INTRODUCTION
Cognitive impairment after stroke is an important factor affecting independent function and activity participation of patients, and dementia syndrome has been known to occur in approximately 8 to 26% of stroke patients within 12 months of the onset of stroke.1,2 In cases of severe cognitive impairment, it decreases morale and motivation to participate in an intensive rehabilitation program during the acute phase. It may also affect the ability to acquire motor skills, thus becoming the main cause of poor prognosis for rehabilitation. In addition, it may affect only one area of cognitive function, but in most cases, it is accompanied by impairment of the overall area of attention, concentration, memory, spatial processing skills, language, problem-solving skills, and planning skills. Therefore, accurate assessment of cognitive function and prompt initiation of treatment in the early stage is needed for successful rehabilitation.3-5
In the meantime, variable cognitive rehabilitation programs using computer technology have been developed for cognitive rehabilitation, and several studies on brain-injured patients have reported that computer-assisted cognitive therapy can be effective in treating cognitive disorders of various areas including memory, attention, spatial perception.6-9 Compared with conventional therapy, computer-assisted cognitive rehabilitation programs have the advantage in that patients can repeat themselves to learn, provide immediate feedback on the performance of patients, and adjust the difficulty level by selecting the appropriate program level for patients.
More recently, studies in the area of cognitive function using three-dimensional virtual reality (VR) programs have been actively conducted.10-13 Virtual reality has the advantage of being able to implement the specific cir cum stance or situation just like a real three-dimensional environment under a virtual environment using a computer and it can be performed regardless of physical disability using the unconstrained interface and minimizing the difference between laboratory environment and real life by interaction with the virtual environment. In particular, recently published studies have reported diagnosis of ambulatory navigational skill delay or reduced ability to perform activities of daily living through the virtual environment or improvement in memory or problem-solving skills through the virtual reality treatment for patients with dementia for whom cognitive decline was observed,14,15 patients with Parkinson's disease16 or elderly persons with mild cognitive impairment.17,18 However, whereas studies of cognitive function using virtual reality for stroke patients are mostly to assess unilateral neglect or overall cognitive impairment using the virtual reality program,19-22 there are relatively few studies to prove the effectiveness of virtual reality treatments for cognitive impairment.23 In particular, there is little research on the influence on cognitive function when computer-assisted cognitive rehabilitation and virtual reality training are performed at the same time, by comparison with when only computer-assisted cognitive rehabilitation is performed.
The aim of our study was to evaluate the influence on the recovery of cognitive function when the computer-assisted cognitive rehabilitation and the virtual reality training are performed together for acute stroke patients with cognitive impairment.
MATERIALS AND METHODS
Study subjects
Among patients diagnosed with stroke for the first time by magnetic resonance imaging and computerized tomography from July 1, 2009 to June 30, 2010, we recruited 28 patients who were stabilized neurologically and surgically after undergoing acute phase treatment at the Department of Neurology or Neurosurgery in our hospital and transferred to the Department of Rehabilitation Medicine for comprehensive rehabilitation treatment. All patients had cognitive impairment with a K-MMSE (Korean version of the Mini-Mental Status Examination) score range from 10 to 24. We excluded patients with a K-MMSE score of less than 10, patients presenting with severe cognitive impairment or aphasia and not being able to understand instructions, patients with poor sitting balance such that they could not sit on a chair with back and armrests, patients with limited range of motion of the neck due to orthopedic problems, and patients with loss of visual acuity such that they could not perceive content on a computer screen. Through random sampling, target patients were classified into two groups. One group was the VR group, which consisted of 15 patients who underwent virtual reality training and computer-assisted cognitive rehabilitation, and the other group was the control group, which consisted of 13 patients who underwent computer-assisted cognitive rehabilitation only. The average ages of the VR and control groups were 66.5 and 62.0 years old, respectively. The average stroke durations from stroke onset to the time of initial evaluation were 18.2 and 24.0 days, respectively. No statistically significant difference was observed in age, sex, duration from stroke onset to the time of initial evaluation, lesion location, number of patients with unilateral neglect, and K-MMSE score before treatment of the VR and control groups (Table 1).
