INTRODUCTION
The causes of intoeing gait include metatarsus adductus, internal tibial torsion, and internal femoral torsion, among which internal tibial torsion is known as the most common cause of intoeing gait.1 Tibial torsion is defined as the relationship between the axis of rotation of the knee and the transmalleolar axis.2 The indirect methods used to measure the value include physical examination of the patient's leg and radiological measurement methods such as simple X-ray, computed tomography (CT), nuclear magnetic resonance, ultrasonography, and fluoroscopy.3 During physical examination, the thigh foot angle (TFA) and bimalleolar angle (BMA) are commonly measured.2,4-6 However, the accuracy of physical examination has not been proven.7 On the contrary, the accuracy of CT was verified through a cadaver study,8 and thus most of the studies conducted until now have been to investigate the correlation between physical examination and CT. However, the two measurement methods showed a low correlation and the reliability and reproducibility of CT were superior,5,8 which was also verified in domestic studies.4,9 Other radiological methods including nuclear magnetic resonance and unltrasonography were suggested but these are also limited because the validity was acquired on the basis of the correlation with CT. Additionally, the recent development of medical imaging allows three dimensional computed tomography reconstruction (3D-CT). Studies were conducted on the reliability and accuracy of 3D-CT with respect to internal femoral torsion but not with respect to the tibial torsion.
Therefore, we proposed a new method to measure the tibial torsion angle using 3D-CT and evaluated the reliability of the method.
MATERIALS AND METHODS
Subjects
The subjects of this study were 33 infants who visited our hospital with the main complaint of intoeing gait and volunteered to participate in the study. Two physiatrists who learned the method to measure the tibial torsion angle measured the tibial torsion angle by performing physical examination and by using 3D-CT. Among the 33 infants, 8 were males, 25 were females, and the mean age was 6.18±3.81 (Table 1).
Methods
Radiological method using 3D-CT
To measure the tibial torsion angle radiologically, the 3D-CT images were reconstructed. The distal reference axis was determined as the transmalleolar axis that connected the most protruding parts of the medial malleolus and lateral malleolus on the caudo-cranial view of 3D-CT. The proximal reference axis was determined as the following two axes on the cranio-caudal view: the transtibial axis that divides the tibial head into two and passes through the central region; and the posterior condylar axis that passes through the two most posterior joints on the tibial plateau. The angle between the distal reference axis and the proximal reference axis was measured as the tibial torsion angle (Fig. 1).
Two raters measured the left and right sides, having the transtibial axis and posterior condylar axis as the proximal reference axes (first session) and then the individual raters repeated the measurement in the order of patients different from the previous one, making the measurements of the first session and measurements by the other rater unknown (second session).
Clinical measurement
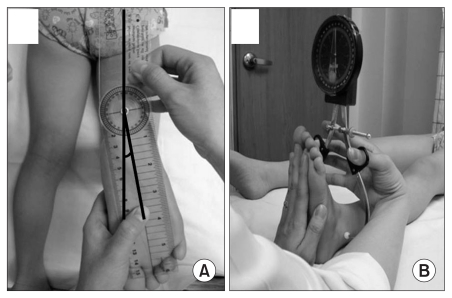
TFA measurement2,4,5: The patient was positioned prone, the knee flexed to 90°, and ankle positioned in neutral dorsiflexion/plantarflexion. The point where the heel is divided into two and the point where the forefoot is divided into two were marked. Then, the angle between the lines that connect these two points and the line that divides the thigh was measured on the horizontal plane using a goniometer.
BMA measurement6: The central points of the medial malleolus and lateral malleolus were marked with a pen. The patient was asked to be in the supine position, stretch the knee joint, and keep the feet in the neutral position. Then, the angle was measured by placing the two arms of a vertical goniometer at the central points between the medial malleolus and lateral malleolus (Fig. 2).
Two raters measured the left and right sides (first session) and then the individual raters repeated the measurements at the next follow up, making the measurements of the first session and the measurements by the other rater unknown (second session).
