INTRODUCTION
Stroke is one of the main causes of disability, with serious economic and social consequences [1].
In stroke patients, balance and proprioceptive impairment are important causes of functional limitations [2], and they are present in 48.1% [3] and 34%–64% [4] respectively.
Sherrington’s definition of proprioception encompasses the perception of joint positioning and bodily motion within space [5]. This description underlines the contemporary interpretation of the concept. Proprioception involves coordinated responses from various mechanoreceptors, including proprioceptors found in tendons, muscles, ligaments, and joint capsules [6]. These proprioceptors, such as the Golgi tendon organ, muscle spindle, and Pacini corpuscle, relay joint position and motion information to the central nervous system (CNS) [7]. The CNS processes this sensory information, integrates it with other inputs, and sends responsive commands to target tissues. Proprioceptive feedback is crucial for regulating body movement, protecting against joint overstretching and controlling posture and balance, allowing awareness of joint and body movements [8,9]. A decline in proprioception can change the joint biomechanics and the neuromuscular control of the limbs, resulting in impaired balance and a higher possibility of falls [7,10].
A negative significant correlation is suggested between the severity of proprioception impairment and both motor and functional abilities [11], and risk of falling [12]. Likewise, an impaired reactive balance (the ability to execute appropriate and effective reactions to keeping balance despite perturbations) makes hard walking and producing functional movements, resulting in a loss of autonomy in everyday life [13], and an increase of risk of falling [14].
The multiple sensory impairments, i.e. tactile sensations disorder, present in 7%–53%, and loss of stereognosis, present in 31%–89% of patients [4], contribute also to a high prevalence of falls [2,14].
Finally, daily activities in human life require the concomitant completion of motor tasks and cognitive functions, particularly difficult for stroke people [15], making them frail and disabled [16]. Furthermore, the difficulties in dual task activities increase the risk of falling among stroke subjects [17].
As well as the proprioceptive and reactive balance impairment, the severity of somatosensory impairments, and the degree of mobility-interference during dual task activities can help to predict the risk of falling and guide the therapeutic strategies to maximize long-term participation, minimize disability and reduce the risk of falls [12,18,19]. To obtain these goals, the rehabilitation must focus not only on autonomy, but also on balance, and task performance, and on falls prevention [20,21].
The aim of the study is to show the effectiveness of goal-oriented proprioceptive training in subacute stroke for the recovery of balance, autonomy in activities of daily living (ADLs), and for the prevention of falling. Secondary aims are to compare the effectiveness of goal-oriented proprioceptive training with dual task training or single task exercises. Lastly, sharing the rehabilitation program could guide physicians and therapists in their clinical practise, because, until now, recommendations about specific exercises in subacute stroke are not standardized.
METHODS
All procedures performed in this study involving human participants were in accordance with the 2013 Helsinki declaration and its later amendments or comparable ethical standards. The article was a retrospective study, so the approval of the ethical committee was not necessarily required. Informed consent was obtained from all participants included in the study.
Participant selection and characteristics in rehabilitation
The data of 35 subacute stroke patients, hospitalized in an intensive rehabilitation facility from September 2021 to March 2022, were retrospectively collected (Table 1). They were homogeneous in terms of type of stroke having experienced ischemic events between 3 to 11 weeks prior to the study. Their average age was 75.31±8.65 years. In terms of severity, their symptoms ranged from mild to moderate, manifesting primarily as spastic hemiparesis, weakness, balance issues, disability in daily activities. The distribution of the patients’ specific brain lesions was as follows: 22 patients had lesions in the territory of the middle cerebral artery 6 in the posterior limb of the internal capsule (2 underwent single task proprioceptive training, 4 dual task proprioceptive training), and 7 exhibited lacunar strokes in the capsular region (4 underwent single task proprioceptive training, 3 dual task proprioceptive training). At the onset of the study, both groups demonstrated homogeneity across all submitted scales, and this homogeneity extended to the subgroups stratified based on the location of stroke (Table 1).
