INTRODUCTION
The number of people with disabilities is rapidly increasing in Korea. By December 2010, the Ministry of Health and Welfare registered 2,517,312 people as disabled [1]. The disabled population constructs 5.0% of the total population. Due to improvements in the living standard and public welfare system, the disabled population registered in Korean health care system is steadily increasing. The 96.5% of the total disabled population resides within communities [2]. Therefore, a community-based rehabilitation (CBR) strategy is receiving more attention as there is an increased demand for the healthcare of people with disabilities.
For an initial assessment of people with disabilities, measuring their functional ability and quality of life is important. These measurements are also necessary for goal setting as well as for evaluating the effect of medical treatment. To assess the health-related quality of life, a Medical Outcome Study 8-items Short-Form Health Survey (SF-8) was first used in Korea's CBR project. The ease and quickness of administration are the most attractive aspects of SF-8 [3]. In a previous survey for people with disabilities living in Goyang city, the average score was 36 [2]. However, SF-8 could not reflect the detailed quality of life because there were only a few numbers of questions regarding the psychological, social and environmental aspect. Moreover, the SF-8 is not translated and validated for use on the Korean population. For this reason, a new scale is necessary to assess the quality of life among people with disabilities.
The World Health Organization Quality of Life Assessment (WHOQOL) is a self-reporting multidimensional measure which is composed of six domains: physical, psychological, levels of independence, social relationship, environment, and spirituality [4,5]. The shorter version WHOQOL-BREF (the abbreviated version of WHOQOL instrument) was therefore developed in order to enable a brief but accurate assessment of the quality of life [6]. The WHOQOL-BREF contains one item from each of the 24 facets of the quality of life included in the WHOQOL-100, plus two 'benchmark' items from the general facet on the overall quality of life and general health [7-9].
The Korean version of WHOQOL-BREF was developed in 2002. The results suggest that the Korean version WHOQOL-BREF is valid and reliable for assessing the quality of life [6]. With this method, the issue of searching a new tool for assessing the quality of life among people with disabilities could be satisfied; Korean WHOQOL-BREF could be the substitute of SF-8.
The type of impairment is divided into four big sections: physical, sensory, mental (psychiatric), and intellectual. Chronic health conditions encountering difficulties in everyday life are also included in the boundary of disabilities [10,11]. Various segmented disability types are established by each government policy. There are fifteen types of disability in Korea, including internal organ impairment which is divided into six disability types.
We aim to search the usefulness of a new tool among people of various health conditions, such as stroke, traumatic brain injuries, amputees, spinal cord injuries, or other diverse physical impairment associated with musculoskeletal disorders. Such health conditions common in rehabilitation medicine unit could be broadly combined with the category of physical impairment. By subdividing, the physical impairment category would lead to a group of people who are registered with brain lesions or physical disabilities.
The aim of this study is to identify the validity and reliability of the Korean version WHOQOL-BREF among people with physical impairment living in communities.
MATERIALS AND METHODS
Procedure and subjects
Participants listed in the CBR project were recruited from 45 public health centers. People from randomized selected communities registered with brain lesions or physical disabilities were invited to complete our questionnaires. Respondents who had multiple disabilities related to physical impairment were included. Those excluded from the study were people with severe communication impairment who had difficulty completing the questionnaire despite assistance.
Subjects who agreed to participate in the study were requested to sign the consent form. The questionnaire was composed of questions related to health care status, satisfaction score, functional ability, and quality of life. The questionnaires were completed from November 15-26, 2009. A total of 994 respondents were initially included. With the exception of 244 respondents who had incomplete data, a statistical analysis was performed on the data of 750 respondents.
Measurement
Socio-economic personal information was obtained with regards to age, gender, marriage status, dwelling patterns, economic status, onset of impairment, and the type of registered disability.
For assessing the respondent's functional ability, the Korean version of Modified Barthel Index (K-MBI) was rated by health care providers working on the CBR project. The MBI consists of 10 items: personal hygiene, bathing, feeding, toileting, stair climbing, dressing, bowel control, bladder control, ambulation or wheelchair, and chair-bed transfer [12]. The item scores range from '0', which indicates an inability to perform, to a total score of 100, which indicates a complete independence in self-care performance [13].
