INTRODUCTION
Dysphagia is a common complication that may cause malnutrition and aspiration pneumonia in patients with brain injury [1]. Aspiration pneumonia is the major cause of death, especially in patients with chronic brain lesion. Aspiration occurs as a result of swallowing dysfunction, gastroesophageal reflux, or inability to adequately protect the airway from oral secretions [2]. Aspiration pneumonia is frequently seen in patients with long-term tube feeding, suggesting it results from salivary aspiration in patients with chronic brain-injured patients [3]. Therefore, it is important to detect salivary aspiration for preventing pneumonia.
Videofluoroscopic swallowing study (VFSS) is the gold standard for evaluating swallowing difficulties [4]. VFSS can visualize the oropharyngeal and esophageal phases of swallowing and provide detailed information on the anatomy and physiology of swallowing [2]. However, it is challenging to diagnose aspiration pneumonia in chronic brain-injured patients because salivary aspiration is the least recognized form of aspiration and episodic phenomenon that cannot be detected by VFSS [5-8].
A radionuclide salivagram is a useful tool for detecting salivary aspiration. It uses the scintigraphic method and traces material in the respiratory tract or not. It is used mostly in children with cerebral palsy to evaluate swallowing difficulties as it is safe and does not require radiation exposure or adequate cooperation [9,10]. Although the salivagram is a sensitive test as reported in previous studies, it is not established as a formal test for detecting salivary aspiration [10-12].
Several studies have compared VFSS and salivagram. However, most have focused on children or heterogeneous disease groups. In addition, studies on chronic brain-injured patients with salivary aspiration are limited although these patients are commonly seen in a rehabilitation unit. Therefore, the aim of this study is to investigate the correlation between VFSS and radionuclide salivagram in chronic brain-injured patients with dysphagia.
MATERIALS AND METHODS
Subjects
This was a cross-sectional retrospective study of chronic brain-injured patients who had radionuclide salivagram and VFSS for detecting salivary aspiration from January 2013 to February 2020 at Seoul Medical Center rehabilitation unit. Characteristics of patients, findings of VFSS and salivagram and clinical factors were obtained from their medical records. The inclusion criteria were (1) adult patients (>18 years old) who had brain injury, (2) those whose disease duration was at least 3 months since brain injury. Exclusion criteria were (1) a previous history of brain lesion, (2) any underlying disease that could affect swallowing function, such as neurodegenerative disease (idiopathic Parkinson disease, Alzheimer dementia), brain tumors and epilepsy, (3) patients with more than 1-week interval between the salivagram and VFSS, and (4) those with insufficient medical records. This study was approved by the Institutional Review Board of Seoul Medical Center (No. 2020-04-036). Written informed consents were obtained.
Patients’ characteristics and clinical factors
To evaluate the correlation between VFSS and salivagram findings, patient characteristics such as age, sex, disease duration, types of impairment and lesion location were analyzed. Additionally, clinical factors such as Mini-Mental State Examination (MMSE), the Modified Barthel Index (MBI), the Functional Ambulatory Category (FAC), feeding method, the presence of tracheostomy were analyzed. History of pneumonia was investigated through a retrospective review of charts from 1 month before and after VFSS and salivagram. The criteria were the presence of symptoms (fever, cough or sputum), associated radiological evidence of aspiration pneumonia and use of antibiotics.
Videofluoroscopic swallowing study
VFSS was performed in a fluoroscopy room with the patients seated in an upright position. Dynamic fluoroscopic images were acquired with lateral and anteriorposterior views. Swallowed materials were comprised water, yogurt, boiled rice, and cookies mixed with barium sulfate (Solotop Suspension; Taejoon Pharm Co. Ltd., Seoul, Korea). The results were analyzed by two experienced rehabilitation medicine physicians.
Penetration-Aspiration Scale (PAS), an 8-point numerical scale, was used for qualitative evaluation of penetration or aspiration during VFSS [13]. In this study, negative aspiration was defined as a PAS of 1 to 5 while positive aspiration was greater than 5 [9,14] (Supplementary Table S1).