Importantly, they exhibited no cognitive impairments, with normal vigilance, cooperation, orientation, memory, attention, decision-making, and general cognitive processing capabilities (ability to understand, process, and respond to information effectively), as a dedicated psychologist reported. No patients necessitated psychological support during their hospitalization. Moreover, there were no visual deficits, ensuring intact depth perception, reading abilities, facial recognition, and effective navigation of their surroundings without any visual field cuts or double vision. The participants were consistent also in terms of similar prior health conditions, being sufficiently autonomous in ADLs before the acute event. Furthermore, they were awake, alert, and cooperative at admission. Dual task group had 3 patients each using wheelchairs, walkers, and canes, with 8 requiring no aids. The single task group had varied distributions with 2 using wheelchairs, 2 with walkers, 5 with canes, and 9 without aids.
During the study period, the focus was on capturing a representative sample of patients undergoing rehabilitation post-stroke. It was noteworthy to clarify that the inclusion of only infarction stroke patients was not due to an intentional exclusion criterion set against haemorrhagic stroke cases. Rather, the patient demographics available for inclusion during the study timeline naturally led to this composition.
A total of 2 patients were excluded for incomplete data present in their medical record, instable clinical conditions during the hospitalization, and comorbidities that interfered with the intensive rehabilitative program.
Clinical evaluation tests and assessment tools
To gain a comprehensive understanding of the participants’ health and functional capabilities, several clinically validated assessment scales were employed. The clinical assessments included the following scales: Numerical Rating Scale (NRS) for pain [22], Barthel Index to assess the functional autonomy [23], Tinetti test [24] and Berg Balance Scale (BBS) for balance [25], Timed Up and Go Test (TUG) in single and dual tasks for the risk of falling [26]. The cognitive dual tasks, executed during TUG, included counting backward while walking; the motor dual task included carrying a half full glass while walking.
NRS was utilized to evaluate the subjective experience of pain among participants. Patients were asked to rate their pain on a scale from 0 (no pain) to 10 (worst possible pain). Barthel Index measured performance in ADLs, and assessed participants’ functional autonomy, covering aspects from mobility to self-care. Tinetti Test gauged both balance and gait capabilities. By examining participants as they performed specific physical tasks, the test provided insights into their stability and coordination. These scales were administered at admission and at discharge, after a mean of 59.82±2.72 days of hospitalization in rehabilitation facility.
The evaluations were consistently conducted by the same physician who was a specialist in Physical Medicine and Rehabilitation, with over 3 years of experience specifically working with stroke patients, with a focus on balance disorders and postural instability. This consistency in the evaluator ensured uniformity and reliability in the assessment process throughout the study.
Proprioceptive training: procedure and dual task implementation
The rehabilitation consisted of 3 hours a day of goal-oriented proprioceptive training for 7 days a week, organized in two sessions of 1.5 hours a day. All participants performed a consistent traditional rehabilitation program. The distinction between the two groups was based on different proprioceptive training approaches. The single task group underwent proprioceptive exercises, while the dual task group integrated both motor and cognitive exercises in their training regimen. The specific exercises for each group are detailed in Table 2.
Within these sessions, specific exercises were performed at varying intensities, tailored to the individual needs and progression of each patient. The intensity was regularly adjusted based on patient feedback, performance, and therapist observation to ensure both safety and challenge.
The difficulty of tasks was progressively increased. For instance, patients initially started with simpler tasks, like walking while naming fruits. As their proficiency improved, they would progress to tasks that demanded more cognitive load, such as walking while performing serial subtractions. Continuous feedback was provided to the participants about their performance. If a participant struggled, the complexity was adjusted to ensure safety while still providing adequate challenge.
For the integration into daily activities, as participants became more comfortable, the dual tasks were integrated into more complex ADLs, like navigating a crowded area while carrying a conversation or holding objects.
Thanks to the homogeneity of the sample, this implementation remained consistent across all participants, ensuring uniformity in the training experience for every individual.