MBI scores were divided into three groups, indicating the respondents' functional ability: 'total or severe dependence', 'moderate dependence', and 'slight or no dependence'. In the original Barthel Index, a total score of 0-20 suggests total dependence, 21-60 severe dependence, 61-90 moderate dependence, and 91-99 slight dependence [14]. However, this division has not been used widely in the MBI score system. A number of valued studies used different categories of disability on the Barthel Index [15-17]. After much consideration, we have decided to follow the Korean disability rating system standard of brain lesions, representing grade I-II, III-IV, and V-VI; each group indicates a MBI total score '0-53', '54-80', and '81-100'.
The WHOQOL-BREF is a 26-item generic questionnaire containing four domains: physical health, psychological, social relationships, and environmental. Each domain includes three to eight items [18]. The first item (Q1) asks the overall quality of life, and the second item (Q2) asks questions on general health satisfaction. Each item is based upon a self-report using a 5-point scale, which is applied in all questions. Respondents then check one of the following degrees.'not at all', 'a little', 'moderately', 'mostly', and 'completely' [6]. Higher scores indicate higher quality of life, with the exception of three negative forms which include pain and discomfort, need for medical treatment, and negative feelings [5]. Items proposed in negative form are calculated by subtracting the score form 6 [6].
Statistical analysis
Obtained data were analyzed using SPSS ver. 14.0 (SPSS Inc., Chicago, IL, USA). In order to assess the reliability, the internal consistency of each domain was calculated using Cronbach's Оұ. Instruments with Cronbach's Оұ value of 0.70 or greater are considered to have satisfactory internal consistency [18].
To examine the construct validity, intercorrelation between item-domain and factor analysis were conducted. Domain to domain and item to domain intercorrelation was analyzed by calculating Pearson product moment correlation coefficient. Correlations were interpreted as follows: 0.75вүӨrвүӨ1.0, good; 0.50вүӨr<0.75, moderate; 0.25вүӨr<0.50, fair; and 0.00вүӨr<0.25, slight or none [18]. Stepwise multiple regression analyses were conducted in order to determine which WHOQOL domains best predicted the overall quality of life (Q1) as well as the general health satisfaction (Q2). The exploratory factor analysis was used to identify the underlying variables that explain the pattern of correlation within the items and to examine the structure of WHOQOL-BREF. Leaving Q1 and Q2, 24 items underwent an exploratory factor analysis using the principle component method and orthogonal varimax rotation procedure. Factor loadings of 0.40 or above were interpreted as being meaningful. The extraction method was set up over eigenvalues >1.
RESULTS
Socio-demographic results
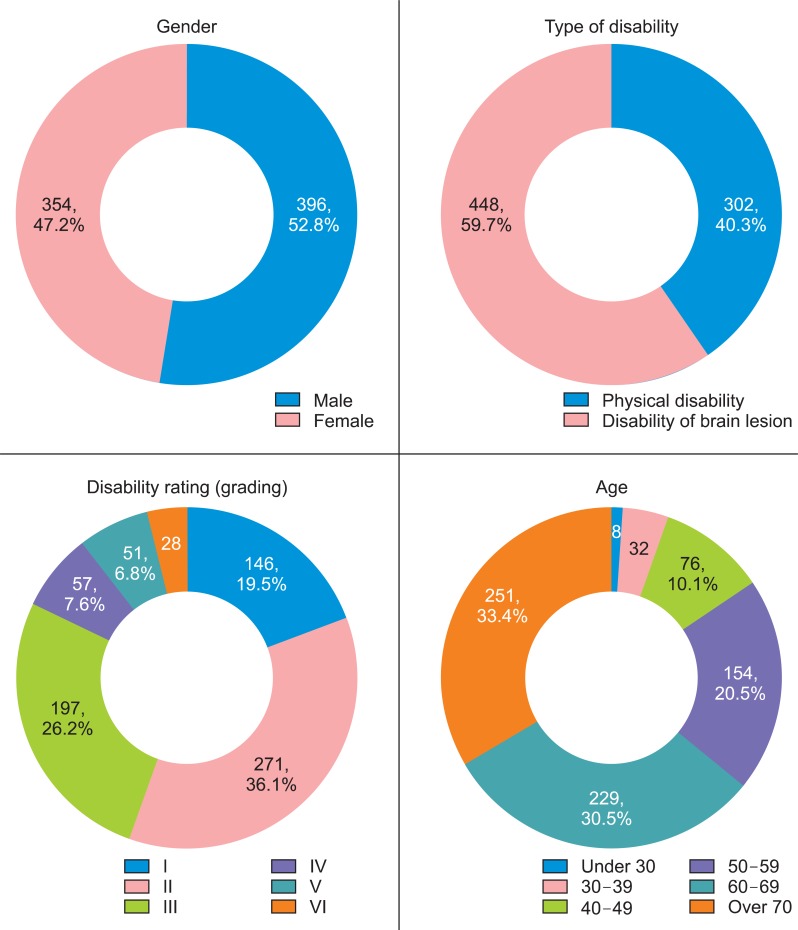
Analysis was conducted on a total of 750 individuals. Three hundred and ninety-six (52.8%) respondents were male, and the mean age was 62.4 years (range, 12.93 years). The number of each disability type was as follows: 448 (59.7%) people with brain lesions and 399 (40.3%) with physical disability. The 36.2% of the respondents were registered in grade II of a six-grade disability rating system, in which grade I indicates the most severe grade and grade VI relates to a mild disability determined by official standards (Fig. 1).
