INTRODUCTION
Children with traumatic brain injury (TBI) typically experience major developmental disruptions and long-term functional impairments [1]. TBI has more severe and persistent effects in children than adults, presumably due to the immaturity of the child’s brain and the potential for early injury, which interferes with ongoing brain development and disrupts related cognitive functions [2,3]. A recent review reported that 50% of children showed some form of cognitive impairment following TBI [4]. Cognitive function deteriorates after TBI, particularly attention, memory, processing speed, and executive function [5]. Studies of the prevalence of motor impairment in children with TBI are particularly limited, as prior studies focused on the rate of motor recovery based on functional rather than impairment measures. However, the majority of children with TBI have disrupted balance performance and walking ability that limit their activities [6,7]. Moreover, they are more prone to gait instability and repeated head injury in the presence of both motor impairments and cognitive deficits [8]. Cognitive and motor function are significantly linearly correlated in individuals with TBI [9]. Most children with TBI present spatiotemporal deviations in gait, including decreased gait velocity, decreased step length, a broad-based gait, and increased double-limb support time compared to typically developing (TD) children [6,7]. The potential consequences of gait impairments in children with TBI include increased disability and increased risk of falls [8]. These limitations can cause TBI children to become more dependent on their caregivers and reduce their community and social participation, reducing their quality of life [10-12]. Thus, recovery toward independent and safe walking is crucial for children with TBI to ensure that they can be independent at home and in the community.
Walking is a fundamental function of mobility in daily life that requires various forms of concurrent motor and cognitive tasks. Performing a dual-task while walking requires some degree of attention and complex processes that involve the ongoing integration of visual, proprioceptive, and vestibular sensory information [13]. The ability to divide one’s attention and process information is also essential in the simultaneous execution of two or more tasks [14]. As attention is a common impairment among children with TBI [15], the demands for attention for tasks may be overwhelming and reduce their performance of one or all tasks [16]. Hence, children with TBI require more attention to walk and are more affected by concurrent tasks.
A previous study of ambulatory children with TBI found that a concurrent cognitive task deteriorated their gait since it imposed high demands on attention [17]. The authors concluded that increasing the complexity level of the task resulted in significant attention-related gait changes and that the existing attention deficit can cause severely disturbed walking ability in children with TBI. Katz-Leurer et al. [17] observed the gait performance of children with TBI who were challenged with concurrent cognitive tasks without concurrent motor tasks. Another recent study showed that cognitive and motor tasks deteriorated gait performance in children with TBI relative to TD children during the Timed Up and Go test [18]. However, the author emphasized that the concurrent motor activity in that study required less effort and was not difficult for those children with TBI who had no motor impairments of the upper limbs and recommended increasing the difficulty of the task in future studies to challenge gait performance. Since walking involves concurrent motor and cognitive tasks in everyday life, it is necessary to evaluate its impact on these children to provide useful knowledge and important outcomes for clinicians who treat children with TBI.
Therefore, the present study aimed to investigate gait performance under concurrent tasks in children with TBI versus TD controls by increasing the complexity level of concurrent motor tasks. The second objective was to compare these two types of concurrent tasks (cognitive vs. motor) on gait performance between groups. Finally, the third objective was to examine the correlations between gait parameters and attention and balance in children with TBI. We hypothesized that the concurrent motor and cognitive task conditions would cause significant gait deterioration compared to the single task condition in children with TBI and that concurrent cognitive tasks would result in greater gait deterioration than concurrent motor tasks in children with TBI.
MATERIALS AND METHODS
Participants
This case-control study included 16 children with TBI (13 boys and 3 girls) and 22 TD children (18 boys and 4 girls). Based on a previous study by Katz-Leurer et al. [17], an estimated 30-participant sample would provide 80% power with a type 1 error risk of 0.05. Children with TBI were recruited using purposive sampling from a government-funded hospital, while TD children were recruited from a local school and then matched by age, sex, body weight, and height to the TBI participants.
