INTRODUCTION
Dysphagia is a common condition after brain injury. Previous reports using videofluoroscopic swallowing study (VFSS) estimated the dysphagia prevalence to be 35% to 67% in stroke patients. It is also estimated that 30% of traumatic brain injury (TBI) patients have a swallowing disorder [1,2,3]. Mukand et al. [4] found that 26% of their brain tumor patients had dysphagia. Dysphagia may cause aspiration pneumonia, under-nutrition, and/or a decreased quality of life [5]. Since there is an increase in the morbidity and mortality because of complications arising due to dysphagia, a proper feeding method is required in the affected patients. Approximately 13%ŌĆō15% of stroke patients show a persistent swallowing dysfunction after 6 months [6], and many cases of severe dysphagia remain dependent on tube feeding for longer periods [7].
The common methods of enteral tube feeding include nasogastric (NG) and gastrostomy tubes. NG tube feeding is the most common; the tube is easy to insert and has been used successfully for enteral nutrition. However, this feeding is associated with complications such as rhinitis, esophageal reflux, strictures, aspiration pneumonia, and esophagitis, and the risk of tube misplacement also indicates that NG tube is not an ideal long-term method of tube feeding [8]. The gastrostomy tube is ideally offered to patients requiring long term (longer than 4 weeks) tube feeding, but associated complications such as peristomal infection, peritonitis, inadvertent removal, and leakage [9].
Intermittent oro-esophageal (OE) tube feeding was introduced in 1988 by Campbell-Taylor et al. [10], to supply nutrition to patients with dysphagia. In the OE tube method, the feeding tube is intermittently inserted into the esophagus. Previous studies have reported that the OE tube improves swallowing functions and reduces the risk of pneumonia, reflux and aspiration [10,11,12]. In addition, studies indicate the OE tube to be a safer tube feeding method that can be applied over a longer period without severe complications [10,13,14]. However, since there are no clear optimal guidelines for the indication of OE tubes in dysphagic patients with a brain lesion, there are difficulties in selecting appropriate dysphagic brain lesion patients for OE tube treatment. The aim of this study was to evaluate the clinical factors associated with OE tube training success and identify possible clinical predictors.
MATERIALS AND METHODS
Subjects
Dysphagic patients hospitalized in the department of rehabilitation medicine and who had undergone OE tube training in the period between January 2005 and December 2014 were retrospectively identified. A total of 135 patients underwent swallowing therapy at our hospital using an OE tube. Patients with a brain lesion (stroke, brain tumor, and TBI) were included in our current analysis. We excluded patients who met any of the following criteria: (1) active medical problem such as respiratory infection, (2) no VFSS evaluation during admission or no VFSS-confirmed dysphagia, (3) verified abnormal findings in the esophageal phase of VFSS, (4) history of head and neck cancer or operation, or (5) inability to appropriately respond to verbal commands. From an initial cohort of 135 patients, 76 patients were finally recruited. All patients included in this study were assigned to either an OE tube success or failure group. The success group included patients where an OE tube was successfully and safely inserted at least 3 times, or who were capable of attempting OE tube feeding. The failure group contained patients in whom the OE tube could not be inserted for various reasons.
Data was collected from the medical records of our study cases, including age, sex, onset (duration between onset and OE tube training), cause of brain lesion, location of brain lesion, and history of pneumonia. We assessed the ability of these patients to follow commands, their Korean version of Mini-Mental Status Examination (K-MMSE) score for cognitive function, VFSS findings, reason for OE tube training failure, and any OE tube complications. This present study was approved by Asan Medical Center Institutional Review Board and local ethics committee (IRB No. S2014-2101-0002).