In the motor dual task, participants simultaneously engaged in two motor activities. Examples included walking while holding a tray laden with cups of water or dribbling a ball while walking. Conversely, the cognitive task combined motor and cognitive elements. While participants performed a motor activity, such as walking, they also undertook a cognitive challenge. This could involve counting backwards, verbally solving arithmetic problems, or naming items from a specific category, all while continuing their motor task. The primary aim was to assess the participant’s ability to coordinate and execute two distinct motor functions simultaneously, reflecting many real-world scenarios where multitasking is required.
Statistical analysis and methodology
The R statistical software (igraph package) was used for data analysis. Quantitative data were expressed as mean and standard deviation and were compared using t-test. The paired t-test was used to assess outcomes within each group before and after training. The unpaired t-test was utilized for comparing the two groups at baseline (T0) to evaluate sample homogeneity. At the follow-up assessment (T1), the unpaired t-test was applied to analyze the comparative effectiveness of the two different treatments.
The correlation between the scales was estimated using the Pearson and Spearman’s coefficient. For Spearman correlation, the data of mobility aids were ranked in 1 indicating their unnecessary use, 2 for the use of canes, 3 for walkers, and 4 for wheelchairs. p<0.05 was considered with statistical significance.
RESULTS
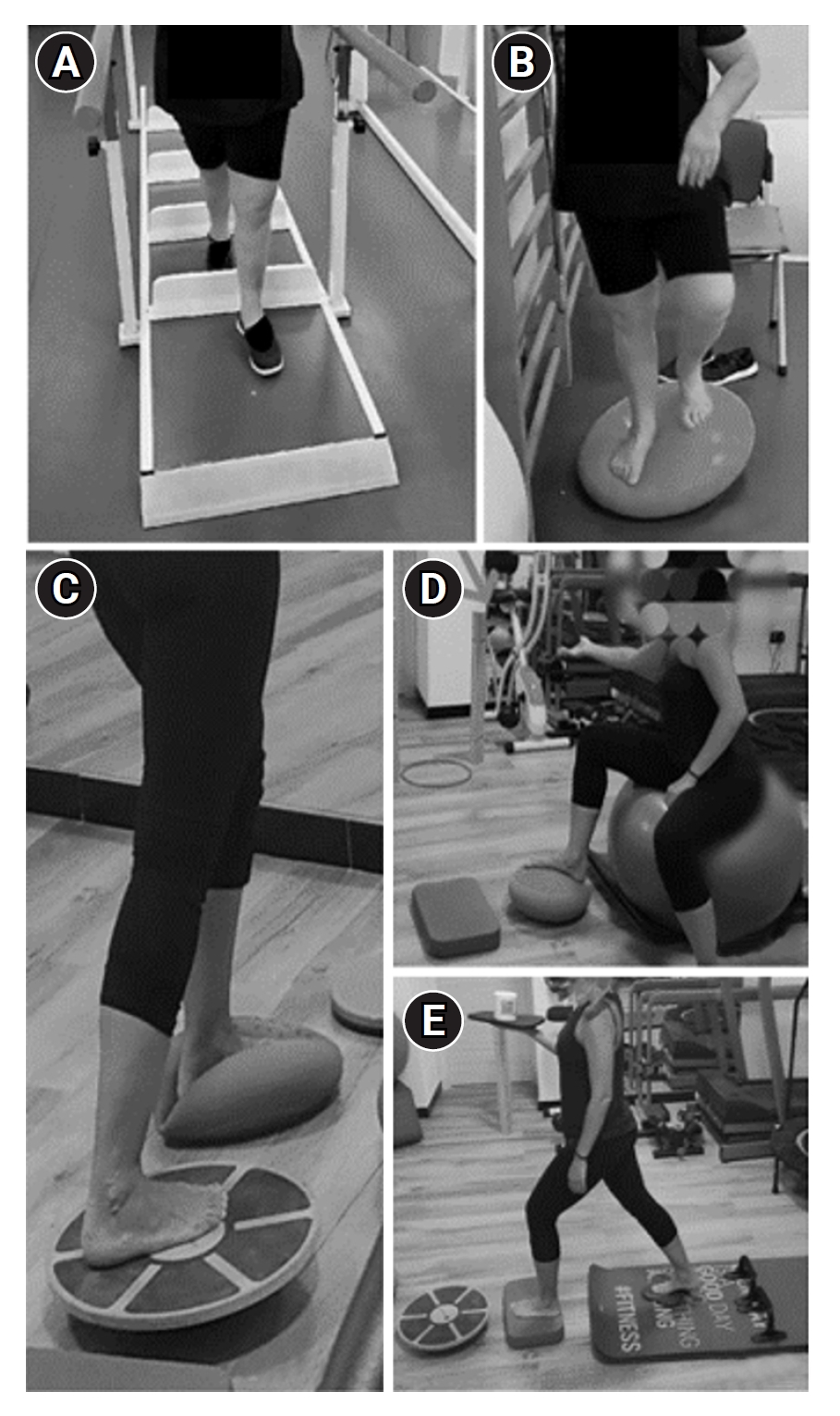
During a mean of 59.82±2.72 days hospitalization in a rehabilitation facility, 35 subacute stroke patients conducted (1) a traditional rehabilitation program with (a) postural and core exercises, (b) mobility training, (c) occupational therapy, and (2) a goal-oriented proprioceptive training that consisted in proprioceptive and reactive balance training (Fig. 1). A total of 18 out of 35 patients performed a goal-oriented single task proprioceptive rehabilitation, while 17 patients performed dual task training with goal-oriented motor and cognitive exercises (Table 2).
