INTRODUCTION
Gait dysfunction is the most common problem in the pediatric rehabilitation field. Gait function is usually achieved between 12 and 14 months of age, and it consists of multiple components including neurological, mechanical, cognitive, and perceptual factors. However, the motor component is thought to be the most critical factor in gait function. The main motor pathways are classified as the corticospinal tract (CST, pyramidal tract) and non-CST tract (extrapyramidal tract). The CST is known to control voluntary movements of distal extremities, and it is known to be mainly related to fine motor skills [1]. On the other hand, gait function, which requires trunk control and leg movement, is less associated with the CST and is more associated with the corticoreticular tract (CRT) [2]. The CRT originates from the premotor cortex (PMC) and terminates in the pontomedullary reticular formation. Several previous studies using conventional magnetic resonance imaging (MRI), single positron emission tomography-computed tomography (PET-CT), functional MRI (fMRI), and transcranial magnetic stimulation (TMS) have reported a strong association of PMC injury with gait dysfunction. Since the PMC is the main origin site of the CRT, it is considered that the CRT is one of the main neural pathways responsible for gait function [3].
Recent developments in diffusion tensor tractography (DTT) have enabled three-dimensional visualization and evaluation of neural tracts at the subcortical level. In 2012, Yeo et al. [4] identified the CRT in the human brain using DTT and a few other studies have reported CRT injury in patients with stroke or traumatic brain injury (TBI) [5,6,7,8]. However, little is known about the CRT status and its relation to gait dysfunction in pediatric patients who show delayed development.
In this study, we report three cases of pediatric patients with gait dysfunction, showing the corresponding DTT results.
CASE REPORTS
Diffusion tensor imaging
All three patients showed no definite abnormal findings on conventional brain MRI which does not explain the hemiplegic symptom of patients. Therefore, diffusion tensor imaging (DTI) was performed. DTI data were obtained using a synergy-L Sensitivity Encoding (SENSE) 6-channel head coil on a 1.5-T Philips Gyroscan Intera system (Hoffmann-La Roche, Best, The Netherlands). We acquired 67 contiguous slices parallel to the anterior commissure-posterior commissure line. The imaging parameters used were as follows: matrix=128×128, field of view=221 mm×221 mm, echo time (TE)=76 ms, repetition time (TR)=10,726 ms, SENSE factor (parallel imaging reduction factor)=2; EPI factor=67 and b=1,000 s/mm2, NEX=1, and thickness=2.3 mm (acquired voxel size 1.73 mm×1.73 mm×2.3 mm).
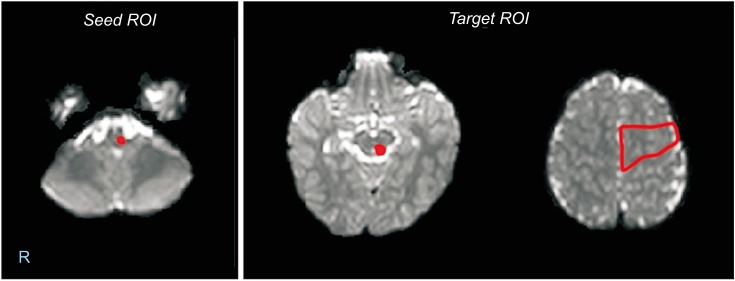
The Oxford Center for Functional Magnetic Resonance Image of the Brain (FMRIB) Software Library (FSL; http://www.fmrib.ox.ac.uk/fsl) was used to analyze diffusion-weighted imaging data. Fiber tracking was performed using a probabilistic tractography method based on a multi-fiber model, and it was applied utilizing tractography routines implemented in FMRIB diffusion (5,000 streamline samples, 0.5 mm step lengths, curvature thresholds=0.2). The CST and CRT were identified by selecting fibers passing through both regions of interest (ROIs). A seed ROI of the CST was placed on the CST portion of the anterior mid-pons on a 2D color map. Target ROIs of the CST were located on the CST portion of the anterior low-pons on a 2D color map. To reconstruct the CRT, a seed ROI was positioned on the reticular formation in the medulla. The first target ROI was positioned on the midbrain tegmentum and the second target ROI was positioned on the PMC (Brodmann area 6) (Fig. 1). Values of fractional anisotropy (FA) and tract volume (TV) of the reconstructed CST and CRT were measured.
Trunk Control Measurement Scale
The Trunk Control Measurement Scale (TCMS) [9] was used to assess trunk stability. Laterality of trunk instability was evaluated by assessment of each trunk side. Total scores ranged from 0 (lowest performance) to 58 (best performance). Scores of the right and left sides ranged from 0 to 19, respectively, but the other scores showed no left or right bias. The reliability and validity of the TCMS in pediatric patients has been demonstrated in several previous studies [9].