OE tube protocol
OE tubes were applied to patients who met the following criteria: (1) dysphagia with non-oral feeding or severely poor oral intake, (2) an alert consciousness, (3) no medical problems such as pneumonia, and (4) ability to adhere to OE tube procedure. An 8ŌĆō12 French Nelaton tube (effective tube length 360 mm, natural rubber latex catheter) was used for the OE tube treatment and feeding procedure. In the first OE tube treatment session, an occupational therapist inserted the tube. The Nelaton tip was first immersed in water to reduce friction. Insertion proceeded with the patient's chin facing down to prevent entry into the airway. The patient was asked to swallow the tube when the tube tip reached the lateral wall of the pharynx. The tube was then inserted carefully through the pharynx as far as possible without triggering the gag reflex. Tube insertion was stopped if there was a possibility of incorrect insertion, or if any of the following events occurred: (1) voice change, (2) coiling of the tube in the mouth, (3) coughing or signs of choking, or (4) a severe gag reflex.
To ensure correct tube placement, the end of the tube was put in a glass of water after insertion to check for bubbles due to the pressure of the cricopharyngeus or esophageal peristalsis, and siphoning due to the negative pressure of the pharynx. Five respiratory cycles were observed. We then injected 10 mL of air through the OE tube to check whether the patient coughed, and a further 2ŌĆō3 mL of water to check for any signs of aspiration. Patients and caregivers were both shown how to insert the OE tube. Once the patient was able to safely insert the tube, OE tube feeding commenced in the ward. All patients continued conventional swallowing therapy.
Data analysis