There were no statistically significant differences between the two groups at the initial assessment (T0) across all the scales used.
At discharge, statistically significant differences were recorded in both groups for (1) Barthel Index (p<0.0001), with the recovery of the autonomy in ADLs; (2) Tinetti test (total score p<0.0001, balance assessment p<0.0001 in dual task group, p=0.0029 in single task group, gait assessment p=0.0023 in dual task group, p=0.0093 in single task group); (3) BBS (p<0.0001), with an improvement of balance; (4) TUG with dual task exercises (p=0.0052 in dual task group, p=0.0020 in single task group); and (5) TUG with single task exercises only for dual task group (p=0.0035) with a reduction of the risk of falling (Table 1). Comparing the two groups, balance, as assessed with Tinetti balance assessment, showed a significant difference in dual task proprioceptive training group than single task group (p=0.052). Thus, the study showed that goal-oriented both single and dual task proprioceptive rehabilitation significantly improved autonomy (Barthel Index in single and dual task groups p<0.0001), balance (BBS in single p=0.0001 and dual task groups p<0.0001; Tinetti balance test in single p=0.0029 and dual task groups p<0.0001), and gait (Tinetti gait test in single p=0.0093 and dual task groups p<0.0023; Tinetti total score in single and dual task groups p<0.0001) and reduced the risk of falling (TUG during dual task conditions in single task group p=0.0020 and dual task groups p=0.0052).
Considering the three subgroups, the first, related to strokes in the territory of the middle cerebral artery, the most numerically significant, showed similar results in terms of significance after both single and dual-task proprioceptive training and in the comparison between single and dual task training. Indeed, an improvement in Barthel Index (after single and dual task training p<0.0001), BBS (after single p=0.0172, dual task training p=0.0013), Tinetti balance test (after single and p=0.0340, dual task training p=0.0108), Tinetti gait test (after single and p=0.0340, dual task training p=0.0108), TUG during single task activities (dual task training p=0.0453), TUG during dual task activities (after single p=0.0262, dual task training p=0.0263) were recorded.