The inclusion criteria were as follows: (1) at least 6 months post-TBI, (2) Glasgow Coma Scale (GCS) score ≤12 at first admission, (3) age 8–14 years old, (4) ability to walk independently without walking assistance (foot orthoses permitted), (5) ability to obey one-step instructions, (6) ability to carry a tray, (7) full GCS score at the time of enrollment, and (8) provided consent to participate. Participants were excluded if they (1) had received botulinum toxin, (2) had undergone orthopedic surgery in the previous 6 months, (3) had visual field defects, or a (4) had a T-score >75 for disruptive behavior as measured by the Conners Clinical Index. Conners Clinical Index is commonly used in pediatric clinical and research settings to measure behavioral function [19]. It is intended to provide a concise overview of the problems and conditions of children and teenagers, primarily to assess children with attention deficit/hyperactivity disorder [19]. The study was approved by the Research Ethics Committee, Universiti Teknologi MARA (REC/86/15), and written informed consent was obtained from all participants and their guardians (or legal counsel).
Testing procedure
After written consent was provided, the participants’ demographic data were recorded. Their cognitive function and functional balance were measured using the Children’s Color Trail Test (CCTT) and Pediatric Balance Scale (PBS), respectively. The CCTT is an instrument used for neuropsychological assessments that provides information about visual attention, scanning, processing speed, and mental flexibility and performance [20,21]. The test consists of two sections, CCTT-1 and CCTT-2. The direct score of each section is represented by the time of task completion [20]. In the CCTT-1, the participants connect numbers in circles with alternate colors (yellow and pink) consecutively, while in the CCTT-2, the participants connect numbers in circles with alternate colors consecutively, as the same numbers exist in different colors [22]. The study revealed that the CCTT has a moderate test-retest reliability coefficient range (rtt=0.46–0.68) and moderate to high interference reliability coefficient range (rtt=0.75–0.78) among children with attention deficit hyperactivity disorder [23].
The PBS consists of 14 items assessing balance during different activities. On a 5-point scale (0 to 4), each item in the PBS is rated with a maximum total score of 56 (higher scores imply better balance) [24]. The study reported excellent test-retest (intraclass correlation coefficient [ICC]=0.998) and inter-rater reliability (ICC=0.998) when applied to school-aged children with mild to moderate motor impairments [24].
The APDM Mobility Lab (APDM Inc., Portland, OR, USA) is a system used to measure postural sway, postural transitions, and trunk and upper and lower limb movements using inertial sensors connected to particular parts of the body [25]. This system provides gait and balance information. In this study, to record spatial-temporal gait parameters, three motion sensors called “Opal” consisting of a 3-axis accelerometer, gyroscope, and magnetometer (APDM Mobility Lab) were used. The system was portable and user-friendly; therefore, it could be easily set up in a more natural environment than a laboratory. Each Opal was attached to each participant: one on each ankle and one on the lower back. The test using the instrumented long walk consists of walking in a straight line for a distance of 7 m. The primary outcomes obtained from the APDM Mobility Lab system were gait velocity, stride time, stride length, cadence, and double support time to complete the gait task.
The children were asked to walk at their normal pace in a straight line for each task and prioritize the secondary tasks during the concurrent task to magnify their impacts on gait performance. Start and stop signs were positioned on the floor to provide visual feedback to the participants. A trained evaluator provided standardized verbal instructions about the test protocol along with a visual demonstration of the walking test before the test was conducted. To familiarize themselves with the test, the participants performed three practice trials for each task. The task sequence was randomly determined, and the participants were given 3 minutes to rest between tasks. During the test, the participants wore their usual footwear (and orthotics, if applicable).
The concurrent motor and cognitive tasks were adapted from a previous study by Cherng et al. [26]. Since a recent study [18] studied subjects’ performance of a simple concurrent task consisting of carrying an empty tray and counting forward while walking and suggested an increase in the degree of difficulty, we chose the task involving a higher level of difficulty in which the subject carries a tray with seven marbles and counts backward. The test consisted of three different conditions in the following order.