Clinical factors, neuroanatomical characteristics, and the gag reflex were compared between the OE tube success and failure groups, using the Mann-Whitney test and Fisher exact test. A multivariable logistic model was applied to identify independent clinical predictors of OE tube training success (odds ratios and 95% confidence interval [CI]). A p-value <0.05 was considered statistically significant. A receiver operating characteristic (ROC) curve was used to determine the optimal cutoff values of some predictive variables (the area under the curve [AUC] >0.5). All analyses were performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
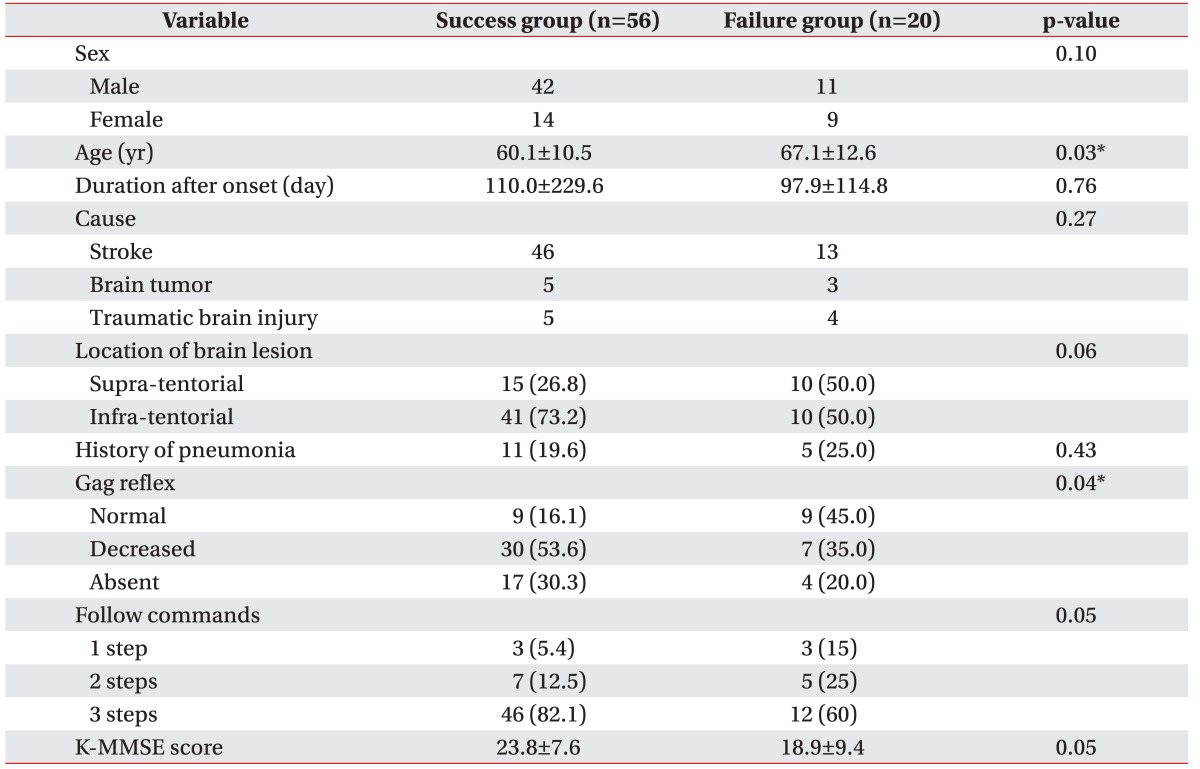
The clinical characteristics of the two study groups are presented in Table 1. There were significant differences between the groups in terms of age, gag reflex, ability to follow commands, and K-MMSE (p<0.05). The mean age of the success group was 60.1┬▒10.0 years, which was 7.0 years younger than that of the failure group (67.1┬▒12.6 years). Gag reflex was classified as normal, decreased, or absent. There were 16% normal gag reflex patients in the success group, but 45% in the failure group. There were no significant differences between the unilateral and bilateral gag reflex impaired patients. The mean K-MMSE scores of the success and failure groups were 23.8┬▒7.6 and 18.9┬▒9.4, respectively. The success group patients were able to follow more command steps than patients in the failure group. There were no significant differences in the cause of brain lesion. Infra-tentorial lesions were non-significantly associated with successful OE tube training compared with supra-tentorial lesions, but showed statistical trends of more OE tube success than supra-tentorial lesions.
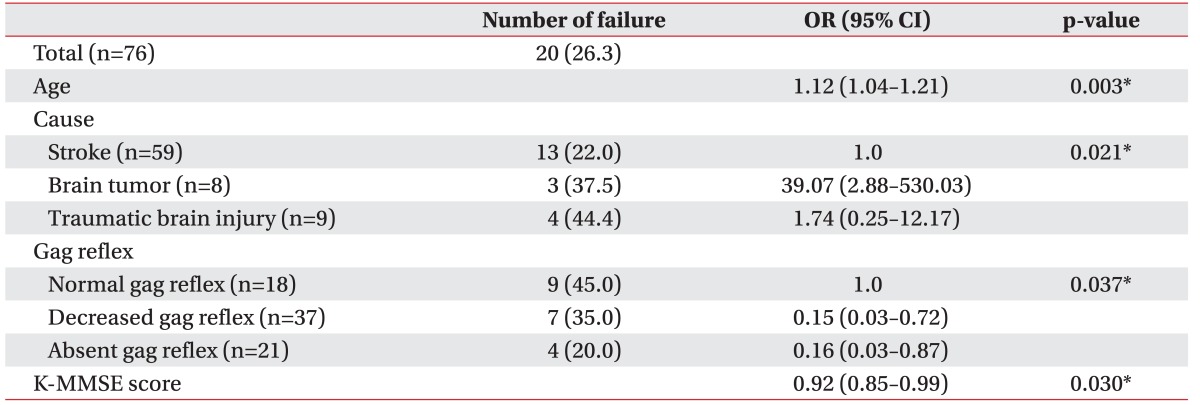
Multiple logistic regression analysis of the clinical features of the dysphagic patients revealed that age (p=0.003), cause of brain lesion (p=0.021), gag reflex (p=0.037) and K-MMSE (p=0.030) were independent predictors of successful OE tube training (Table 2). A younger age was also associated with OE tube training success. Patients with a brain tumor or TBI showed a higher failure rate than patients with stroke. Impaired gag reflex and a higher K-MMSE markedly increased the rate of OE tube insertion success.
