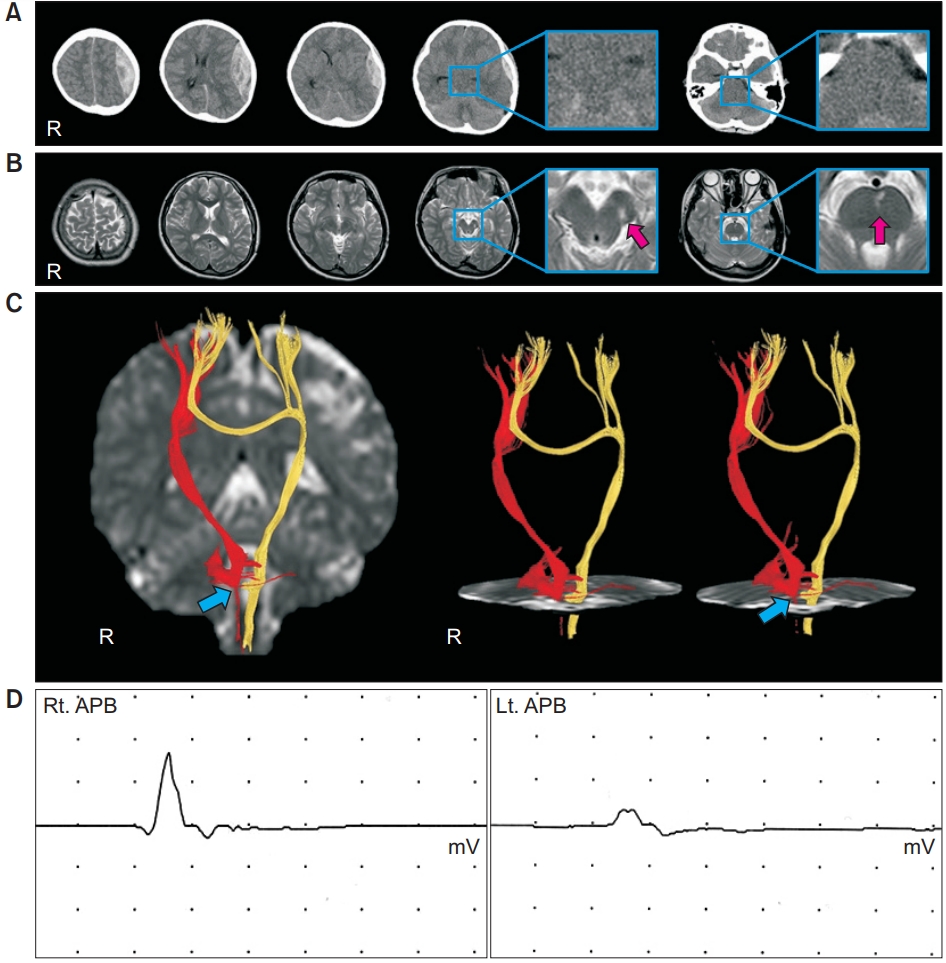
A 15-year-old right-handed female underwent craniectomy and removal of epidural hematoma (EDH) due to head trauma sustained as a result of falling while riding a bicycle. A brain computed tomography at onset showed an EDH on the left fronto-parieto-temporal lobes and subarachnoid hemorrhage (Fig. 1A). Brain magnetic resonance images 5 years after onset showed a leukomalactic lesion in the left subcortical white matter, left cerebral peduncle, and anterior center of the mid-pons (Fig. 1B). The patient showed mild hemiparesis in the left upper and lower extremities (manual muscle test, 4/5).
DTI data were acquired 5 years after onset using a 1.5T Philips Gyroscan Intera System (Philips Medical Systems, Cleveland, OH, USA). Fibers passing through two regions of interest at the upper and lower pons were selected for corticospinal tracts (CSTs): FA threshold >0.15, direction threshold <27° [1]. Both CSTs, originating from the cerebral cortex including the primary motor cortex, descended to the medullary pyramid through the normal CST pathway. However, drastic narrowing of the right CST, was observed at the lower pons level (Fig. 1C).
Transcranial magnetic stimulation (TMS) was performed 5 years after onset using a Magstim Novametrix 200 magnetic stimulator (Magstim Co. Ltd., Spring Gardens, Whitland, UK) with a 9-cm mean diameter circular coil. Motor-evoked potentials (MEPs) were obtained from both abductor pollicis brevis (APB) muscles in relaxed state. MEP obtained from the left APB showed lower amplitude and higher excitatory threshold (ET) (latency=21.0 ms, amplitude=0.7 mV, ET=80%) compared to those of the right APB (latency=19.9 ms, amplitude=2.0 mV, ET=60%) [2] (Fig. 1D).
In this study, the following three coinciding results were observed in terms of clinical features, DTT, and TMS in a patient with ipsilateral hemiparesis following EDH. (1) This patient presented with left hemiparesis, even though EDH was present in the left hemisphere. (2) On DTT, the right CST showed drastic narrowing at the lower pons level. And (3) the MEP obtained from the left APB showed low amplitude, delayed latency, and high ET compared with that of the right APB. As a result, the left hemiparesis in this patient appeared to be ascribed to partial injury of the right CST at the lower pons, due to downward compression by the left transtentorial herniation following the left EDH. Leukomalactic lesions on the left cerebral peduncle and anterior center of the pons, appeared to be additional evidence of this injury mechanism. Kernohan notch phenomenon is ipsilateral hemiplegia caused by compression of the contralateral cerebral peduncle against the tentorial edge by a supratentorial mass [3,4]. Consequently, injury of the right CST in this patient was not typical Kernohan notch phenomenon, but an injury by downward compression following transtentorial herniation because the right CST injury was detected in the lower pons level [3,4]. However, there is a limitation of this study should be considered. The patient didn’t exam the electromyography, so we could not confirm peripheral neuropathy such as cervical radiculopathy or myopathy. Therefore, further study using electromyography to check peripheral neuropathy is encouraged.