(1) During the single task condition, the participants walked in a straight line for 7 m only (without a secondary task). The participants stood on the start sign comfortably and the experimenter gave the following instruction: “When I say ‘go,’ please walk toward the stop sign at your normal speed.” This procedure was repeated three times.
(2) For the concurrent motor task condition, the participants stood on the start sign comfortably while holding a tray with seven marbles on it (the tray was 17 cm in diameter and 1.2 cm deep, while the marbles were each 2 cm in diameter). When the experimenter said go, the participants walked 7 m toward the stop sign at their normal speed. The participants were required to prioritize the secondary task (carrying the tray) while walking. This procedure was repeated three times. Trials were considered failed and then repeated when the participants dropped one or more marbles from the tray.
(3) For the concurrent cognitive task, the participants had to walk in a straight line for 7 m while repeating a sequence of numbers backward. The task was adapted from the Wechsler Intelligence Scale for Children’s digit span task. The series of numbers to be replicated was set at the capacity of each child, which was individually decided prior to the experiment by following the Wechsler Intelligence Scale for Children section’s administration protocol. The participants stood on the start sign comfortably and the experimenter verbally gave them a series of numbers when the participant was ready to start walking. When they heard “go,” they walked 7 m toward the stop sign at their normal speed. The participants were required to prioritize the secondary task (counting backwards) while walking. This procedure was repeated three times. Trials were considered failed and then repeated when the participants committed errors in the counting backwards task.
Statistical analysis
The primary outcomes obtained from the APDM Mobility Lab system were gait velocity, stride time, stride length, cadence, and double support time to complete the gait task. We averaged three trials for each condition. All statistical analyses were performed using SPSS Statistics for Windows version 23.0 (IBM, Armonk, NY, USA). Descriptive statistics and normality of the distribution of variables were determined using skewness and kurtosis tests for all outcome variables. The independent t-test was used to compare the demographic data of the two groups of children. Repeated-measures analysis of variance (ANOVA) was performed to analyze the gait parameters across three different conditions (single, concurrent motor, and concurrent cognitive task) and two groups (TBI and TD children). A post-hoc Bonferroni comparison was conducted when the repeated-measures ANOVA test showed a significant difference (p<0.05). Finally, the correlations between the gait parameters and attention and balance performance in children with TBI were evaluated using Spearman correlation coefficient, where 0–0.30, was perceived as a weak correlation, 0.30–0.70 as a moderate correlation, and >0.70 as a strong correlation.
RESULTS
Gait velocity
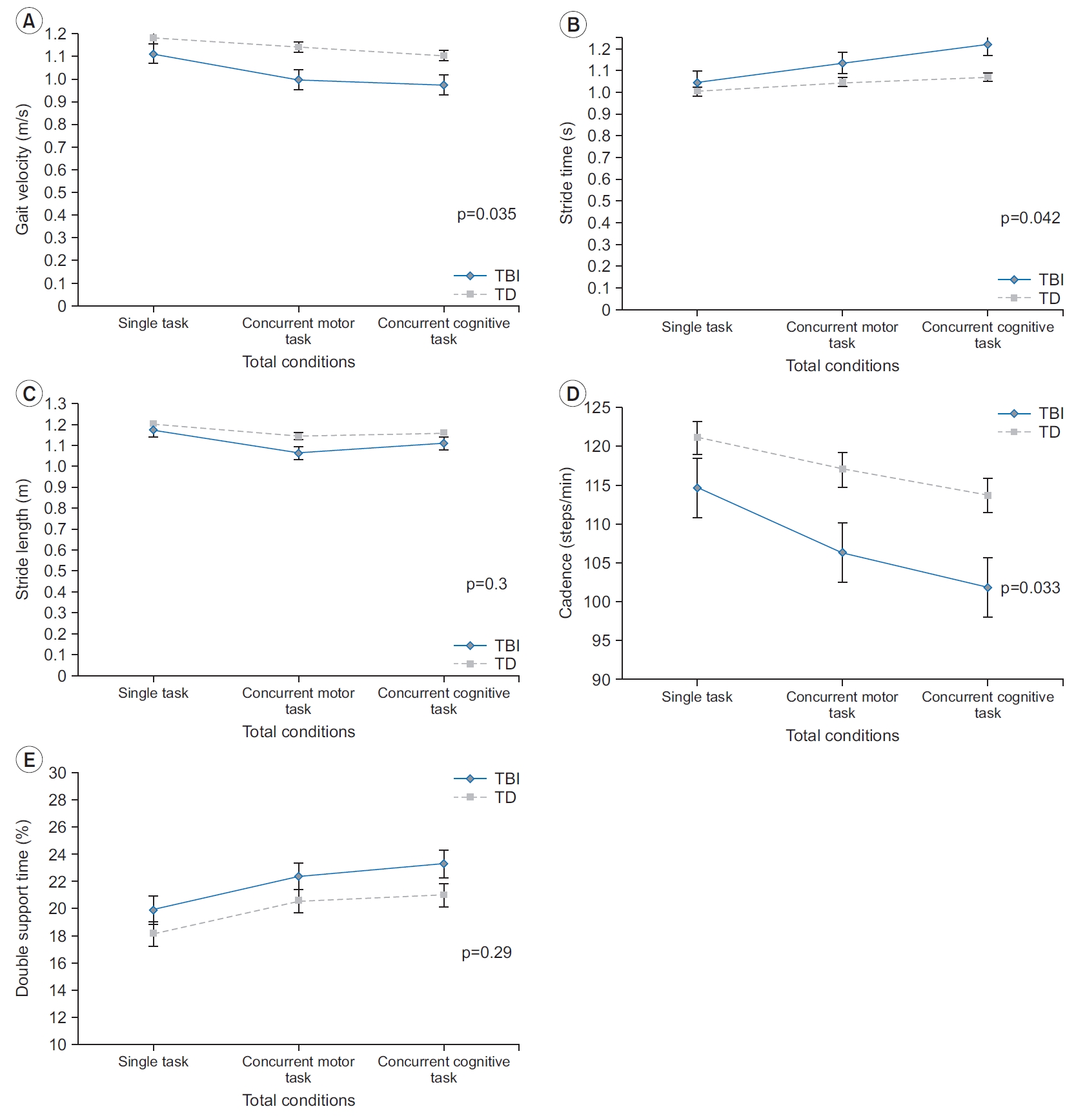
The gait velocity of the children with TBI was significantly slower than that of the TD children (group effect, p=0.035) (Fig. 1A). More importantly, concurrent tasks (motor and cognitive) had a differential effect on gait velocity for both groups (condition×group interaction; p=0.012). Table 2 shows a reduction in gait velocity for both groups in the concurrent task but was more significant in children with TBI. The post-hoc analysis (Table 3) revealed that, for children with TBI, the concurrent motor and cognitive task condition led to a slower gait velocity than the single task condition (p=0.005, p<0.001). Similar to children with TBI, both the concurrent motor and concurrent cognitive task conditions for TD children led to slower gait velocity than the single task condition (p=0.001, p<0.001). Although the gait velocity for both groups seemed slowest during the concurrent cognitive task out of the three conditions, it did not differ significantly between the concurrent cognitive task and the concurrent motor task in either group (p=1.000 in TBI, p=0.063 in TD).
Stride time
The reduction in gait velocity may have resulted from the longer stride time, shorter stride length, or both. To determine which gait parameters (spatial or temporal) deteriorated the gait velocity, the stride time and stride length were analyzed. As presented in Table 2, stride time was longer in children with TBI than in TD children (group effect, p=0.042). The stride time was also influenced by the concurrent task, which was confirmed by the significant condition effect (p<0.001). The concurrent task had a similar effect in both groups as confirmed by the non-significant interaction (p=0.051). The posthoc comparisons (Table 3) indicated that the concurrent cognitive task led to a significantly longer stride time than the single task condition (p<0.001) and the concurrent motor task condition (p=0.002). The concurrent motor task increased the stride time slightly compared to the single task, but the difference was non-significant (p=0.03).