Statistical processing
The SPSS version 19.0 was used for statistical analysis. The inter-rater reliability and the intra-rater reliability of the tibial torsion angle measurement method were analyzed using the intraclass correlation coefficient (ICC). The correlation between the physical measurement and the 3D-CT measurement was analyzed using Pearson's correlation coefficient.
RESULTS
The descriptive statistics of the tibial torsion angle measured using 3D-CT
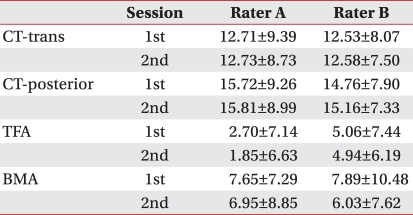
In the measurement performed by Rater A, the mean and standard deviation of the tibial torsion angle were 12.71±9.39° and 12.73±8.73° in the first and the second sessions, respectively, with reference to the transtibial axis as the proximal axis. The mean values were 15.72±9.26° and 15.81±8.99° in the first and the second sessions, respectively, with reference to the posterior condylar axis as the proximal axis. In the measurement performed by Rater B, the mean and standard deviation of the tibial torsion angle were 12.53±8.07° and 12.58±7.50° in the first and the second sessions, respectively, with reference to the transtibial axis as the proximal axis. The mean values were 14.76±7.90° and 15.16±7.33° in the first and the second sessions, respectively, with reference to the posterior condylar axis as the proximal axis (Table 2).
The inter-rater reliability and intra-rater reliability of the tibial torsion angle measurement method using 3D-CT
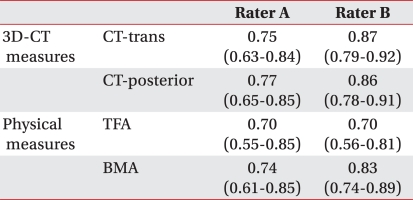
The correlation coefficient of the tibial torsion angle with reference to the transtibial axis between the first and the second session was 0.75 for Rater A and 0.87 for Rater B. In that case, the correlation coefficient between Raters A and B was 0.69. The correlation coefficient of the tibial torsion angle with reference to the posterior condylar axis between the first and the second session was 0.77 for Rater A and 0.86 for Rater B. In that case, the correlation coefficient between Raters A and B was 0.71 (Table 3, 4).
The descriptive statistics of the tibial torsion angle measured by physical examination by the individual raters
In the measurement performed by Rater A, the mean and standard deviation of the TFA value were 2.70±7.14° and 1.85±6.63° in the first and the second sessions, respectively. The mean BMA values were 7.65±7.29° and 6.95±8.85° in the first and the second sessions, respectively. In the measurement performed by Rater B, the mean and standard deviation of the TFA value were 5.06±7.44° and 4.94±6.19° in the first and the second sessions, respectively. The mean BMA values were 7.89±10.48° and 6.03±7.62° in the first and the second sessions, respectively (Table 2).
The inter-rater reliability and intra-rater reliability of the tibial torsion angle measurement method using physical examination
The correlation coefficients of the TFA and BMA values between the first and the second sessions were 0.70 and 0.74, respectively, by Rater A, and those of Rater B were 0.70 and 0.83, respectively. The correlation coefficient of the TFA and BMA values between Raters A and B were 0.25 and 0.02 (Table 3, 4).
DISCUSSION
Infants may show intoeing gait normally during the growth and development process, which is improved naturally in most cases.2 If continued, however, it may result in cosmetic, functional, and psychologic problems, and if serious, may cause degenerative arthritis or chondromalacia patella.10 Thus, treatment of tibial torsion, the most common cause of intoeing gait, is very important and should be based on accurate diagnosis. Various methods of physical examination and radiologic measurement have been applied to measure the tibial torsion angle.4-6,8,9,11-13
Among these methods, physical examination is most commonly used in clinics. However, in a cadaver study that investigated the accuracy of physical examination, significant difference was verified with direct measurement.7 Studies on the correlation with CT also showed that the correlation was not very high. For example, Lee et al.9 found a mild correlation coefficient between physical examination and the two-dimensional computed tomography (2D-CT) in 18 children with cerebral palsy. Stuberg et al.5 also verified the significant difference between the two measurement methods in 17 normal subjects.