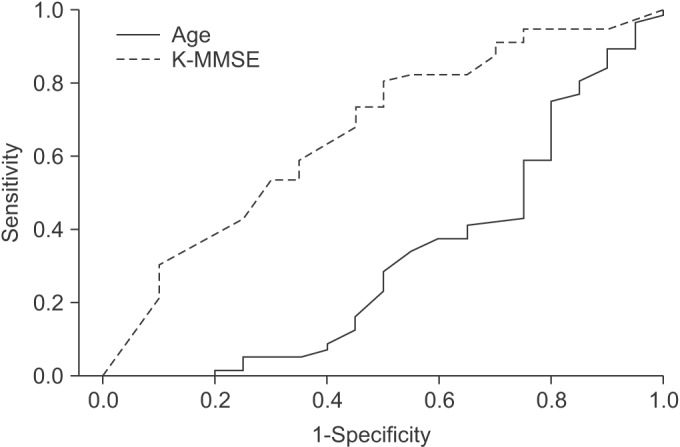
Given that age and the K-MMSE cutoff values predicted OE tube success, we assessed the ROC curve (Table 3, Fig. 1). We were unable to determine the cutoff value for age, since the AUC was less than 0.5. The AUC for K-MMSE was 0.67, with a standard error of 0.072 (95% CI, 0.526ŌĆō0.807; p=0.028). The K-MMSE cutoff score associated with successful OE tube training was 19.5.
The reasons for OE tube failure were gag reflex (42.1%), refusal or noncooperation (31.6%), and inability to swallow the tube (26.3%). Only one patient developed an OE tube associated complication, specifically a sore throat. However, this patient was in the success group and maintained feeding with the OE tube.
DISCUSSION
This study investigated the clinical factors predicting OE tube training success in dysphagic patients with a brain lesion. We found that age, stroke (cause of brain lesion), impaired gag reflex, and higher cognitive function are predictive of OE tube training success.
In our current study, the cause of brain injury was classified into stroke, brain tumor, and TBI. TBI patients had a higher rate of OE tube failure. In addition, since TBI patients showed the most impaired cognitive functions and lowest abnormal gag reflex percentage, the results of these patients were as expected. The OE tube failure rate of tumor patients was also very high. However, because the brain tumor patients were younger, had a near normal cognitive function and a high rate of abnormal gag reflex, this outcome was contrary to our expectations. Notably, there were only 3 tumor patients in the failure group, which probably limited the analysis. Thus, a larger sample size is required in future, to identify the OE tube success rate of tumor patients.
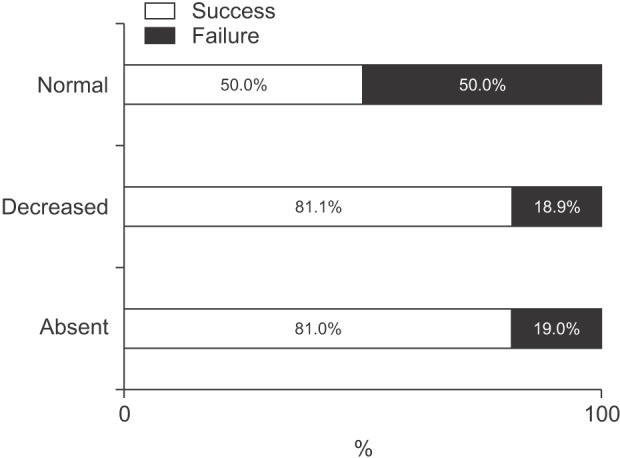
The gag reflex is a normal defense mechanism that prevents foreign bodies from entering the upper respiratory tract [15]. Because the OE tube is intermittently inserted through the oral cavity into the esophagus, this reflex can lead to OE tube feeding failure. In our present study, the most common reason for OE tube failure was indeed found to be the gag reflex. A greater number of our patients had a decreased or absent gag reflex in the success group than in the failure group (Fig. 2). Both, a bilaterally and unilaterally impaired gag reflex, are associated with a higher OE tube success rate compared with a normal gag reflex in our current series. This finding indicates that a unilaterally impaired gag reflex mechanism also satisfactorily enables the patient to withstand the intraoral stimuli caused by the OE tube. Although a gag reflex is often absent in healthy adults [16], an absent gag reflex is 10 times more frequent in dysphagic patients with an acute stroke, and is associated with a need for tube feeding [17]. It is reported to be an independent predictor of non-oral feeding in the subacute phase (at 6 weeks from onset) [18]. Brain lesion patients with an impaired gag reflex have a higher chance of requiring long term tube feeding. However, although the gastrostomy tube, and not the NG tube, is the ideal method for patients requiring long-term enteral feeding, the complications and invasiveness of the stomal site leads to resistance in some patients and their care givers. Moreover, a continuously inserted NG or gastrostomy tube constrains patients from returning to their daily routines and work. Thus, it is worthwhile to utilize OE tube feeding for dysphagic patients with an abnormal gag reflex.