Internal consistency
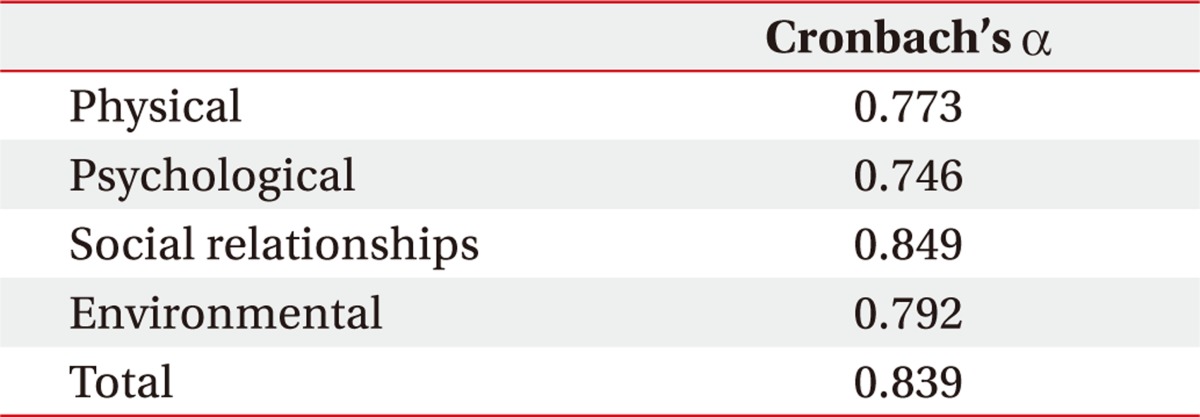
Cronbach's Оұ value for the total score was 0.839. The values for the physical, psychological, social relationships, and environmental domains were 0.773, 0.746, 0.849, and 0.792, respectively. The result reflects the acceptable internal consistency within all four domains (Table 1).
Construct validity
Domain to domain correlations
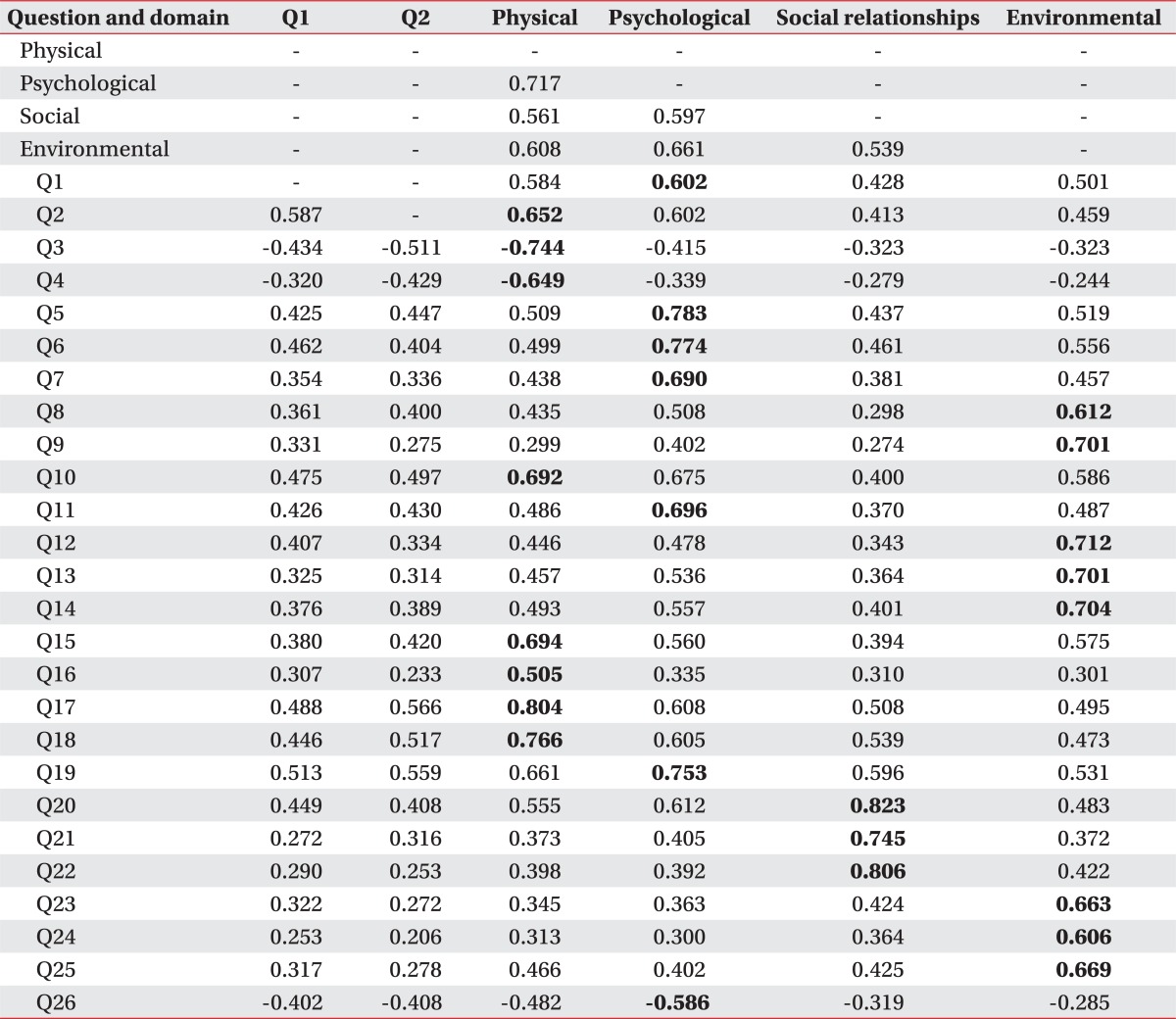
In the total sample, the correlation between each domain ranged from 0.539 to 0.717. All correlations were moderate; the highest correlation ranged between the psychological and physical domains (0.717) while the lowest correlation was between the social and physical domains (0.539) (Table 2).
Item to domain correlations
The item-domain correlation showed a significant correlation with their original domains (Table 2). Correlation coefficients for the physical domain ranged from 0.505 to 0.804, from 0.586 to 0.783 for the psychological domain, from 0.745 to 0.823 for the