therapy, similar to LSVT, or indirect training using an expiratory muscle strength training program [10,11,17]. Since this study indicates that an increase in MPT leads to an improvement of swallowing symptoms, training that is designed and conducted to target MPT will directly confirm the treatment effects.
In addition to MPT, diverse acoustic parameters such as intensity, jitter, shimmer, harmonics-to-noise ratio, voice onset time, sequential motion rate, and alternating motion rate can be measured to evaluate the voice. In this study, MPT was based on the subject’s characteristics, ease of evaluation and parameter representation. In future studies, the relationship between different parameters and swallowing function needs to be investigated in a large group.
Overall, there is a need for large-scale, well-designed, randomized, and controlled studies in order to correlate MPT with swallowing-related elements, as well as determine the short- and long-term effects of voice therapy on dysphagia, by comparing the results before and after treatment.