Intracranial Hemorrhage in the Corpus Callosum Presenting as Callosal Disconnection Syndrome: FDG-PET and Tractography: A Case Report
Article information
Abstract
We report the findings of 18F-fluorodeoxyglocese positron emission tomography (FDG-PET) and diffusion tensor tractography (DTT) in a right-handed patient presenting with callosal disconnection syndrome, including alien hand syndrome, after an anterior communicating artery aneurysmal rupture. The 49-year-old patient had right hemiparesis and unintended movement of the right hand during action of the left hand. A brain magnetic resonance imaging revealed lesions in the upper part of the genu and body in the corpus callosum as well as hemorrhage in the inter-hemispheric fissure. We observed extensive disruption of corpus callosum fibers in the upper genu and trunk by DTT for the evaluation of inter-hemispheric connection. FDG-PET revealed severe hypometabolism in the left cerebral hemisphere, including basal ganglia and thalamus, and hypermetabolism in the right cerebral hemisphere. Based on findings of FDG-PET and DTT, the callosal disconnection syndrome presented in the patient could be the result of loss of transcallosal inhibition in the contralateral hemisphere.
INTRODUCTION
Callosal fibers connecting both hemispheres allow communication of information as well as integrative and reciprocal inhibitory influences. Injury to corpus callosum may disturb an individual's emotions, motor control, and decision-making. Alien hand syndrome (AHS), first described in 1972, is one of the symptoms of callosal disconnection. The characteristic symptom of AHS is a purposeful action of one hand against the patient's intentions, while the ipsilateral hand could not make intended movements. Several cases of AHS due to deficits in the corpus callosum have been reported [1]. However, the mechanism of AHS after brain injury has not been fully elucidated.
Diffusion tensor tractography (DTT) derived from diffusion tensor imaging (DTI) is a method used to reveal structural connectivity and injury of white matter. Corpus callosum is composed of bundles of white matter for communication between the two hemispheres. Therefore, DTT is a useful tool to investigate structural injuries to the corpus callosum [2]. 18F-fluorodeoxyglocese positron emission tomography (FDG-PET) is used to examine the functional state of whole brain by measuring glucose metabolism. A change of metabolism detected by FDG-PET may reveal functional activity and pathological changes after brain injury [3,4]. Herein, we report the findings of DTT and FDG-PET in a patient who presented with callosal disconnection syndrome accompanied by AHS caused by an anterior communicating artery (A-com) aneurysm rupture.
CASE REPORT
A 49-year-old woman suffered from spontaneous subdural arachnoid and intracranial hemorrhages in the corpus callosum genu and body, resulting from a ruptured A-com aneurysm. One month later, after a coiling procedure of the A-com aneurysm, she was transferred to our rehabilitation department. Clinical symptoms of the patient included global aphasia, apraxia, and right hemiparesis. Features of AHS were observed in her right hand while she demonstrated improved motor strength and performance. Her right hand often reached forward and grasped objects within sight unintentionally. She experienced difficulty voluntarily releasing the grasp similar to a foreign limb in the subacute period. The coordination of the hands was insufficient to be able to do buttons on clothes. The right hand would hold the clothes against the patient's will, so the left hand had to free right hand's grip on clothes. After several weeks, the impulsive action disappeared. However, the inter-manual conflict and voluntary hand release problems still remained. Her functional state was severely impaired after one month from onset, at which time FDG-PET was conducted. Recorded performance measures were as follows: 3 for the Modified Barthel Index (MBI) score, 3 for the Berg Balance Scale (BBS), and 16 points for the National Institutes of Health Stroke Scale (NIHSS). One month after rehabilitation, the functional state of the patient showed much improvement, from 3 to 38 for MBI, 3 to 40 for BBS, and 16 to 6 points for NIHSS. Three months later, inter-manual conflict and voluntary hand release had improved enough to undo buttons.