social domain, and from 0.606 to 0.712 for the environmental domain. Q1 correlated most strongly with the psychological domain and weekly correlated with the social and environmental domains. Q2 correlated most strongly with the physical domain.
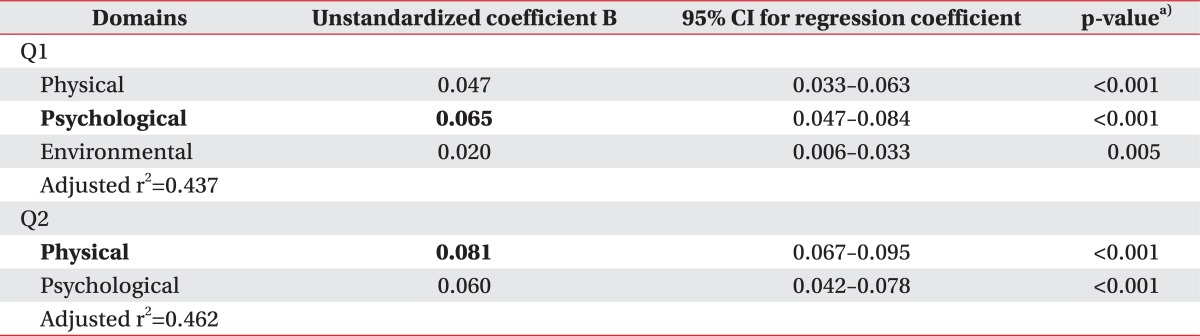
A multiple regression analysis of the domain scores with Q1 and Q2 was performed. As Q1 used for the dependent variable, the physical, psychological, and environmental domains were found to make a significant contribution. The psychological domain made the strongest contribution (unstandardized coefficient B=0.065). This variance accounted for 43.7% of the total variance of the overall quality of life. When Q2 was used for the dependent variable, the physical and psychological domains were found to make a significant contribution primarily with the physical domain (unstandardized coefficient B=0.081). The physical and psychological domains together explain 46.2% of the total variance for health satisfaction (Table 3).