Because of the limitations of physical examination, studies on radiological evaluation methods are still conducted. For example, 2D-CT is widely used as the method to measure the tibial torsion angle because a relatively high accuracy was verified in cadaver studies.8,13 Although the recent development of medical imaging allows 3D-CT, the reliability and accuracy of 3D-CT with respect to the tibial torsion angle measurement have not been investigated.
We assumed that the conventional two-dimensional measurement methods had a fundamental limitation in measuring the tibial torsion, because the tibia is a three-dimensional structure. Additionally, the excellent accuracy of 3D-CT for internal femoral torsion was verified already.14,15 Thus, we presumed that the application of 3D-CT to the measurement of internal tibial torsion would be more accurate.
Therefore, we conducted this study to suggest the application of 3D-CT, not 2D-CT, as a method to measure the tibial torsion angle. Because the reliability and accuracy should be high for a measurement method to be widely used, this study primarily focused on whether the reliability of the method could be verified clinically. The results showed a high intra-rater reliability and interrater reliability of the 3D-CT measurement method, indicating that it can be a useful tool for diagnosis and follow-up. On the contrary, physical examination of tibial torsion showed a low level of inter-rater reliability even though the intra-rater reliability was high. In other words, physical examination cannot provide objective information because the measurement result is greatly dependent upon the raters and the measurement methods, except for the continuous follow-up of the same infant patient by the same rater.
Moreover, the choice of the reference axis should be taken into account when applying the 3D-CT measurement method. To confirm the argument, Eckhoff and Johnson3 conducted a cadaver study comparing the 3D-CT measurement values of the cases where the transtibial axis, posterior condylar axis, and anterior condylar axis were chosen as the proximal reference axis The transtibial axis was defined as the bisector of the two lines that join the most anterior and posterior points on each half of the tibial plateau. The posterior condylar axis was defined as the line joining the two most posterior joints on the tibial plateau, which is the same as that of our study. The anterior condylar axis was defined as the line joining the most anterior points of each condyle or compartment of the tibial plateau. The comparison showed that the choice of proximal reference axis did not have a significant effect. Also, in our study, the results were compared for the cases where the transtibial axis and the posterior condylar axis were chosen, as they are chosen most widely as the proximal reference axes.3,8,13 The result showed that there was not a great difference in the reliability depending on the choice of proximal reference axis and the relation coefficient between the methods was as high as 0.86-0.93, indicating that the result was consistent with that of the previous studies.
In summary, the measurement of the tibial torsion angle based on 3D-CT is a very useful method because it has a high reliability and is not greatly dependent on the choice of the reference axis. However, the limitations of the method should not be overlooked. For example, CT may be of limited value in children because of the incomplete ossification and it has the disadvantages of radiological exposure and high cost.11,12
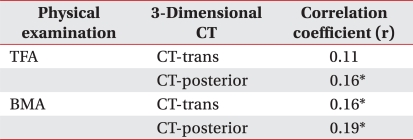
In conclusion, considering the advantages and limitation of the methods to measure the tibial torsion angle, we suggest that the 3D-CT method should be used for accurate diagnosis of internal tibial torsion, whereas physical examination by the same rater should be used for the follow-up in a short period of time for same patient. However, it is inappropriate to assess the progression by comparing the two values measured by different methods because the correlation between the two measurement methods is low.
Moreover, it may be needed to verify the accuracy of the 3D-CT method by means of direct measurement, which is impossible in clinical settings. Thus, a future study should be focused on the assessment of the accuracy of the 3D-CT method to measure the tibial torsion angle through direct measurement in cadaver study. In addition, it is necessary to present the normal tibial torsion angle values among normal infants measured by the 3D-CT method and clarify the standards for the diagnosis of internal tibial torsion.
CONCLUSION
The 3D-CT method to measure tibial torsion angle had higher intra-rater reliability (0.75-0.87) and inter-rater reliability (0.69-0.87) than those of physical examination. The 3D-CT method also has the advantage that the result is not dependent on the choice of the proximal reference axis. Therefore, the 3D-CT method can be useful for the diagnosis and follow-up of the infants who have intoeing gait.