Functional Dysphagia Scale (FDS), a numerical scale, was utilized for the quantitative evaluation of dysphagia severity (from 0 to 100) [15], with a high score indicating poor oropharyngeal dysfunction. FDS has 11 parameters to indicate the swallowing function of the oral and pharyngeal phase. These parameters include lip closure, bolus formation, residue in oral cavity, oral transit time, triggering of pharyngeal swallowing, laryngeal elevation and epiglottic closure, nasal penetration, vallecular sinus residue, pyriform sinus residue, coating of the pharyngeal wall and pharyngeal transit time. All parameters were quantified using 3 mL thin liquid of diluted barium (Supplementary Table S2).
Radionuclide salivagram
Radionuclide salivagram was used to detect salivary aspiration by assessing radioactivity in trachea or not. One milliliter of diluted 99mTc-DTPA (technetium-99m labeled diethylenetriaminepentaacetic acid) was administrated under the tongue of patient in a supine position. Dynamic acquisition for posterior images was conducted for the first 10 minutes, followed by a delayed static acquisition for with anterior and posterior images at 0, 10, and 30 minutes. Images were taken by gamma camera (BrightView XCT Imaging System; Philips, Cleveland, OH, USA). These images were analyzed by experienced nuclear medicine physicians. Aspiration was defined as detectable radioactivity within the tracheobronchial tree.
Statistical analysis
All statistical analyses were performed using SPSS version 23.0 (IBM SPSS, Armonk, NY, USA). For comparison between groups, a Mann-Whitney test and Fisher exact test or Pearson chi-square test was used. A multivariate logistic regression analysis with forward stepwise selection was performed to identify statistically significant variables associated with aspiration of radionuclide salivagram. A receiver operating characteristic (ROC) curve was used to determine the reference value showing optimal sensitivity and specificity. A p-value less than 0.05 was considered statistically significant.
RESULTS
Patient characteristics
After screening 182 chronic brain-injured patients with dysphagia, a total of 124 patients were finally included. The patients were divided into two groups according to the presence of salivary aspiration on a salivagram. Sixty-nine patients (55.6%) were positive for salivary aspiration while 55 (44.4%) were negative. Patient characteristics are presented in Table 1. There were no significant differences in age, sex, disease duration, types of impairment and lesion location between two groups. Regarding functional state, there was no significant difference in MMSE, FAC, and MBI score either between the two groups (Table 2). Other clinical factors such as feeding method and presence of tracheotomy showed no significant difference between the two groups. However, the incidence of aspiration pneumonia was significantly higher in the positive group than in the negative salivagram group (p=0.013).
Dysphagia severity and characteristics
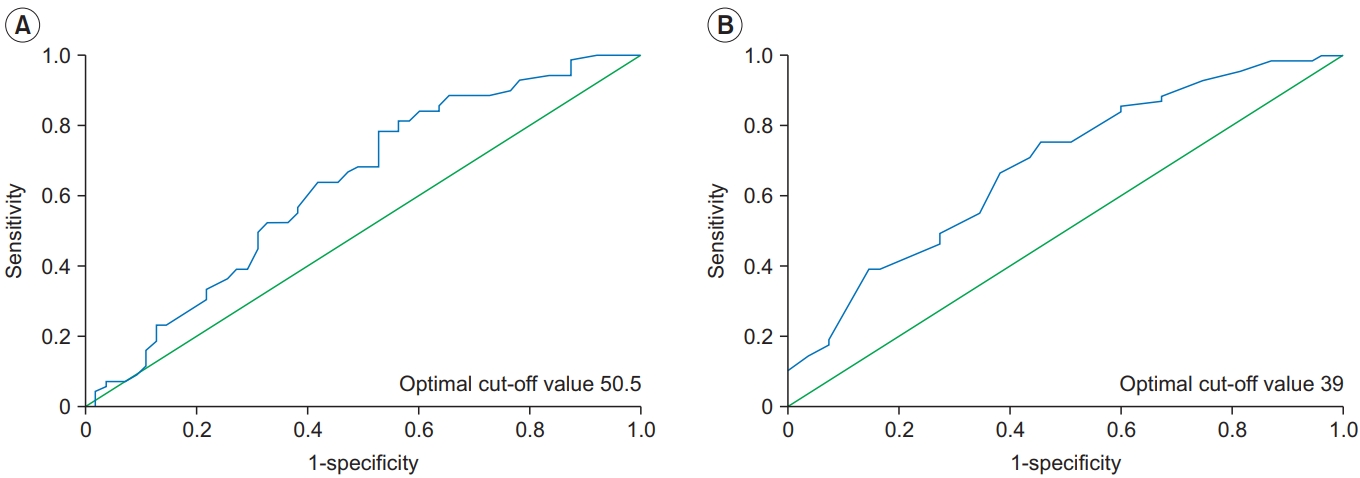
Dysphagia characteristics according to salivagram findings are summarized in Tables 3 and 4. There was statistical association between VFSS and salivagram (p=0.011). The total agreement between the two tests was 62% and the kappa value was 0.228. Statistically significant differences were observed for PAS as a qualitative evaluation (5.74±2.842 in positive finding vs. 4.11±3.071 in negative finding; p=0.004) and total FDS score indicating the severity of dysphagia (52.96±15.971 in positive finding vs. 44.45±19.433 in negative finding; p=0.013). There was a significant difference in FDS parameters such as triggering of pharyngeal swallowing (p=0.009), laryngeal elevation and epiglottic closure (p=0.008) and nasal penetration (p=0.026) between the two groups. The multivariate logistic regression analysis with the