Factor analysis
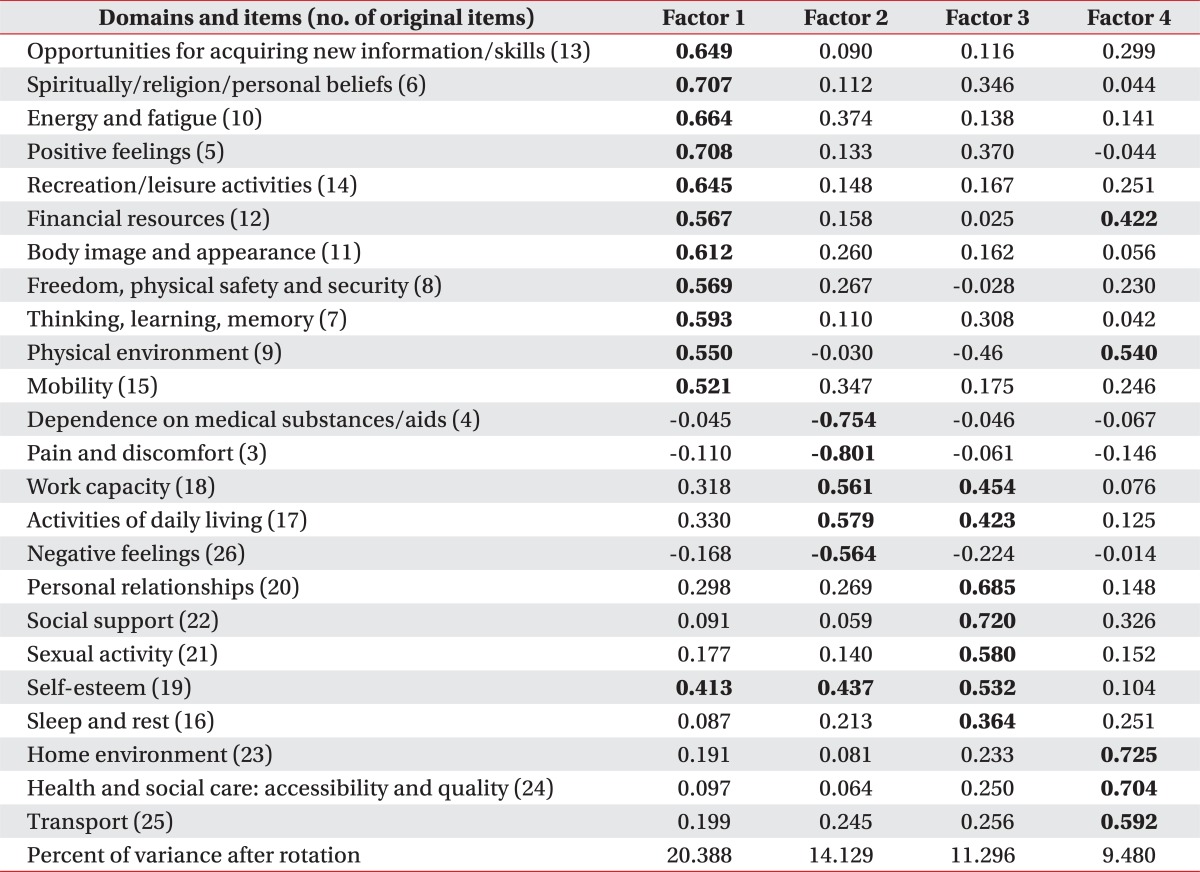
The exploratory factor analysis yielded four factors in the WHOQOL-BREF, accounting for 55.29% of the variability (Table 4).