T2-weighted MRI and DTI were acquired from the patient at four weeks after onset. The DTI was acquired using a sensitivity-encoding head coil on a 3T MR scanner (GE Healthcare, Milwaukee, WI, USA). A diffusion-weighted echo-planar imaging sequence was performed with the following parameters for each of the 26 noncollinear diffusion-sensitizing gradients: TR/TE/NEX=10000 ms/95.9 ms/2.0; slice thickness=4.0 mm; b=1000 s/mm2; matrix 128×128; FOV=250×250 mm. Fiber tracking was performed using DTI-Studio software (CMRM; John Hopkins Medical Institute, Baltimore, MD, USA) for reconstructing corpus callosum fibers by a fraction anisotropy <0.2 and angle change >60°. A region of interest was placed on the whole corpus callosum by a sagittal color map. Eddy current-induced image distortions were removed using affine multi-scale two-dimensional registration in the Oxford Centre for Functional Magnetic Resonance Imaging of the Brain (FMRIB) Software Library (FSL; www.fmrib.ox.ac.uk/fsl). FDG-PET/CT was performed to assess metabolic activity in the brain. PET scans were acquired starting at 50 minutes after intravenous injection of 0.2 mCi/kg 18F-FDG using an Advance PET scanner (GE Healthcare). Axial resolution of the scanner was 2.14 mm full width at half maximum. The PET images were reconstructed using a Hanning filter (cutoff frequency=10.9 mm) and displayed in a 128×128 matrix with a slice thickness of 4.0 mm. Spatial preprocessing and statistical analysis were performed using the Statistical Parametric Mapping (SPM) method to compare the patient to age-matched control subjects using an unpaired t-test. SPM generates an SPM statistic for the entire brain image which was then transformed to a normal distribution. Regions were considered significant at an uncorrected level of p<0.001.
DTT of the corpus callosum showed bilateral extensions to both hemispheres in normal subjects. However, the DTT of the patient revealed extensive disruptions at the upper portion of the genu and whole body area (Fig. 1). Compared to healthy control subjects (n=18; mean age, 49 years; range, 44-55 years; 8 men), we found abnormal results in the FDG-PET/CT showing reduced intensity in the left hemisphere, including the basal ganglia and thalamus but excluding the occipital lobe (Fig. 2). Moreover, metabolism in the right hemisphere was extensively increased. According to the findings of tractography and FDG-PET/CT, disconnection of both hemispheres at the corpus callosum led to metabolic changes in the brain and manifestation of AHS.

Sagittal T2-weighted brain magnetic resonance imaging (A) and axial images (B) showed hyperintensity in the corpus callosum genu and body as the result of anterior communicating artery aneurysm rupture. (C) Diffusion tensor tractography of the corpus callosum fibers shows extensive disruption.
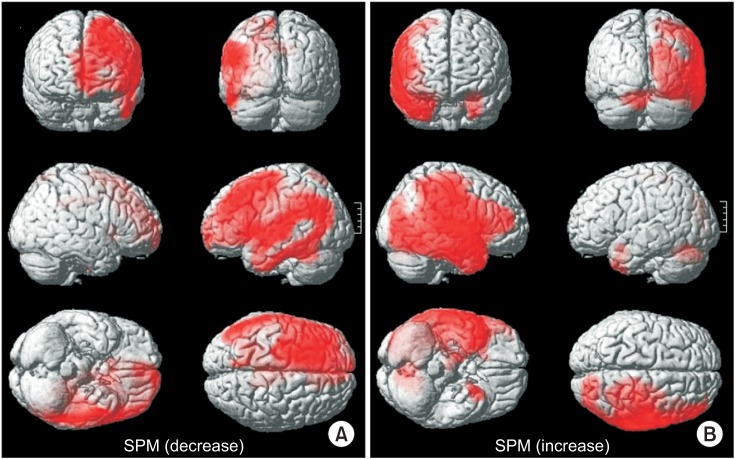
Three-dimensional rendering, showing the spatial distribution of significant metabolic changes by Statistical Parametric Mapping (SPM) (p<0.001). (A) 18F-fluorodeoxyglocese positron emission tomography (FDG-PET) scans reveal diffuse hypometabolism in the left hemisphere with the exception of the occipital lobe. (B) Metabolism of the right hemisphere is generally increased.
DISCUSSION
We report the findings of DTT and FDG-PET/CT for a patient with callosal disconnection syndrome with AHS due to a ruptured A-com aneurysm. MRI scans revealed subdural arachnoid and intracranial hemorrhages in the corpus callosum genu and body. Clinical symptoms included right hemiparesis, right somatosensory deficit, aphasia, gait disturbance with a wide base, apraxia, and AHS. DTT of the corpus callosum showed extensive disruption. FDG-PET/CT showed hypometabolism in the left hemisphere with the exception of the occipital lobe.