Research methods
The VR group underwent both virtual reality training and computer-assisted cognitive rehabilitation together. Virtual reality training underwent a total of 30 minutes, 3 times a week, and computer-assisted cognitive rehabilitation underwent a total of 30 minutes, 2 times a week for a total of 5 times a week and 4 weeks. The control group underwent computer-assisted cognitive rehabilitation for a total of 30 minutes, 5 times a week, for a total of 4 weeks. All patients were treated with physical therapy and occupational therapy of the same intensity and time duration.
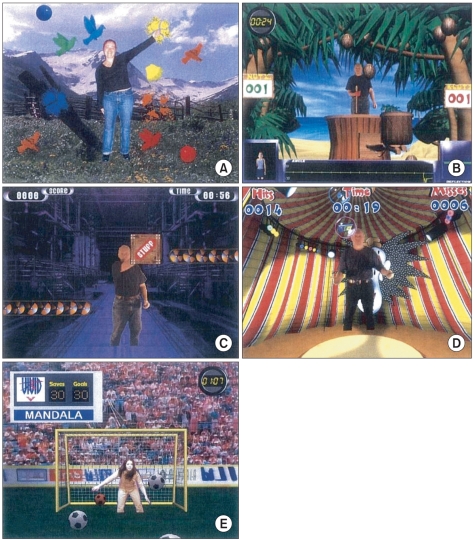
Virtual reality training was performed by one occupational therapist and IREX system® (Vivid group, Toronto, Canada) was used for the virtual reality system. Virtual reality environment consisted of television monitor, video camera, data gloves, and virtual objects (Fig. 1). A video camera recognized the movement or location of a patient and placed them in a virtual reality space, and data gloves recognized the motion of patients responding to virtual reality. We selected 5 out of a total of 20 virtual reality programs for our study. Four different programs were used for one time of virtual reality training, and the programs were correctly set up depending on the patient's condition. Each program was performed in 6 minutes, taking the 2-minute break between programs. Patients were mainly asked to move the affected upper extremity, but were allowed to use the unaffected upper extremity if their motor power was poor grade not being able to lift in themselves against gravity, and sometimes we allowed them to use both upper extremities depending on the program. In addition, since not all patients could be trained while standing, training was performed in the sitting position in a wheelchair. For patients who could not follow the instructions well, it was performed with verbal cues given by the therapist. The first program was called "Bird and Balls", in which balls appeared from various directions on the screen and the patient burst the balls with his/her hands to change them into birds. The second program was called "Coconuts", in which coconut fruits fell down from the top of the screen and the patient put them into a basket by moving his/her arms to the left or right. The third program was called "Conveyor", in which conveyor belts appeared on the left and right sides of the screen and the patient held the box coming from the conveyor belt in one side and moved it to the conveyor belt on the opposite side. The fourth program was called "Juggler", in which one or more balls came up on the screen at the same time, and the patient continued to hit the balls and move them upward to avoid dropping the balls on the ground. The fifth program was called "Soccer", in which a soccer ball came up on the screen and the patient stopped the ball from going in the goal with his/her hands by playing the role of a goalkeeper (Fig. 2). In all programs, the level of difficulty could be controlled by adjusting the velocity, quantity, distance and angle of the object provided by virtual reality depending on the patient's condition. After the end of each program, the screen displayed the score achieved by the patient to make it possible to obtain feedback. In addition, a variety of background music associated with the game was provided in each program.
Computer-assisted cognitive rehabilitation used Com Cog® (Maxmedica Inc., Seoul, Korea), which was composed of programs designed to promote attention and memory for patients with cognitive impairment. Attention program was divided into three types of courses, which included the beginner course, intermediate course and advanced course. Based on the complete learning method, the training level could be determined according to the difficulty of the task, and the program details consisted of basic visual perception training, auditory perception training, attention training, attention discrimination training, continuous attention training, attention integration training, and emotion training. Memory programs consisted of three kinds of training courses (beginner, intermediate and advanced) by combining verbal/non-verbal tasks and sequential/non-sequential tasks. It could be classified according to the level of difficulty in the same way as the attention program and the program details consisted of simple recognition memory training, simple spatial memory training, sequential recall memory training, sequential verbal recall memory training, associated recall memory training, verbal categorization memory training, and integrated memory training.