Eleven items were loaded on the first factor, which explained 20.4% of the rotation variance. The first factor is considered to be a psychological component. Four items (Q5, Q6, Q7, and Q11) were originally included under the psychological domain, but five (Q8, Q9, Q12, Q13, and Q14) were in the environmental domain, and two (Q10, Q15) were in the physical domain. However, considering that the factor loaded above 0.40 were interpreted as being significant, item numbers 9 and 12 also could be cross-loaded in their original domains.
Five items were loaded on the second factor with 14.1% of rotation variance. The second factor is considered to be a physical component. Four items (Q3, Q4, Q17, and Q18) were originally included under the physical domain, but item number 26 was originally in the psychological domain.
The third factor represents the social component, in which five items were loaded, explaining 11.3% of the rotation variance. Three (Q20, Q21, and Q22) items were originally included in the social domain. Item number 19 was originally in the psychological domain and also demonstrated a significant result (0.413, 0.437) with the first and second factors. Item number 16, originally in the physical domain, showed a weaker loading which was not significant with all of the four factors, but had a trend of relation with the third factor.
The last factor accounted for 9.5% of the rotation variance; three items were loaded, and all of them originally represented the environmental components.
The total cumulative variance explained by these four factors was 55.29%.
Discriminant validity
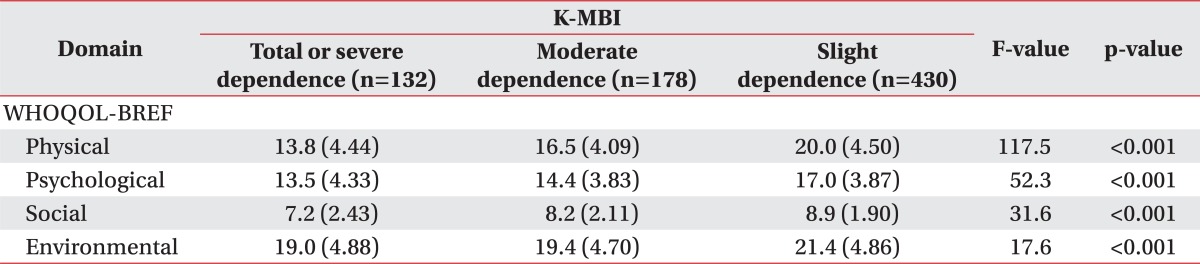
For exploring the discriminant validity, a comparison of each domain utilizing the respondent's functional ability was performed. The MBI was divided into three groups in degrees of 'total or severe dependence', 'moderate dependence', and 'slight or no dependence'; indicating an MBI score of '0-53', '54-80', and '81-100', respectively. The variance analysis (Table 5) indicated that there were highly significant changes across the MBI groups with the WHOQOL-BREF domains (p<0.001). This represents that if the functional independency is higher the quality of life is also good. This trend is also observed among all four domains of WHOQOL-BREF.
DISCUSSION
The aim of this study is to investigate the validity and reliability of the Korean version WHOQOL-BREF in people with physical impairment. The results of our study revealed that WHOQOL-BREF is valid and reliable in this group. It has good internal consistency, construct validity as well as discriminant validity.
Cronbach's Оұ value used for assessing internal consistency showed high scores in the range of 0.746 to 0.849 for each domain. These values are comparable with the previous study of the Korean version study of WHOQOL-BREF, which indicated a range of 0.584 to 0.777, implying that the social domain reveals relatively low values [6].
The construct validity was significantly high, showing that the domain to domain correlation of range was 0.539 to 0.717. However, even if the domains are highly related, the correlation coefficients are not so high as to suggest that the domains are measuring the same concept. As also expected, this could explain the variance between the four domains [22].
Further, all individual items were best correlated with their conceptual original domains. The overall quality of life mostly contributed to the psychological domain, whereas health satisfaction primarily contributed to the physical domain. These are different results compared to the Korean version WHOQOL and WHOQOL-BREF study conducted in healthy subjects and medical patients. In the previous study, the physical domain came out to be the largest contributor in the overall quality of life [6]. However, the study of Polish and Norwegian participants showed a similar result to this study for the main contributing factor [20,22]. In summary, the physical and psychological domains can explain the participant's quality of life and health satisfaction better than the environmental and social domains.