Three pediatric patients who showed gait dysfunction and six age- and sex-matched typically developing controls were recruited into this study. All control subjects were volunteers whose parents had applied for participation in this study and the study provided research funds to control subjects. Written informed consent was obtained from the parents of all participants and the study was approved by the Institutional Review Board at Yeungnam University Medical Center (IRB No. PCR-10-31). Demographic data and the functional data are summarized in Table 1. Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS) ver. 23.0 (IBM Corp., Armonk, NY, USA). Demographic data was compared between the two groups using the Mann-Whitney test. The level of statistical significance was set at p<0.05.
Case 1
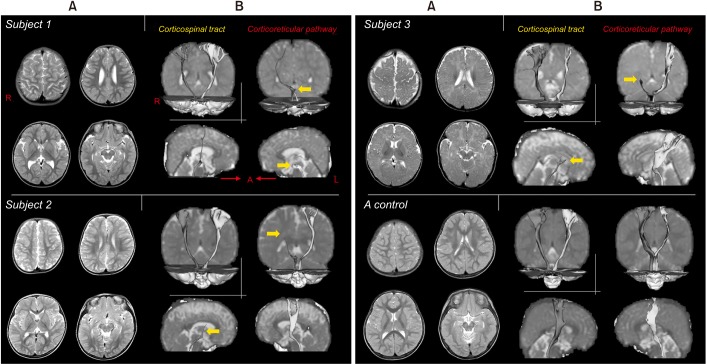
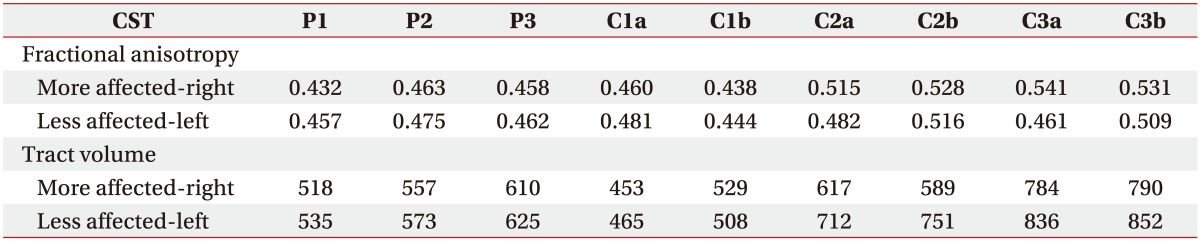
This patient was born at a gestational age of 40+2 weeks, and had a birth weight of 3.42 kg, and no specific perinatal history. He could not stand independently when he visited our clinic at the age of 19 months. With someone holding his hand, he could barely take a few steps and he showed prominent trunk sway. His mother stated that he could stand better when she held his right hand rather than his left hand, that he could barely maintain the sitting position with his hands on the bottom at 12 months of age, and that he could not stand without assistance until 18 months of age. His crawling was not well controlled and he showed an intermediate level of creeping (crawling and belly) and crawling, but the hemiplegic pattern was not observed. He showed no definite spasticity, weakness or sensory problem in his distal extremities, but he exhibited right-side trunk instability. He used his left hand predominantly but showed poor fine motor coordination skills of both hands. His TCMS scores for the right and left sides were 1 and 6, respectively (Table 1). His conventional brain MRI showed no definite abnormal lesion that could explain the unilateral proximal instability and gait dysfunction. Values of FA and TV of bilateral CSTs showed only a marginal difference from those in controls (Table 2) and the integrity of bilateral CSTs was preserved (Fig. 2). However, the left CRT showed disrupted integrity (Fig. 2). DTT result of bilateral CRTs showed decreased values of FA and TV compared to those in controls (Table 3). Other neural tracts involved in motor function such as the medial lemniscus and cerebellar peduncles were also analyzed and no abnormal findings were found.
Case 2
This patient was born at a gestational age of 39+4 weeks and had a birth weight of 3.14 kg. At the age of 22 months, the patient and his mother visited our rehabilitation department due to concerns about his delayed development. He could not walk independently despite his age. Interestingly, he could walk when his mother held his left hand, although he exhibited trunk sway. However, he was unable to walk when his mother held his right hand due to severe trunk instability. His mother described his delayed developmental milestones as follows: he could maintain the neck posture at the age of 5 to 6 months, and he could not stand alone until the age of 15 months. He did not have a specific hemiplegic pattern during crawling. His right and left side TCMS scores were 7 and 4, respectively (Table 1). DTT showed right CRT disruption (Fig. 2) and decreased values of FA and TV of bilateral CRTs compared to those in controls (Table 3). Bilateral CSTs showed preserved integrity (Fig. 2) and the values of FA and TV showed no definite difference from those in controls (Table 2). The medial lemniscus and cerebellar peduncles showed no abnormal findings.