Evaluation methods
To evaluate cognitive function for all patients before treatment, we performed computerized neuropsychological test (CNT, MaxMedica)24 and Tower of London test (TOL).25
We performed CNT including visual & auditory continuous performance tests (CPT) to evaluate continuous concentration on visual and auditory stimulations, and word-color test to evaluate the selective attention, and we evaluated forward & backward digit span tests (DST) and verbal learning test for verbal memory evaluation tests. For the verbal learning test, after letting the patients hear 15 target words through the speaker, we scored the number of words they first recalled, the number of words they recalled after repeating the same target words five times, the number of words they recalled after 20 minutes, and the number of words they found after presenting on the screen a list of 30 words containing the previous 15 words. For the spatial memory test, forward and backward visual span tests (VST) and visual learning tests were performed. For the visual learning test, after presenting 15 different figures sequentially, and then showing 30 figures including 15 figures that were not presented and 15 figures that were previously presented, we scored the number of presented figures they first found, the number of figures they found after showing the same figures five times, the number of figures they found after 20 minutes, and the number of figures they found after showing all 30 figures on the screen. For the visual motor coordination test (Trail making test-type A), we evaluated the time taken to drawing lines connecting 25 small circles on the screen, containing numbers 1 to 25 in each small circle.
For Tower of London (TOL) test to assess executive functioning, 5 balls of different colors were put into each bar among a total of 3 bars and after the occupational therapist showed the final goal position of 5 balls evenly put into 3 bars, we measured the time taken to make the final goal position by moving the balls as little as possible.
We evaluated activities of daily living function using Korean-Modified Barthel Index (K-MBI), and also evaluated motor function using the Motricity Index (MI) for the assessment of upper and lower muscle strength of the affected side after stroke. After 4 weeks of rehabilitation treatment, we re-evaluated the above clinical examination items.
Statistical analysis
SPSS 14.0 was used for statistical analysis. We analyzed the changes of the described test items including the evaluation of cognitive function before and after treatment within VR and control groups using Wilcoxon signed rank test, and we compared the difference of above test items including the evaluation of cognitive function before and after treatment between the VR and control groups using Mann-Whitney test. For statistical significance, we used 95% confidence interval, p<0.05.
RESULTS
In the comparison of evaluation items including cognitive function, ability to perform activities of daily living and motor function between the two groups that were tested before treatment, no significant differences between the two groups were observed in all the test items, except for the K-MBI scores (50.1±20.3 vs 30.2±21.6, p=0.03), which were significantly higher in the VR group than in the control group.
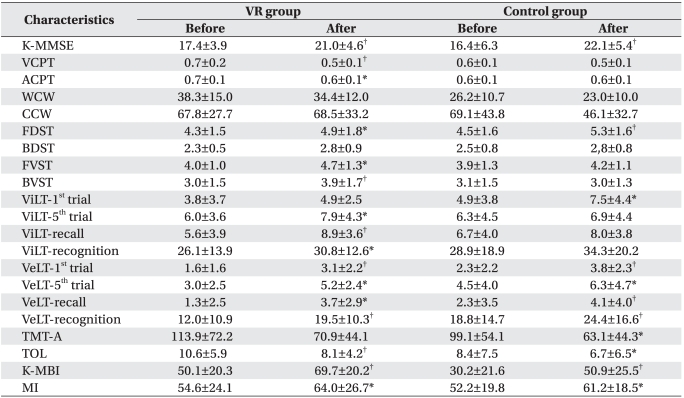
In the comparison of changes of cognitive function, ability to perform activities of daily living and motor function before and after treatment within the VR and control groups, among the K-MMSE, CNT items, visual and auditory CPTs, forward DST, forward and backward VSTs, and verbal and visual learning tests, TOL test, K-MBI, and MI scores showed statistically significant improvement in the VR group after treatment when compared with before treatment. In the control group, among the K-MMSE, CNT items, forward DST, visual and verbal learning tests, trail making test-type A, TOL test, K-MBI, and MI scores showed statistically significant improvement after treatment (Table 2).