The other subgroups, with locations in the posterior limb of the internal capsule and lacunar strokes, differed from the results of the first subgroup. Indeed, the second subgroup showed no significant results in the scales related to balance, gait and risk of falls after either single or dual task training (p>0.05). The only noteworthy improvement observed was in autonomy (after single task training p=0.0219, dual task training p=0.0270).
The third group showed no results after single task training (p>0.05), but improvements in balance after dual task training, assessed by BBS (p=0.0261) and Tinetti balance (p=0.0481).
The comparison between single and dual task training revealed a significant improvement in BBS and Tinetti balance in the first two groups and in TUG in single task in the third subgroup. Particularly, in patients with stroke affecting the territory of the cerebral middle cerebral artery, there was a significant enhancement of autonomy (Barthel Index p<0.0001), and balance (BBS=0.0056, Tinetti balance test p=0.0908) after dual task training compared with single task training. After stroke in the internal capsule, dual task training resulted in an improved BBS (p=0.048) and Tinetti balance scale (p=0.0245) compared to single task training. In lacunar strokes of the capsular region, dual task training led to a significant improvement in TUG during single task activity (p=0.0154).
Given that subgroups with fewer patients exhibited only partial results, consolidating them into a single group could enhance the overall statistical robustness and consistency of the findings.
After rehabilitation, in dual task proprioceptive training group, the values of TUG in single and in dual task were associated and changed correspondingly (r=0.9867, p<0.0001). Moreover, a significant relationship was present between the total score of Tinetti test and (1) BBS (r=0.8382, p<0.0001), (2) TUG in single task (r=-0.5343, p=0.0271), (3) TUG in dual task (r=-0.5455, p=0.0235). Likewise, Tinetti gait test was significantly related to (1) BBS (r=0.7640, p=0.0004), (2) TUG in dual task (r=-0.4885, p=0.0466). Furthermore, Tinetti balance test was significantly related to (1) Barthel Index (r=-0.5033, p=0.0394), (2) BBS (r=0.8443, p<0.0001), (3) TUG in single task (r=-0.5510, p=0.0219), (4) TUG in dual task (r=-0.5594, p=0.0196). Conversely, no correlation was recorded between Barthel Index and (1) Tinetti gait test (r= -0.2629, p=0.3081), (2) total score of Tinetti test (r=-0.3927, p=0.1189), (3) BBS (r=-0.3631, p=0.1520), (4) TUG in single task (r=0.3934, p=0.1182), and (5) TUG in dual task (r=0.3563, p=0.1603). Likewise, no significant relationship was showed between BBS and (1) TUG in single task (r=-0.3762, p=0.1367), (2) TUG in dual task (r=-0.4012, p=0.1105), and (3) total score of Tinetti (r=-0.4758, p=0.0536). Thus, after rehabilitation, the improvement of balance was related to the reduction of the risk of falling, (showed by the positive relationship between Tinetti test and TUG in single task and in dual tasks), but only partially to the recovery of autonomy (positive relationship between Barthel Index and Tinetti balance test, but no significant between Barthel and BBS; Table 3).
A significant relationship was found between the use of mobility aids and (1) BBS (r=-0.625, p=0.0074), (2) Tinetti gait test (r=-0.602, p=0.0105), and (3) total score of Tinetti test (r=-0.574, p=0.0160). Conversely, no significant relationship was found between the use of aids and (1) Barthel Index (r=-0.0374, p=0.8865), (2) Tinetti balance test (r=-0.453, p=0.0682), (3) TUG in single task (r=0.375, p=0.1385), and (4) TUG in dual task (r=0.400, p=0.1113). Therefore, these data highlighted a positive correlation between the use of aids and the recovery of balance (positive relationship of aids with BBS and total score of Tinetti test). Nevertheless, the use of aids did not improve autonomy (no significant relationship between aids and Barthel Index), nor reduce the risk of falling (no significant relationship between aids and TUG in single task and dual task; Table 3).