Stride length
The stride length did not differ significantly between children with TBI and TD children (group effect, p=0.3) (Fig. 1C). In addition, a significant condition by group interaction (p=0.041) was noted for the stride length parameters despite the reduction trend for each task being similar between groups. Overall, stride length decreased during the concurrent tasks in both groups, but more so in children with TBI. The post-hoc test (Table 3) revealed that the concurrent motor and cognitive task conditions in children with TBI led to a shorter stride length compared to the single task condition (p=0.001, p=0.005), whereas the difference between the concurrent motor and the concurrent cognitive task conditions was nonsignificant (p=0.08). Both concurrent tasks (motor and cognitive) resulted in a significantly shorter stride length than the single task for TD children (p<0.001 for both comparisons). While the concurrent motor task led to a shorter stride length relative to the concurrent cognitive task, the difference was non-significant (p=0.539).
Cadence
The results of cadence during straight walking indicated that children with TBI took fewer steps per minute than TD children (p=0.033). Additionally, the concurrent tasks had a differential effect on cadence as indicated by the significant interaction (p=0.031). The post-hoc analysis (Table 3) revealed that both concurrent tasks resulted in a reduction in cadence compared to the single task in children with TBI (p=0.001 in concurrent motor, p<0.001 in concurrent cognitive). Although the cadence measured during the concurrent cognitive task was lower than that during the concurrent motor task, the difference was non-significant (p=0.086). As for TD children, performing the concurrent motor and cognitive tasks while walking in a straight line caused a decrease in cadence compared to the single task (p=0.001 in concurrent motor, p<0.001 in concurrent cognitive) in TD children. The concurrent cognitive task slightly decreased cadence compared to the concurrent motor task, but the difference was nonsignificant (p=0.058).
Double support time
The double support time during straight walking did not differ between children with TBI and TD children (p=0.29). The concurrent task conditions significantly increased the double support time (condition effect, p<0.001). Moreover, the condition by group interaction was not significant (p=0.29). The post-hoc comparison (Table 3) revealed that the concurrent motor and concurrent cognitive task conditions resulted in significantly higher double support times compared to the single task condition (p<0.001 for both). Although the concurrent cognitive task resulted in a higher double support time than the concurrent motor task, the difference was not significant (p=0.14) for either group.
Correlation between spatiotemporal gait parameters and CCTT-2 and PBS scores in children with TBI
The correlation coefficients between the spatiotemporal gait parameters and the CCTT-2 and PBS scores in children with TBI are shown in Table 4. In children with TBI, the gait velocity for the concurrent motor and cognitive tasks was significantly correlated with the CCTT-2 and PBS scores. For stride length, only the concurrent motor task was significantly correlated with CCTT-2 score. In contrast, all three different task conditions for the stride length parameters were significantly correlated with the PBS score.
DISCUSSION
Deterioration of gait performance while walking in children with TBI was reported previously [7,27-30]. However, there is scant information on the effects of concurrent motor and cognitive tasks on gait performance in children with TBI. The present study investigated the effects of concurrent motor and cognitive tasks on gait performance in children with TBI versus TD controls. The researchers discovered several important findings. First, concurrent tasks (motor and cognitive) adversely affect gait performance in children with TBI and TD controls. Second, children with TBI demonstrated reduced gait velocity, longer step time, and decreased cadence when combined with concurrent tasks relative to the performance of TD children. Third, the concurrent tasks (motor or cognitive), did not have any differential effects on walking performance, other than stride time parameters. Both groups took a longer stride time to perform concurrent cognitive tasks than the concurrent motor task, and this difference was significantly more prominent in children with TBI than in the TD control group. Finally, there was a moderate correlation between gait parameters, specifically gait velocity and stride length, and CCTT-2 and PBS scores.