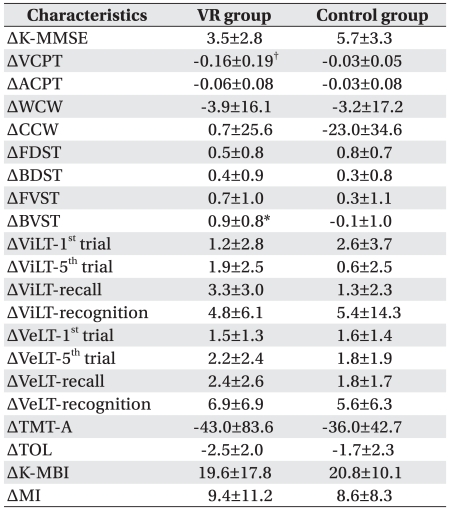
When comparing the differences of cognitive function, ability to perform activities of daily living and motor function before and after treatment between the VR and control groups, among the CNT items, visual CPT and backward VST showed significant improvement compared to the control group (Table 3).
DISCUSSION
In our study, we found that visual attention and short-term visuospatial memory showed significant improvement in the VR group compared to the control group for acute stroke patients with cognitive impairment. Ben-Yishay et al.26 reported that intact attention is required to use higher cognitive functions effectively and when the ability to pay attention and concentrate on the information given outside is impaired, memory, problem solving, and production of appropriate actions could be difficult. In other words, they suggested that the loss of attention due to brain injury could interfere with the recovery of other cognitive functions such as memory, executive function, and planning ability. This implies that the cognitive treatment for training and improvement of attention should be based and preceded in order to improve overall cognitive function for brain-injured patients with cognitive impairment. In this sense, it is very meaningful that the results of this study showed the improvement of visual attention and short-term visuospatial memory after treatment with the virtual reality program.
Considering the reasons why visual attention and short-term visuospatial memory significantly improved after virtual reality training: First, virtual reality program was conducted in the forms of the game that could induce motivation and interest of the patients, leading to the improvement of procedural memory and the reactivation of brain neurotransmitters. Therefore, it was likely to improve visual attention and short-term visuospatial memory finally. Rose et al.23 reported that among patients with vascular brain injury, the patient group that showed interests in virtual reality environment and actively participated in the program, presented significantly improved spatial awareness test scores, compared to the patient group who watched the program passively. Rose et al.23 explained that since there were many cases in which procedural memory was preserved even if there was brain injury, procedural memory would have been helpful to improve visuospatial memory during the active participation and devotion in virtual reality program. In addition, Kim et al.27 reported that if the patients were motivated by experiencing a diverse and stimulating environment through the virtual reality program, it would be able to result in the improvement of attention and memory by the reactivation of brain neurotransmitter capability such as cholinergic and dopaminergic systems when combined with cognitive treatment. Second, the screen backgrounds for the virtual reality used in our study were a natural environment such as mountains and fields, skiing resorts, soccer grounds suitable for each program, and by placing the patients in the stimulus-rich virtual backgrounds for visuospatial perception, their visuospatial perception abilities were likely to be improved. Several studies28,29 demonstrated that visuospatial learning ability improved significantly when treated with stimulus training of visuospatial perception through the virtual reality program in the form of game for patients with physical disability, compared with the patients not treated with virtual reality program. Third, it might be able to improve the patient's level of alertness and visual attention during the treatment by providing continuous visual stimulus through the dynamic screen along with various auditory stimulus such as background music offered in the virtual reality program. In fact, we found that visual attention as well as auditory attention showed significant improvement within the VR group before and after treatment. Kim et al.27 reported the results of attention and memory performance improvement after performing virtual reality program of cognitive function for the elderly. The previous study proposed an explainable mechanism that strong virtual reality stimulus (visual and auditory) and immersiveness enough to induce the user active cognitive activities have been involved in improvement of cognitive function.