DISCUSSION
The novelty of this study lies in its integrative approach to post-stroke rehabilitation. Instead of relying on just one type of therapeutic intervention, we incorporate three distinct types of rehabilitation: (1) goal-oriented training, (2) proprioceptive training, and (3) dual task training. By weaving these three methodologies together, our objective is to foster a more comprehensive and synergistic rehabilitative experience. We suggest that the union of these specific training types has the potential to yield superior outcomes, capitalizing on the strengths of each individual method. The confluence of goal setting, enhancing body spatial awareness, and promoting multitasking abilities forms the foundation of our holistic rehabilitation strategy, setting the stage for optimized patient recovery.
Proprioceptive training is a specialized rehabilitative approach that underscores the body’s ability to discern its position in space, an essential component for ensuring coordinated and smooth movements [8]. In addressing such deficits, goal-oriented training gets patients to concentrate on specific movement or position-based objectives, by making them focus on achieving specific action or position-based goals. It seems to increase the intensity of practice in stroke rehabilitation [27].
This specificity can aid in rejuvenating neural pathways connected to proprioception, despite there is no solid evidence about the underlying long-term neuroplastic changes associated proprioceptive training [28]. Moreover, in single-task exercises, patients are primarily engaged in one specific activity at a time. On the other hand, dual task proprioceptive training requires patients to multitask, effectively managing two activities simultaneously. This simultaneous engagement in dual task training inherently exerts a greater cognitive and motor demand as compared to single task exercises. While the single task approach can be pivotal during the initial phases of rehabilitation, dual task training, with its augmented cognitive load, mirrors the multifaceted demands often encountered in real-world situations [29].
According to the results of the study, in subacute stroke patients, the goal-oriented proprioceptive training, both with single and dual task exercises, improved balance and autonomy in ADLs, and reduced the risk of falling, during dual task activities too. Thus, the pivotal element to reach these results is the goal-oriented proprioceptive training. Whether applied through single or dual-task exercises, the distinction between them appears superimposable. Furthermore, the comparison between the scales at discharge showed what rehabilitation goals were achieved. In particular, after goal-oriented dual task proprioceptive training, the positive relationship between Tinetti test and TUG was related to a reduced risk of falling secondary to an improvement of balance. Nevertheless, the lack of correlation of Barthel Index with BBS and with Tinetti test (gait assessment tool and total score of Tinetti test) could explain why the recovery of balance only partially was related to autonomy (positive relationship between Barthel Index and Tinetti balance test), despite the reduction of the risk of falling. Lastly, the use of mobility aids resulted closely related to the recovery of balance (positive relationship between the aids and the score of BBS and Tinetti gait test and total score), but it did not improve autonomy (no significant relationship between aids and Barthel Index), nor reduced the risk of falling (no significant relationship between aids and TUG in single task and dual task). This demonstrated that the use of aids was not sufficient to make mobility and gait safe and to acquire autonomy, but only helped to improve balance. Indeed, mobility aids can enhance proprioceptive feedback and provide stability, aiding in balance recovery. However, autonomy involves more than just balance; it encompasses daily functional activities, which might not be directly improved by the mere presence of an aid. Furthermore, while aids help in improving balance, patients might become overly dependent on them, potentially limiting their autonomy in daily tasks without the aid.
Among the foremost objectives of rehabilitation for stroke patients there are enhancing activity levels, reducing fatigue, and minimizing the risk of falls [30]. The choice of the rehabilitation program, with goal-oriented therapy, proprioceptive exercises, and dual task training was based upon the goals to be achieved, the recovery of autonomy, balance and the reduce of the risk of falling.
The contribution of this research is mainly represented by its comprehensive approach to post-stroke rehabilitation. While much of the existing literature tends to focus on proprioceptive, dual-task, or goal-oriented training separately, this study melds all three therapeutic interventions, goal-oriented rehabilitation, proprioceptive training, and dual-task exercises.