Appropriate movement requires coordination of the posterior parietal lobe and supplementary motor area, transcallosal inhibitory influence, and so on [5]. Injury to the corpus callosum could lead to dysfunction of the communication in these brain territories, resulting in various clinical symptoms associated with callosal disconnection syndrome. AHS, one of these symptoms, is a state of autonomy causing patient lose the ability to initiate intended movement. AHS has two types, frontal and callosal. Pure callosal AHS occurs with lesion restricted to the middle trunk of the corpus callosum. The primary symptom of callosal AHS is inter-manual conflict and difficulties in initiating desired actions. Frontal AHS is caused by lesions in the callosal and frontal cortex with distinguishable clinical symptoms, such as impulsive reaching and grasping behaviors of the contralesional hand. The patient in this study exhibited unwilling unintentional movement patterns and inter-manual conflict with difficulty in voluntary hand release during the subacute period. Subsequently, inter-manual conflict remained for three months after onset. Based on these symptoms, it can be concluded that the patient presented frontal and callosal AHS during the subacute period. Moreover, clinical symptoms of callosal AHS remained for three months.
For setting goals and establishing a treatment plan for stroke rehabilitation, it is very important to determine the location and extent of brain injury. Although MRI is a very sensitive and accurate method for the detection of brain injuries, it is sometimes difficult to determine the degree of injury due to various factors, such as perilesional edema, volume effect of the stroke, and penumbra lesion. DTT is a reconstruction of tracts of diffusion tensor images according to fraction anisotropy in white matter tracts. The corpus callosum is composed of bundles of white matter [6,7]. There have been two cases showing correlation between clinical symptoms and disruption of corpus callosum fibers passing through the corpus callosum body using DTT [8]. Our case also presented severe disruption of fibers in the body of corpus callosum.
The patient presented with hypometabolism in the left hemisphere with the exception of the occipital lobe. This was detected by FDG-PET/CT conducted one month after onset. FDG-PET/CT revealed that hemorrhage of the corpus callosum produced degradation and hypometabolism of the left hemisphere in the left frontal and parietal lobes. This injury produced right hemiparesis, aphasia, and apraxia of right upper extremities. Remote metabolic effects in PET/CT allowed for the identification of functional and structural neural connectivity. Each portion of the corpus callosum connects the cerebral cortex between the two halves of the brain, allowing communication of information, as well as reciprocal inhibitory influence in both sides of the brain. Therefore, we hypothesized that the loss of transcallosal inhibition influenced by injury to the corpus callosum as well as the mass effect of the hemorrhage was responsible for the hypometabolism of the left hemisphere, which subsequently led to symptom of AHS in the right hand and difficulty in bimanual activities.
The right hemisphere, including frontal, parietal, and temporal lobes, presented hypermetabolism in FDG-PET/CT when compared to normal control subjects. To the best of our knowledge, this study is the first report concerning contralateral cerebral hypermetabolism of static PET/CT in a stroke patient. Since the brain cannot store energy substrates, the majority of glucose in the brain is consumed for signaling. Hypermetabolism of the resting brain on the 18F-FDG/PET indicated that cell activity and energy demand of the right hemisphere continuously increased, even at a resting state. Although the mechanism of increased metabolism has not been fully elucidated, we presume that recovery mechanisms (caused by severe injury of left hemisphere) and interruption of transcallosal inhibition (caused by the corpus callosum hemorrhage) lead to hypermetabolism in the right hemisphere. Rehme et al. [9] reported that fMRI findings in stroke patients with great corticospinal tract damage and more marked motor impairments showed enhanced contralesional motor cortex activity as a result of reduced inhibition of the contralesional hemisphere. Furthermore, some stroke patients use the ipsilateral motor pathway as a recovery mechanism. Repetitive transcranial magnetic stimulation (TMS) at the contralesional dorsal premotor cortex and primary motor cortex resulted in deterioration of motor performance for some stroke patients. Many other studies reported a relationship between functional recovery and the ipsilateral motor pathway of the affected extremities using fMRI, TMS, and DTI [10]. However, little studies concerning hypermetabolism of resting PET/CT after stroke have been conducted. Therefore, this case report has a limitation in discussing hypermetabolism in PET/CT.
In conclusion, we suggest that callosal disconnection syndrome is the result of the loss of transcallosal inhibition and metabolic changes in both hemispheres based on findings of FDG-PET and DTT. Although studies on hypermetabolism in PET/CT is not sufficient, this case showed the possibility that metabolic changes using FDG PET/CT could give useful information to evaluate brain injury and recovery mechanism after stroke. Further study using FDG-PET in stroke patients is needed to elucidate brain injury and recovery mechanisms.
Notes
No potential conflict of interest relevant to this article was reported.