These study findings demonstrated that children with TBI and TD experienced concomitant changes in gait parameters, including reduced gait velocity, increased stride time, and decreased cadence. Both concurrent motor and cognitive task conditions resulted in the deterioration of gait parameters in both groups relative to the single task condition, but significantly more so in children with TBI. This result suggests that concurrent task conditions were challenging for children with TBI because they have balance and cognitive impairments (PBS: TBI vs. TD, 52.13±5.76 vs. 55.50±0.67 seconds; CCTT-2: TBI vs. TD, 99.50±68.96 vs. 59.64±0.36 seconds). The current findings are in line with those of previous studies that consistently showed deterioration in gait performance in children during walking while performing concurrent tasks [17,18,26,31-33]. They noted that the complexity level of the concurrent task determines the effect on walking performance. Since children with TBI have attention deficits, splitting their attention between two tasks may more greatly interfere with their gait performance than that of the control group [15]. Specifically, they must prioritize their attention to the secondary task and do not have gait as an automatic skill, which may explain the decrease in their gait performance.
In addition, our findings showed that gait deterioration was significantly observed for both groups during the concurrent motor and cognitive tasks compared to the single task, and the concurrent task type (motor or cognitive) did not have differential effects on walking performance. This may be due to the need for more attentional resources than for the single task. This increased deterioration in children with TBI can be explained by the balance deficiency and attention deficit posed in this population as seen in the PBS and CCTT-2 results. This is supported by the correlation analysis, which showed a moderate relationship between spatiotemporal gait parameters, particularly gait velocity and stride length, and PBS and CCTT-2 scores in children with TBI. The combination of balance deficit and attention problems in children with TBI may have made the concurrent tasks (motor and cognitive) more complex, requiring them to move and regulate more body segments while performing tasks at the same time. This requires greater attention compared to a single task. However, a recent study of ambulatory children with TBI showed that concurrent cognitive tasks caused greater deterioration in gait performance than concurrent motor tasks [18]. They concluded that holding an empty tray as a concurrent motor task is less challenging for children with TBI and intact upper-extremity function. Thus, it explained the present study’s finding as the concurrent motor task’s complexity has increased, which required the participant to carry the tray with seven marbles while walking. In contrast, previous studies involving TD children showed that concurrent motor tasks caused a greater reduction in their gait performance than concurrent cognitive tasks [26,32-34]. Furthermore, a study investigating children with developmental coordination disorder (DCD) demonstrated similar findings with TD children in which a concurrent motor task led to greater deterioration in walking under the dual-task condition [31]. These results may be explained by the existence of motor impairments among children with DCD and the lack of a cognitive deficit in TD children, which makes the concurrent motor task more difficult than the concurrent cognitive task.
The results demonstrated a reduction in gait velocity under the concurrent task condition in both groups. Changes in the temporal gait parameters, including stride time and cadence, appear to contribute to the gait velocity reduction. These results indicate that temporal gait parameters may be more vulnerable than spatial gait parameters to concurrent task interference. Clinically, the increase in double support time in children with TBI and balance impairment reflects balance control during gait [7]. Therefore, the increase in stride time led to a decrease in the gait velocity and cadence under the concurrent task condition, reflecting the greater challenge preserving dynamic stability during walking and performing more difficult tasks as a compensatory strategy that would be reflected in the double support time [35].
This study has several limitations. First, the researchers used only one form and one difficulty level of the motor and cognitive tasks. In future studies, when examining the gait of children with TBI in dual-task settings, researchers should use various types and different levels of difficulty of concurrent tasks to assess motor and cognitive capacity. Second, the researchers examined gait only when participants were walking in a straight line. Future studies should investigate the gait characteristics of turning during walking. And finally, the evaluator who performed the APDM Mobility Lab assessments was not blinded to the group allotments. Blindness should be addressed in future studies to avoid potential bias in the findings.
The current study’s findings demonstrated that children with TBI are more vulnerable to dual-task interference during walking than are TD controls. In addition, the concurrent tasks had substantial influence on the temporal gait versus spatial parameters. These findings suggest the importance of dual-task training in the gait training of children with TBI.