For the comparison of each domain score with the functional ability measured by MBI, the discrimination validity meant a higher MBI score correlated with a higher WHOQOL-BREF. These results demonstrate that WHOQOL-BREF scores are highly responsive to the clinical condition of the respondent's functional ability and can distinguish well between them. This result is also supported by the previous result in the disease group of dementia or traumatic brain injury [23,24]. Our study could also be meaningful in that the self-recorded WHOQOL-BREF strongly correlates with the functional ability rated by health care providers.
As part of the construct validation, the exploratory factory analysis (EFA) of the total sample was conducted. Four factors were detected, explaining 55.29% of the total cumulative variance. Ten items were included as different factors from their original domain. Among the ten items, 'financial resources', 'physical environment', and 'self-esteem' were cross-loaded on the original domain. It is worthy to note that eleven items were loaded on the psychological component. 'Opportunities for acquiring new information/skills', 'recreation/leisure activities', 'financial resources', 'freedom, physical safety and security', and 'physical environment' were originally included in the environmental domain and 'energy and fatigue' and 'mobility' were originally included in the physical domain. The 'sleep and rest' item was not significantly loaded on any factor, but had the highest loading in the social domain.
Although the previous Korean version study of WHOQOL-BREF did not perform EFA, similar studies conducted in other countries revealed various EFA results. The concomitant feature of the previous study was that even if the study was performed on the general population or specific disease entity, the WHOQOL-BREF has a four-factor solution [9]. In the previous study of Taiwan, which searched the quality of life of traumatic spinal cord injury using WHOQOL-BREF, ten items showed correlations with other domains [19]. In a Norwegian WHOQOL-BREF study among 4,000 respondents, seven items were shown to have multicollinearity effects, indicating an overlapping of content structure, particularly in the psychological and environmental domains [22].
The result of the factor analysis could be explained with the Korean socio-cultural background. Considering the respondents of our study were people with disabilities living in communities, the psychological property coming from the environmental and physical aspects would be maximized. The social attitudes of poor understanding of disability and developing social welfare system could have a relation as to why the five environmental factors were included in the psychological domain in this study. This cross-cultural variance was also suggested in a previous study of the Korean version WHOQOL-BREF, interpreting that the reason of social, independence and spiritual domains was found to be less important [6]. Consequently, it could carefully suggest that the expansion of the Korean social-welfare system on financial support, environmental improvement, safety and opportunity for social activity could influence the psychological aspect of quality of life in people with physical impairment.
Study limitation
The selection of the subjects has several limitations in this study. There might be a selection bias in that the recruitment was conducted by the CBR project. Lack of stratification in socio-demographic variances exists, especially in the ratio between physical disability and brain lesion. Response bias could also reflect the findings because the data is based on self-reported questionnaires; moreover, testing the retest reliability is absent. Considering the subjects were those with registered disability in the chronic stage, further study is needed, including a study on physically impaired patients in the acute and subacute stages.
The EFA revealed the necessity for further confirmatory factor analysis. To verify construct validity, the previous study of the Korean WHOQOL-BREF in the general population conducted confirmatory factor analysis. Due to different statistical methods, it is difficult to compare the pervious data with this study.
Despite these limitations, this study has significance as the first study of registered disability, not limiting the subjects in a particular disease. In this study, the Korean WHOQOL-BREF was valid and reliable in people with physical impairment. This could be a significant pilot study for a further well-designed and stratified study about people with such disabilities.
The large sample size could be the strength of this study. Considering the known ratio of each health condition [25], the outcome could be carefully applied in physical impairments related with stroke, musculoskeletal disorder, fractures, brain injury, and osteoarthritis.
In conclusion, the Korean WHOQOL-BREF is valid and reliable to measure the quality of life with good internal consistency, construct validity and discriminant validity among people with physical impairments living in a community. WHOQOL-BREF demonstrated higher internal consistency than that in the general Korean population. The overall quality of life was mostly related to the psychological domain, and health satisfaction mainly contributed to the physical domain. The item-domain correlation and exploratory factor analysis showed a structural similarity with the original 4-domain model. Higher functional independency rated by MBI correlated well with the WHOQOL-BREF. These results indicate that this questionnaire could be useful in assessing the quality of life in Korean people who are registered with physical disability or disabilities associated with brain lesions.