In addition, our study showed significant improvement in verbal and visual learning tests reflecting relatively long-term memory as well as short-term memory and attention before and after treatment in the VR group. Patients in the VR group performed simple and repetitive motions primarily using shoulder flexion and abduction through the virtual reality program, and repetitive physical movements in such virtual reality was likely to improve cognitive function by increasing the activation of the brain responsible for cognitive functions. Fordyce and Farrar30 reported that continued treadmill exercise of rats brought improvements in visuospatial memory. Grealy et al.31 observed in their study that when various visual stimulus were given to patients with traumatic brain injury by experiencing bicycle riding by themselves in virtual reality, they showed significant improvement in digit symbol tests as well as visual and verbal learning tests. Grealy et al.31 suggested that an interactive exercise could be associated with improvement of functions in the hippocampal region and a relatively simple physical exercise could result in the improvement of learning ability by reducing the overload of attention through virtual reality. However, because the control group showed significant improvement in one item of visual learning test and verbal learning test, it may be difficult to conclude simply that it was therapeutic effects of virtual reality. In addition, a TOL test to assess planning ability showed significant improvement in both groups before and after treatment, and there are limitations to conclude that it was the effect of virtual reality only. In order to prove its effectiveness, it is considered necessary to compare the group treated only with virtual reality training and the group treated only with computer-assisted cognitive rehabilitation.
In our study, we did not observe significant improvement of ability to perform activities of daily living in patients treated with virtual reality, compared to other patients. We considered that repetitive movements of the shoulder are required in the virtual reality programs, but making fine motor movements of hand such as catching and moving things are usually required in the activities of daily living. Therefore, it may cause limitations that lead to functional improvement. In addition, the improvement in activities of daily living may not appear significant because there are many cases which need other cognitive functions such as planning ability, problem solving ability and working memory in everyday life.
Limitations of our study included not observing significant differences in the number of patients showing unilateral neglect between both groups before treatment. Nonetheless, we have not determined whether the improvement of visual attention and short-term visuospatial memory correlated with the improvement of unilateral neglect because we did not investigate whether the unilateral neglect improved after treatment. Of course, several studies22,32,33 reported the improvement of unilateral neglect through virtual reality training, but the virtual reality programs used in those studies reproduced the situations representing unilateral neglect by letting patients cross the virtual street or to respond to objects that appear in the direction of occurring unilateral neglect by using only the upper extremity. Thus, those programs are different from the contents of virtual reality program that is conducted in the form of game as shown in our study. Therefore, further research is needed to investigate the improvement of unilateral neglect by using the virtual reality programs used in our study. Second, as mentioned earlier, we failed to clarify the effectiveness of virtual reality treatment for long-term visual and verbal memory since the comparison with the group underwent virtual reality treatment only was not performed. However, because computer-assisted cognitive rehabilitation has been used widely for cognitive treatment of stroke patients with cognitive impairment, we could not perform only virtual reality treatment for these patients. Finally, we could not conduct a comparative study on the effectiveness of virtual reality treatment depending on lesion location of cerebral hemisphere, cerebral cortical or subcortical areas due to the small number of patients.
CONCLUSION
In our study, we found that stroke patients with cognitive impairment showed significant improvement of visual attention and short-term visuospatial memory when treated with computer-assisted cognitive rehabilitation and virtual reality training together, compared to the cases when treated with computer-assisted cognitive rehabilitation only. Thus, in clinical practice, the additional effect is expected for the improvement of cognitive function when treated with virtual reality therapy together with computer-assisted cognitive rehabilitation therapy for cognitive rehabilitation of stroke patients with cognitive impairment. In the future, further efforts will be needed to develop virtual reality programs and demonstrate their effectiveness for improvement in various cognitive areas including verbal memory, problem-solving ability, and planning ability as well as attention and short-term visuospatial memory.