forward stepwise method demonstrated that laryngeal elevation and epiglottic closure in FDS parameters was significantly associated with positive findings on the salivagram (odds ratio=1.100; 95% confidence interval [CI], 1.017-1.190; p=0.018) (Table 5). In the ROC curve analysis, the area under the ROC curve (AUC) of total FDS and FDS in the pharyngeal phase for salivary aspiration on salivagram was 0.686 (95% CI, 0.530–0.730; p<0.013) and 0.630 (95% CI, 0.592–0.779; p<0.0001), respectively (Fig. 1). The optimal cut-off value for total FDS was 50.5 (sensitivity=56.5%, specificity=61.8%) and for FDS in the pharyngeal phase was 39 (sensitivity=55.1%, specificity=65.4%).
DISCUSSION
This study investigated the correlation between VFSS and salivagram findings in patients with chronic brain injury. There was no significant difference in patient characteristics or clinical factors between patients with positive findings of salivary aspiration on salivagram and those with negative findings. However, statistically significant differences were found in the swallowing functions, especially in airway protective mechanisms such as triggering of pharyngeal swallowing, laryngeal elevation and epiglottic closure and nasal penetration. According to the multivariate logistic regression analysis, laryngeal elevation and epiglottic closure of the FDS parameter was associated with salivary aspiration. Therefore, appropriate airway protective mechanisms are important as they are related to the occurrence of aspiration pneumonia in patients with chronic brain injury for preventing salivary aspiration.
VFSS and radionuclide salivagram are useful tools for detecting aspiration. In the present study, the total agreement was 62% and the kappa value was 0.228, although there was a statistical association between the two tests (p=0.011). The consistency was lower than expected, which is consistent with previous studies [9,10]. Possible explanations for these results are as follows. First, two tests assess different aspects of swallowing. In VFSS, the patients swallow bolus of food or fluid in an upright position, whereas salivagram is used for detecting small amount of saliva in a supine position which occurs spontaneously or reflexively, and not by voluntary swallowing as required for VFSS [16]. In addition, both tests have high rates of false negative because aspiration is an intermittent phenomenon [10]. Therefore, a combination of VFSS and salivagram have an increased the efficacy of predicting aspiration pneumonia.
Several studies have compared VFSS and salivagram. Kim et al. [9] found that, among 110 children with swallowing difficulty, 43.6% (48/110) of children had positive findings in VFSS whereas 30.3% (33/110) of children had positive findings in salivagram. Jang et al. [14] prospectively studied 50 patients with aspiration pneumonia. Aspiration was observed in 42% (21/50) of patients by VFSS and in 34% (17/50) of patients by salivagram [14]. In this study, of the total 124 patients with chronic brain injury, 58.1% (72/124) of patients showed positive findings in VFSS and 55.6% (69/124) of patients had positive findings in salivagram. The sensitivity of VFSS was higher than that of salivagram, consistent with previous studies [9,14]. However, the percentage of positive findings in salivagram in this study (55.6%) was higher than those in previous studies (30.3% and 34%, respectively). Possible explanations for these results are as follows. First, a salivagram has a long monitoring time in the supine position which is physiologically similar to salivary swallowing. Second, a patient with chronic brain injury is more susceptible to salivary aspiration due to poor function with immobilization and swallowing dysfunction. Thus, a salivagram is more valuable for detecting salivary aspiration in patients with chronic brain injury than for other groups.