Previous studies have reported that patients treated with the OE tube were required to understand this procedure, be cooperative, and show proper cognitive function [10,12,13,14,19]. In our present study series, a higher cognitive function was associated with higher OE tube training success. The reason for this association is that the training requires the perception, attention, memory, and executive functions of the patient, and also because a severely decreased cognitive function correlates with chewing and swallowing dysfunction [20,21]. However, no study to date has recommended that any specific level of cognitive function is required for successful OE tube training. Here, we have used the ROC curve analysis to determine an optimal K-MMSE cutoff score of 19.5.
There was no significant association with the location of brain lesion and tube feeding success in our current cohort. This is possibly due to a biased selection of supra-tentorial patients who would be more likely to successfully complete OE tube training than other supratentorial patients. The enrolled supra-tentorial patients in our current study were more likely to have a greater gag reflex impairment or higher cognitive function, which are better conditions for OE tube training. Another possible reason was an uneven proportion of infra-tentorial patients in our study population. This bias seems to have occurred due to the widespread belief that infra-tentorial patients might be more suitable for OE tube training. Indeed, our infra-tentorial group showed higher cognitive functions than the supra-tentorial group (K-MMSE: 25.6┬▒5.9 vs. 16.0┬▒9.0), and a higher abnormal gag reflex rate (abnormal gag reflex: 81.4% vs. 68.0%). These findings are in line with statistical trends for greater OE tube success in the infra-tentorial group (OE tube success rate: 80.4% vs. 60.0%). Based on these findings, we believe that statistically meaningful results would be obtained with a larger number of patients in a future investigation.
Since ours was a retrospective study, it had several noteworthy limitations. The first was that the K-MMSE scores were not assessed at the starting point of OE tube training. The K-MMSE was performed at admission or transfer, which was before the time the OE tube training starting point. Thus, the score obtained might not exactly reflect the cognitive function of patients at the OE tube training point. However, 20 of our study patients were in the chronic phase and stationary state. In the other 56 patients, the mean interval between the K-MMSE and the OE tube training start time was less than 1 week (6.75┬▒5.55 days). Therefore, it is likely that there was no significant difference in cognitive function between these 2 points. Second, although the gag reflex was routinely checked during OE tube treatment, it was not examined by a predetermined physician or occupational therapist. Third, the OE tube training process administered to each patient was not uniformly controlled.
Notwithstanding these aforementioned limitations, our current study is, to our knowledge, the first report to compare the clinical factors associated with OE tube training success, and to identify the clinical predictors of OE tube feeding success. A well-controlled prospective study is needed to confirm our findings.
In conclusion, the OE tube feeding method can be applied to brain lesion patients with dysphagia. Successful OE tube training is associated with a younger age, an impaired gag reflex and higher cognitive function (particularly, a K-MMSE score Ōēź19.5). These factors should therefore be considered in order to increase the probability of OE tube training success when considering OE tube feeding of dysphagic patients.