Actually, literature agrees that proprioceptive training has positive effects on balance performance, gait speed, trunk control, and basic functional mobility among people with stroke [31,32]. Furthermore, current literature has shown a growing interest in the effects of dual-activity training across various conditions, including older adults [33], dementia [34], Parkinson’s disease [35], and multiple sclerosis [36], with stroke being a prominent focus. Indeed, in stroke patients, despite the high heterogeneity of proposed exercises, all integrated cognitive and motor tasks with proprioceptive exercises proved effective, independently from the rehabilitation session’s organization and timing [37,38,39]. In particular, dual task training shows an improvement in step length, cadence [18], balance, and a reduction of the risk of falling [40].
Furthermore, a task specific training, with an “oriented” dual task exercise, with a specific purpose and functional activity, is deemed to have positive effects on proprioceptive, balance, gait speed and spasticity in stroke survivors [41,42]. Several studies highlighted the significance of incorporating goal-oriented and motivational components into rehabilitation. A study utilized aquatic games [43], and another introduced tango lessons [44]. Such innovative approaches not only enhanced the patients’ enjoyment of their rehabilitation program but also fostered greater treatment adherence and improved final outcomes. Moreover, combining specific task-oriented training with manual therapy appeared to improve balance and mobility in patients after stroke [45]. Furthermore, exergaming [39] and virtual reality-based dual task training [46] not only aids in walking and balance control [39,46], but also has discernible cognitive benefits in stroke survivors [39].
According to the results of the study, the integration of the following rehabilitation techniques (goal-oriented therapy, proprioceptive exercises, and dual task training) with traditional treatment (postural and core exercises, and gait training) allowed patients to recover independence and balance, and reduce the risk of falls, which is very important also for families and caregivers.
Limitations
Despite the limitations related to the retrospective methods of data collection and the small number of patients, we considered valuable to present our experience because of the absence of guidelines and consensus on this topic. While our study offered significant insights into the functional outcomes of goal-oriented proprioceptive training, especially in the context of balance and mobility, it did not include direct assessments of proprioception, such as joint position sense or specific proprioceptive tests, nor a comprehensive evaluation of muscle strength, nor a detailed evaluation of upper extremity function.
The retrospective nature of the research and the absence of standardized psychological scales were notable constraints. Indeed, patients were included based on the psychologist’s qualitative evaluation, considering factors such as vigilance, cooperation, orientation in time and space, ability in maintaining their memory, attention, decision-making, and general cognitive processing capabilities (ability to understand, process, and respond to information effectively), as well as willingness and adherence to the rehabilitation program. Even if this approach lacked specific objective evaluation indicators, it allowed to include patients with favourable psychological attributes to active participation in rehabilitation.
This retrospective study did not include a direct assessment of muscle strength using dynamometers. The level of strength could be indirectly inferred based on the aids used by patients at admission and discharge.
Conclusions
This study uniquely combines three key post-stroke rehabilitation strategies: goal-oriented, proprioceptive, and dual task training, offering a comprehensive therapeutic approach.
In the subacute phase of stroke, the goal-oriented proprioceptive training, both with single and dual task exercises, improved balance, abilities in ADLs, and reduced the risk of falls. Comparing the two rehabilitative strategies, dual task training demonstrated a significant improvement of balance, as assessed by Tinetti balance assessment, compared to single task exercises. Certainly, the consequent improvement of balance reduced the risk of falling, but only partially improved autonomy. Moreover, after goal-oriented dual task proprioceptive training, the use of mobility aids was strictly connected to the recovery of balance, supported by significant relationships with BBS and the Tinetti test’s total score, particularly the gait component. However, these aids did not show a corresponding improvement in autonomy, as evidenced by the lack of a significant relationship with the Barthel Index. Additionally, mobility aids did not significantly reduce the risk of falls, with no significant associations found in both single-task and dual-task versions of the TUG. Moreover, the use of mobility aids did not show a significant reduction in fall risk, as evidenced by the absence of significative associations in TUG performed both in single-task and dual-task and TUG.
However, more research is needed about this topic, to compare different rehabilitation strategies and find the best protocol to reduce the disability related to stroke.