Several studies have evaluated salivary aspiration in patients with brain lesions using radionuclide salivagram. Kang et al. [17] have reported the utility of salivagram in 32 bedridden patients with brain lesion. Sex, cooperation for the response of MMSE and anterior drooling were associated with positive salivagram findings. Park et al. [11] performed salivagram and VFSS in 35 patients with brain injury. The MMSE score was found to be related to positive salivagram findings. The cut-off value of MMSE was 7, suggesting that performing a salivagram could predict aspiration pneumonia in patients with cognitive impairment. Yu and Park [12] reported the clinical characteristics of salivagram findings in stroke patients with swallowing difficulty. The transfer sub-score of the MBI was significantly correlated with salivary aspiration in infratentorial stroke. In addition, MMSE score were a significantly correlated with salivary aspiration in supratentorial stroke. However, the findings of the current study were not consistent with those of previous studies as only swallowing functions among other clinical factors showed significant correlation with positive findings of salivagram in patients with chronic brain injury [11,12,17]. This discrepancy can be explained by disease the duration of the subjects. The present study focused on chronic patients in contrast to previous studies with a mean disease duration was 13.59 months (range, 3–64 months). In other words, they had a longer length of hospital stay and poorer functional state compared to that of patients from the other studies. In fact, only 11 patients (8%) were on oral feeding while 113 (92%) received tube feeding. One hundred patients (80%) underwent tracheostomy. Mean MMSE (7.23±9.140), MBI (10.49±14.728) and FAC (0.56±0.957) of this study were lower than those in previous studies [11,12,17].
Swallowing reflex is a part of the swallowing phase under involuntary control. It occurs when the bolus is passed from the posterior tongue through the hypopharynx to the upper esophageal sphincter. It involves mechanoreceptors innervated by the internal branch of the superior laryngeal nerve. These mechanoreceptors are activated by swallowing. They are connected to central neurons that generate swallowing [18]. The activation of these receptors results in breathing stops secondary to vocal fold adduction, anterior-superior movement of the hyoid bone and larynx and epiglottic posterior movement to close the trachea. These movements are important defense mechanisms against aspiration. Several studies have performed kinematic analysis using VFSS. Seo et al. [19] demonstrated that persistent aspiration could have resulted from delayed triggering of the swallowing reflex. Choi et al. [20] found that higher epiglottic folding angles were significantly associated with recovery of swallowing function in subacute stroke patients. In the present study, triggering of pharyngeal swallowing, laryngeal elevation and epiglottic closure and nasal penetration were significantly associated with salivary aspiration on the salivagram. Loss of these airway protective mechanisms can increase the risk of salivary aspiration and pneumonia. Therefore, it would be advantageous to perform a radionuclide salivagram in a patient showing abnormal values for these parameters on VFSS.
The present study has several limitations. First, it was designed as a retrospective study which might have introduced selection and recall bias. Second, the sample size was relatively small and the patients were heterogeneous in the types of brain lesions. Therefore, the results of this study are not sufficient to make a general conclusion. Third, this study focused on patients with chronic brain injury. Therefore, the results of this study cannot be applied to patients with acute or subacute brain injury. Finally, all parameters of VFSS were quantified by first swallowing of a thin liquid 3 mL and foods with various viscosities were not used in this study. Therefore, further prospective studies with single large samples are recommended to identify the clinical predictors of aspiration pneumonia in patients with chronic brain injury.
This study showed a correlation between salivagram and VFSS findings. Salivary aspiration is not related the functional status but with swallowing function in chronic brain-injured patients. In conclusion, performing a salivagram in patients with less than 39 FDS in the pharyngeal phase might be helpful in preventing aspiration pneumonia in chronic brain-injured patients.