Case 3
This male patient was referred to our rehabilitation department for delayed development at the age of 24 months. He was born at 41+0 weeks and had a birth weight of 3.6 kg. His parents described clinical manifestations which were similar to those of the second patient, i.e., he could only walk with left side assistance and showed no specific hemiplegic pattern during crawling. He showed right hand dominance, but, he had impaired fine motor coordination skills of both hands. In addition, he exhibited trunk instability even when standing while holding his mother's hand. Like the first patient, the second and third patients showed no spasticity or weakness of their distal extremities. His right and left TCMS scores were 7 and 5, respectively (Table 1). Like the first and second patients, the right CRT of the third patient showed disruption and the left CRT and bilateral CSTs showed no evidence of disruption (Fig. 2). DTT of bilateral CRTs, especially the right side, showed decreased values of FA and TV compared to those in controls (Table 3), but, the values of bilateral CSTs showed only a marginal difference from those in controls (Table 2). Similarly, the medial lemniscus and cerebellar tracts showed no definite abnormal findings explaining the patient's symptom.
DISCUSSION
Here, we report three cases of pediatric patients with gait dysfunction and trunk instability that appeared attributable to CRT disruption.
Several studies have reported CRT injury in patients with stroke or traumatic brain injury. In 2013, Yeo and Jang [5] reported that improvement of proximal and axial motor weakness was related to the recovery of an injured CRT in a patient with intracerebral hemorrhage. Furthermore, they concluded that proximal weakness in patients with traumatic brain injury is mainly due to CRT injury, rather than CST injury [6]. There was another DTT study in patients with cerebral infarct. Do et al. [7] recruited four hemiparetic patients with cerebral infarct who showed severe proximal weakness rather than distal weakness. In their DTT results, the affected CST showed preserved integrity in all patients. However, on the contrary, the affected CRT showed Wallerian degeneration in two patients and prominent disruption at the infarct level in the other two patients. In 2015, Lee and Jang [8] recruited 29 patients with proximal weakness following mild TBI and 25 control subjects. They showed that the TV of the CRT was significantly decreased in the patient group than in the control group. Similarly, in our patients, despite unilateral proximal weakness, there was no significant difference in CST parameters between right and left sides, or between patients and control subjects. However, the more affected CRT showed definite disruption and decreased DTI parameters compared to the less affected CRT, although conventional MRI showed no definite abnormal lesion. These results suggest that the CRT plays an important role in gait function and trunk stability, and that DTI could be helpful for assessment of the CRT in pediatric patients with gait dysfunction and trunk instability.
There are no published papers on the CRT problem in pediatric patients, and the cause of CRT disruption in pediatric patients has not yet been elucidated. There is one published paper on the normal maturation pattern of the CST and CRT using DTT. In 2014, Yeo et al. [10] investigated maturation of the CST and CRT in 75 normal healthy subjects ranging in age from 3 months to 25 years using DTI. In their study, all participants including infants, showed preserved integrity of the CST and CRT despite their young age. This indicates that disruption of the CRT in our patients cannot be considered a normal developmental process in the immature brain. Moreover, all patients included in our report showed unilateral disruption of the CRT. During normal development, neural tracts associated with motor function mature with symmetric integrity. The CRT is also a neural tract associated with motor function. Asymmetric integrity and unilateral disruption of the CRT in our patients seems difficult to be understood as a normal developmental process. Considering the absence of lesions on conventional brain MRI, the authors think that unilateral CRT disruption in our patients may be due to microstructural damage or pathological immaturity. Therefore, our results about the CRT are thought to have a meaningful relation with the pathological state of unilateral trunk instability.
However, several limitations of this study should be considered. Firstly, because the present study is essentially a case report, generalizability of its findings is limited. Another limitation is with respect to the TCMS measurement. In previous studies, TCMS was used in pediatric patients older than 5 years. The authors were aware of this fact; however, to the best of our knowledge, TCMS is the only measurement scale that enables assessment of unilateral trunk stability, and therefore, we used the TCMS. This is another limitation of this study. Evidently, large-scale studies with more detailed clinical evaluations are warranted.